


Percutaneous Closure of a Patent Foramen Ovale With a Gore Septal Occluder Device in a Young Woman
Indications
Patent foramen ovale (PFO) is implicated in cryptogenitic stroke, in transient ischemic attack (TIA), and in migraine in young adults. Therapeutic options differ regarding secondary prevention of stroke in patients with PFO. We report the case of a young woman with stroke and a history of migraine in the presence of a PFO treated by percoutaneous closure of the PFO with a new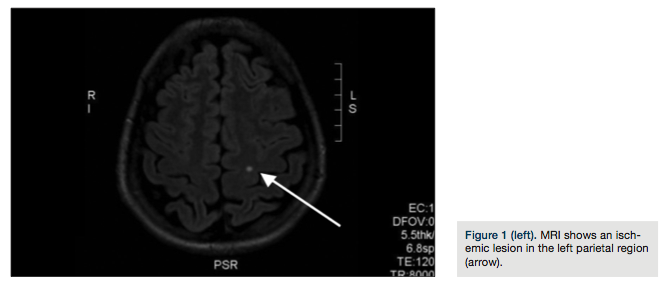 occluder device.
occluder device.
Case report
In August 2012, a 33-year-old woman was admitted to the emergency department of a local hospital due to paresthesias of the right side of the body and mental confusion. She underwent a cranial magnetic resonance (MRI) that showed an ischemic lesion in the left parietal region (Figure 1).
In order to determine the cause of her stroke, the patient was sent to the cardiology unit at INRCA Fermo. She is a non-smoker without a family history of cardiovascular disease. Her history did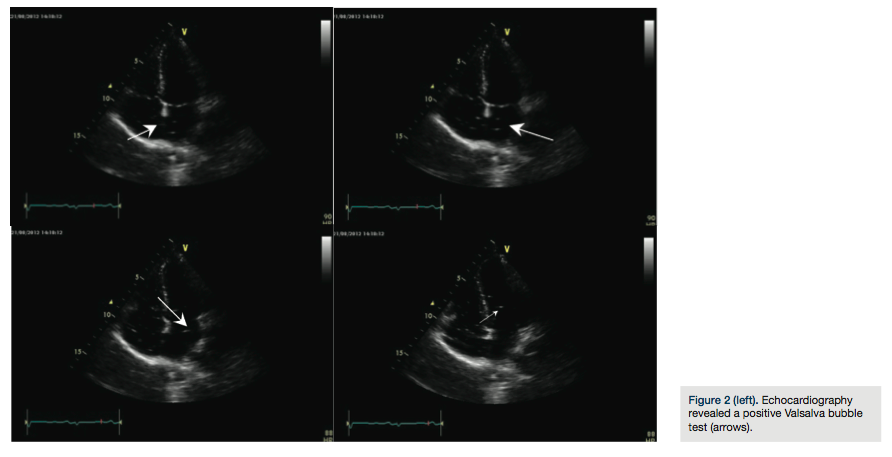 not show any anomalies, with the exception of recurrent typical migraine attacks with aura. Clinical examination showed that the young woman’s general physical condition was normal; resting ECG showed no irregularities. A two-dimensional color-flow echo Doppler scan of the neck vessels showed arteries free of atherosclerotic lesions. An echo Doppler study of the lower extremities was negative for thromboses. All laboratory test tests were normal. Transthoracic two-dimensional color Doppler echocardiography demostrated a patent foramen ovale and Chiari’s network; subsequent ecocontrast with agitated saline bubble contrast demostrated a right-to-left shunt of microbubbles at rest and following the Valsalva maneuver
not show any anomalies, with the exception of recurrent typical migraine attacks with aura. Clinical examination showed that the young woman’s general physical condition was normal; resting ECG showed no irregularities. A two-dimensional color-flow echo Doppler scan of the neck vessels showed arteries free of atherosclerotic lesions. An echo Doppler study of the lower extremities was negative for thromboses. All laboratory test tests were normal. Transthoracic two-dimensional color Doppler echocardiography demostrated a patent foramen ovale and Chiari’s network; subsequent ecocontrast with agitated saline bubble contrast demostrated a right-to-left shunt of microbubbles at rest and following the Valsalva maneuver (Figure 2). Transesophageal echocardiography confirmed a large PFO.
(Figure 2). Transesophageal echocardiography confirmed a large PFO.
