


PCI Indications (Freestyle)
 Medicare’s Recovery Audit Contractor (RAC) Initiative is an outsourcing effort in which contractors assess physician compliance with existing Medicare policy. Medicare gives the contractors authority to summon supporting documentation without cause. But Medicare does not permit contractors to make medical judgment decisions — the auditors must apply existing Medicare policy, as written and disseminated nationwide at https://www.cms.gov/medicare-coverage-database/overview-and-quick-search.aspx.
Medicare’s Recovery Audit Contractor (RAC) Initiative is an outsourcing effort in which contractors assess physician compliance with existing Medicare policy. Medicare gives the contractors authority to summon supporting documentation without cause. But Medicare does not permit contractors to make medical judgment decisions — the auditors must apply existing Medicare policy, as written and disseminated nationwide at https://www.cms.gov/medicare-coverage-database/overview-and-quick-search.aspx.
This Executive Overview of existing Medicare policy, specific to:
- Percutaneous coronary intervention (PCI)
- Dual chamber pacemakers
- Defibrillators
is “quintessential” reading for all cardiologists.
RAC audits are performed on a pre-payment basis for PCI, dual chamber pacemakers, and defibrillators in eleven states. Providers in all other states are audited on a post-payment basis — they will continue to be audited in this way until the pre-pay approach proves to be more cost effective; we anticipate nationwide proliferation of the pre-pay approach by around July 2012.
The standards contractors apply are easy to follow. But providers unfamiliar with the nuances of Medicare policy may face countless hours of administrative burden and thousands of dollars in legal fees to defend against allegations of performing unnecessary procedures. The nuances go a little something like this:
Medicare policy is actually quite rudimentary.
It is written for coders and billers, like me.
They don’t address things like the degree of occlusion;
they let the doctor define what is the best solution.
There are only two PCI policies on this occasion; they are from National Government Services and Wisconsin Physicians Service Insurance Corporation.
The standards are easy to meet; it’s almost impossible to fail.
You won’t pay two hundred dollars, or go directly to jail.
“Taking Care of the Patient” is the name of this game;
don’t be distracted by data from COURAGE or FAME.
You might be surprised at how much you really know,
after reviewing the “existing Medicare policies” in the table below.
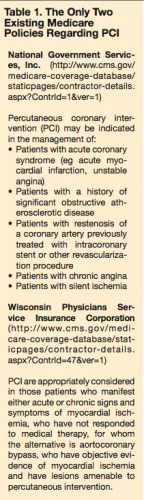 Table 1. The Only Two Existing Medicare Policies Regarding PCI
Table 1. The Only Two Existing Medicare Policies Regarding PCI
National Government Services, Inc. (https://www.cms.gov/medicare-coverage-database/staticpages/contractor-details.aspx?Contrid=1&ver=1)
Percutaneous coronary intervention (PCI) may be indicated in the management of:
- Patients with acute coronary syndrome (eg, acute myocardial infarction, unstable angina)
- Patients with a history of significant obstructive atherosclerotic disease
- Patients with restenosis of a coronary artery previously treated with intracoronary stent or other revascularization procedure
- Patients with chronic angina
- Patients with silent ischemia
Wisconsin Physicians Service Insurance Corporation (https://www.cms.gov/medicare-coverage-database/staticpages/contractor-details.aspx?Contrid=47&ver=1)
PCI are appropriately considered in those patients who manifest either acute or chronic signs and symptoms of myocardal ischemia, who have not responded to medical therapy, for whom the alternative is aortocoronary bypass, who have objective evidence of myocardial ischemia and have lesions amenable to percutaneous intervention.
Don’t even get me started on pacemakers, dude —
that policy hasn’t been updated since Brooke Shields went nude.
Our fault or theirs? Who is to say?
The policy is outdated, but it is still the audit standard today!
The rumors you’ve heard might not be in line
with the standards being used by auditors at this time.
You don’t need to say that pacemaker syndrome is waiting;
or that a drop in blood pressure was caused by ventricular pacing.
If your indication is based on medical wisdom,
the implant will be covered by the Medicare system.
This organization called “NICE” (National Institute for Clinical Health and Excellence) has a standard that’s great;
they call it a “Technology Appraisal” and they numbered it “88.”
They say heart block and a sinus syndrome that is sick
will justify a dual chamber pacemaker in the symptomatically bradycardic.
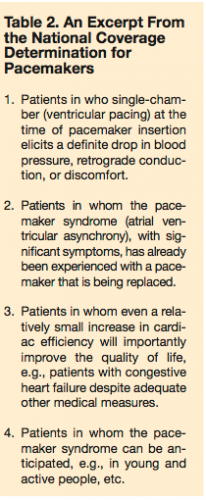
Table 2. An Excerpt From the National Coverage Determination for Pacemakers
- Patients in who single-chamber (ventricular pacing) at the time of pacemaker insertion elicits a definite drop in blood pressure, retrograde conduction, or discomfort.
- Patients in whom the pacemaker syndrome (atrial ventricular asynchrony), with significant symptoms, has already been experienced with a pacemaker that is being replaced.
- Patients in whom even a relatively small increase in cardiac efficiency will importantly improve the quality of life (eg, patients with congestive heart failure despite adequate other medical measures).
- Patients in whom the pacemaker syndrome can be anticipated (eg, in young and active people, etc.).
These conditions fit the coverage policy like a hand in a glove;
they are referenced as “new classes of patients,” and are a critical supplement to four other acceptable indications enumerated in the table (above).
The defibrillator policy is even more obscure;
its interpretation changes like the soup du jour.
You must wait forty days after the patient has an MI,
unless somebody angioplasties —
then you must let three months tick by.
The patient’s non-ischemic dilated cardiomyopathy must be three months old;
but the way this is explained is like the Da Vinci Code.
The indications above are true to the letter.
But read the coverage determinations yourself; as a source, they are much better.
Hopefully you’re more informed than before you started to read.
When you get audited, this perspective will help you, indeed.
Considering the value of your reputation,
you can see why the word “quintessential” was so quintessential in its prior application.
Final thoughts
The chasm that divides evidence-based standards and Medicare policy is being illuminated for the first time to many providers and auditors. Auditors assert that physicians are committing fraud and malpractice if they apply any standard other than those outlined in the existing Medicare coverage policies. These coverage policies desperately need to be updated.
CardiologyCoder.Com, a membership organization for coders in the cardiology field, has launched a campaign intended to “Narrow The Gap” between evidence-based standards and Medicare policy. In addition to reconciling indications with evidence, we are focusing on having the implementation of ICD-10 postponed for at least five years; all evaluation and management service audits discontinued; and the three main barriers to effective heart failure management removed: 1) out-of-pocket expenses for the patient; 2) contractor-priced payment levels, and 3) the requirement for the patient to have an “implanted” cardiovascular monitor in order for the physician to receive compensation for optimal heart failure management (daily weight assessment coupled with telephone nursing support).
Visit CardiologyBiller.com to learn more.