The defect was closed using a Gore Septal Occluder (W. L. Gore & Associates) (Figure 3) at the Villa Maria Hospital of Cotignola. The procedure was performed under x-ray (Figure 4) and transesophageal echocardiography (TEE). In the TEE view, the PFO was interrogated, during the procedure, using a sizing ballon that showed a maximum diameter of 12 mm, and a 25 mm occluder was chosen. The correct position of the Gore Septal Occluder and complete PFO closure was seen via TEE.
The Gore Septal Occluder consists of a frame of five nickel-titanium wires configured to create a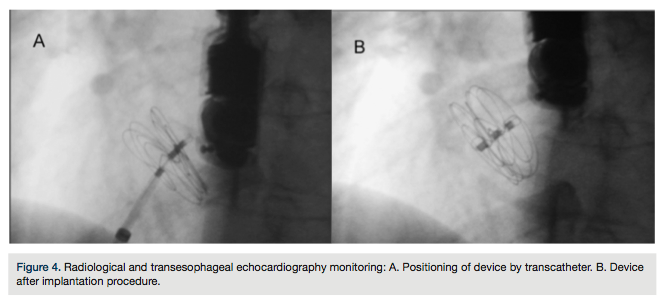 double-disk device. The occluder is submerged in heparinized saline and loaded into a delivery system. After placement of right femoral venous sheath, a guide wire was used to advance to the left atrium through the open foramen ovale and positioned in the upper left pulmnary vein; the Gore Septal Occluder was easily advanced through a 12 French delivery system to the left atrium. Once in the left atrium, first the left atrial disk and then the right atrial disk were released. When both disks were placed, the catheter was disconnected from the device. The patient tolerated the procedure well.
double-disk device. The occluder is submerged in heparinized saline and loaded into a delivery system. After placement of right femoral venous sheath, a guide wire was used to advance to the left atrium through the open foramen ovale and positioned in the upper left pulmnary vein; the Gore Septal Occluder was easily advanced through a 12 French delivery system to the left atrium. Once in the left atrium, first the left atrial disk and then the right atrial disk were released. When both disks were placed, the catheter was disconnected from the device. The patient tolerated the procedure well.
Transthoracic echocardiography the following day confirmed no residual shunt and correct position of device.
The patient was discharged on aspirin (100 mg/day) and clopidogrel (75 mg/day for three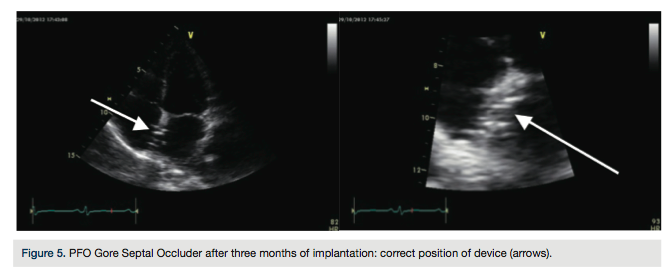 months). Follow-up echocardiogram at three months demostrated no residual shunt through the fenestretion and a well-positioned device (Figure 5). The patient remains free of other neurological events and migraine.
months). Follow-up echocardiogram at three months demostrated no residual shunt through the fenestretion and a well-positioned device (Figure 5). The patient remains free of other neurological events and migraine.
Discussion
Patent foramen ovale (PFO) is a residual element of the fetal circulation and is the most common defect of the heart.1,2 A PFO is an anomaly due to a leak in the fusion of the septum secundum and septum primum. In an autopsy study in a general population of 965 normal hearts, the prevalence of PFO was 27%.3 The importance of a PFO has long been discussed in the literature. A relationship between PFOs and several clinical conditions such as stroke and migraine has been documented.4,5 PFOs have also been linked to multiple atrial anatomical abnormalities such as atrial septal aneurysm and Chiari’s network. These coexisting abnormalities appear to increase the risk of stroke.6 The cause of stroke in a patient with a PFO is presumed to be paradoxical embolism. The optimum management to prevent paradoxical thromboembolic events remains controversial.7 Recently, few trials have been published.
CLOSURE-I is the first completed prospective, randomized PFO device closure study. Results showed no difference between percutaneous closure with a device (Starflex, NMT Medical, Inc.) and medical therapy alone in the prevention of recurrent stroke in patients with a PFO.8 Conversely, a study by Wahl et al9 showed that PFO closure perfomed better than medical treatment. In the RESPECT trial, PFO closure [with the Amplatzer Occluder device (St. Jude Medical)] reduced the risk of stroke in secondary prevention compared to medical management alone.10 The PC-Trial (also using the Amplatzer Occluder device) found closure of a PFO for secondary prevention of cryptogenic embolism did not result in a significant reduction in the risk of recurrent embolic events or death as compared with medical therapy.11 Other studies are in progress, such as the Gore REDUCE clinical study. There are currently several international and national guidelines on stroke prevention in patients with a PFO, but their claim on the best treatment strategy is unclear. Results of randomized trials are necessary to confirm the effectiveness of transcatheter closure of a PFO in patients with paradoxical thromboembolic events.
Conclusion
We report the case of a young woman who presented with cryptogenetic stroke. Transthoracic echcardiography revealed a residual PFO with a positive Valsalva bubble test. The patient underwent a percutaneus PFO closure with the Gore Septal Occluder. The procedure was performed under transesophageal echocardiography to guarantee proper sizing and position of the device. A number of devices are available for closure of PFOs. The Gore Septal Occluder consists of a frame of five nickel-titanium wires with a platinum core which is covered by a tube of expanded polytetrafluoroethylene film12 and is quickly endothelialized. The device is placed via standard femoral venous access. The benefits from its use seem to be easy and quick implantation, adaptability for a variety of atrial septal anomalies, and good tolerability without residual shunt.12 However, large-scale studies are needed to confirm the safety and efficacy of the device and especially to investigate possible late complications.
Disclosure: The authors report no conflicts of interest regarding the content herein.
This article received a double-blind peer review from members of the Cath Lab Digest Editorial Board.
The authors may be contacted via Dr. Luca Fallavollita, Italian National Research Institute on Aging-Fermo, Italy, at l.fallavollita@inrca.it.
References
- Ali Ebrahimi H, Hamzeaie Moghadam A, Aredestani E. Evaluation of patent foramen ovale in young adults with cryptogenic stroke. ARYA Atheroscler. 2011 Summer; 7(2): 74-77.
- Fuster V, Alexander RW, O’Rourke RA, et al. Hurst’s The Heart, 11th ed. New York: McGraw-Hill, Medical Publishing Division, 2004.
- Hagen PT, Scholt DG, Edwards WD. Incidence and size of PFO during the first decades of life: an autopsy study of 965 normal hearts. Mayo Clinicic Proc. 1984; 59: 17-20.
- Horton SC, Bunch TJ. Patent foramen ovale and stroke. Mayo Clin Proc. 2004 Jan; 79(1): 79-88.
- Wilmshurst PT. The persistent foramen ovale and migraine. Rev Neurol (Paris). 2005 Jul; 161(6-7): 671-674.
- Overell JR, Bone I, Lees KR. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology. 2000; 55: 1172-1179.
- Białkowski J, Wawrzyńczyk M, Karwot B, Fiszer R, Knop M, Szkutnik M. Medium-term results of transcatheter closure of patent foramen ovale with Amplatzer PFO and cribriform occluders. Kardiol Pol. 2012; 70(11): 1142-1146.
- Furlan AJ, Reisman M, Massaro J, Mauri L, Adams H, Albers GW, Felberg R, Herrmann H, Kar S, Landzberg M, Raizner A, Wechsler L; CLOSURE I Investigators. Closure or medical therapy for cryptogenic stroke with patent foramen ovale. N Engl J Med. 2012 Mar 15;366(11):991-9. doi: 10.1056/NEJMoa1009639.
- Wahl A, Jüni P, Mono ML, Kalesan B, Praz F, Geister L, Räber L, Nedeltchev K, Mattle HP, Windecker S, Meier B. Long-term propensity score-matched comparison of percutaneus closure of patent foramen ovale with medical treatment after paradoxicalembolism. Circulation. 2012; 125(6): 803-812.
- Carroll JD, Saver JL, Thaler DE, Smalling RW, Berry S, MacDonald LA, Marks DS, Tirschwell DL; RESPECT Investigators. Closure of patent foramen ovale versus medical therapy after cryptogenic stroke. N Engl J Med. 2013 Mar 21;368(12):1092-100. doi: 10.1056/NEJMoa1301440.
- Meier B, Kalesan B, Mattle HP, Khattab AA, Hildick-Smith D, Dudek D, et al. Percutaneous closure of patent foramen ovale in cryptogenic embolism. N Engl J Med. 2013 Mar 21;368(12):1083-91. doi: 10.1056/NEJMoa1211716.
- MacDonald ST, Daniels MJ, Ormerod OJ. Initial use of the new GORE(®) septal occluder in patent foramen ovale closure: implantation and preliminary results. Catheter Cardiovasc Interv. 2013 Mar;81(4):660-5. doi: 10.1002/ccd.24405.
