


An Overview of Diabetes and Its Impact on Cath Lab Care
Diabetes is a major co-morbidity of cardiovascular disease and is closely linked to other co-morbidities like hypertension and chronic kidney disease. According to the American Diabetes Association (ADA)1, The American Heart Association (AHA)2 and the Centers for Disease Control (CDC)3, there are approximately 26 million diabetics in the United States, including 18.8 million diagnosed and 7 million undiagnosed patients.
Just under two million (1.9 million) new cases of diabetes were diagnosed in people age 20 and over in 2010. Approximately 80 million U.S. adults have prediabetes and have blood sugar levels are higher than normal, but not high enough to be diagnosed as diabetes. Diabetes and prediabetes increase a person’s risk of heart disease and stroke. The CDC projects that 1 in 3 U.S. adults could have diabetes by 2050, if current trends continue.
These numbers are significant, as recent studies have shown that the risk of myocardial infarction (MI) in people with diabetes is equivalent to the risk in non-diabetic patients with a history of previous MI. This discovery has led to new recommendations by the ADA and AHA that diabetes be considered a coronary artery disease risk equivalent rather than a risk factor.4 There is also compelling data indicating that diabetes mellitus increases the risk for cardiac dysfunction and heart failure independently of other risk factors such as coronary artery disease (CAD) and hypertension.5 The progression of severe coronary atherosclerosis, prolonged hypertension, chronic hyperglycemia, microvascular disease, and autonomic neuropathy all play a role in the alarming rates of cardiovascular disease in diabetics.6 To fully comprehend the magnitude of the impact of diabetes on cardiovascular heath, consider the following facts from the ADA1, AHA2, and CDC3:
- Diabetes is the 7th leading cause of death in the United States. Diabetics have heart disease death rates and stroke risk rates about 2 to 4 times higher than the general population. In people with diabetes, coronary heart disease occurs at a younger age, and women are affected as often as men.
- Heart diseases and stroke are the number-one causes of death and disability among people with type 2 diabetes. At least 65 percent of people with diabetes die from some form of heart disease or stroke.
- A strong correlation between diabetes and hypertension has been found, and this further increases risks of heart disease and stroke. This is most likely due to a combination of microvascular disease, aggressive atherosclerosis, and hyperlipidemia that is more common in diabetics.7
- Diabetes is a leading cause of chronic kidney disease and kidney failure, accounting for 44% of new cases in 2008.8
- One in three women will die of heart disease compared to one in nine women dying of breast cancer, and forty percent of heart attacks in diabetic women result in death. Women with diabetes are two times as likely to have a second heart attack and four times more likely to have heart failure than women without diabetes.9
Metabolic syndrome
Risk for heart disease, diabetes, and stroke increases with the number of metabolic risk factors. In general, a person who has metabolic syndrome is twice as likely to develop heart disease and five times as likely to develop diabetes as someone who doesn’t have metabolic syndrome. Since 90-95% of all diabetics are type 2, understanding metabolic syndrome is essential to providing care, understanding the etiology of type 2 diabetes, and optimizing patient outcomes. Metabolic syndrome is a name for a grouping of risk factors that occur together and greatly increase the risk for coronary artery disease, stroke, and type 2 diabetes. Metabolic syndrome is generally defined by the World Health Organization (WHO)10, National Institutes of Health11, AHA12 and other organizations as the presence of at least three of the following risk factors:
- Increased fat around the waist and abdomen, with a large (BMI) body mass index usually > 25 or waist girth >102 cm (National Institutes of Health) and central obesity, where the body may be described as “apple-shaped.”
- Fasting plasma glucose >110 mg/dl
- Blood pressure >130/85 mmHg or on blood pressure medication [WHO and Adult Treatment Panel (ATP) 111].
- Insulin resistance or glucose intolerance (the body can’t properly use insulin or blood sugar) (AHA, NCEP).
- Abnormal cholesterol levels, with a triglyceride level > 150 mg/dL (1.7 mmol/L) and reduced HDL < 40 mg/dl.
- A family history of type 2 diabetes or a history of diabetes during pregnancy (gestational diabetes).
A classic case presentation of metabolic syndrome:
A female patient (Figures 1-4) presented to the cath lab with a recent onset of atypical chest pain.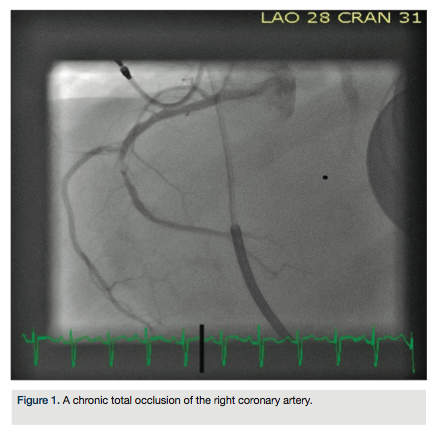 She had a history of cardiomyopathy (ejection fraction of 30%) and an automatic implantable cardioverter defibrillator, a previous stenting of the proximal left anterior descending coronary artery in 2009, hypertension and hyperlipidemia. The patient was a 60-year-old female who was 63 inches tall and 188 pounds (BMI=33.3), creatinine level of 1.5, elevated triglycerides (345), low HDL levels (34), hypertension (180/96), and an elevated blood glucose (256). The patient was non-compliant with medical therapy post-stenting in 2009, and the elevated blood glucose and creatinine levels were not present in 2009.
She had a history of cardiomyopathy (ejection fraction of 30%) and an automatic implantable cardioverter defibrillator, a previous stenting of the proximal left anterior descending coronary artery in 2009, hypertension and hyperlipidemia. The patient was a 60-year-old female who was 63 inches tall and 188 pounds (BMI=33.3), creatinine level of 1.5, elevated triglycerides (345), low HDL levels (34), hypertension (180/96), and an elevated blood glucose (256). The patient was non-compliant with medical therapy post-stenting in 2009, and the elevated blood glucose and creatinine levels were not present in 2009.
This patient had a combination of hyperlipidemia, impaired renal function, elevated blood glucose and hypertension, and was referred for coronary artery bypass surgery after consultation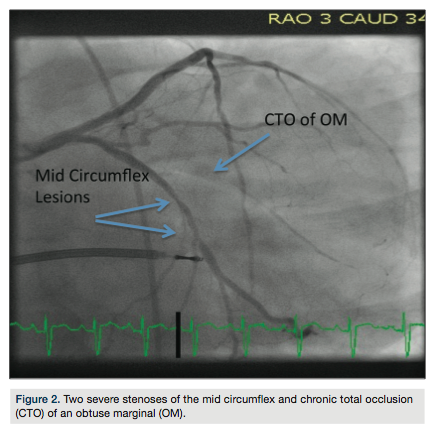 with cardiothoracic surgery.
with cardiothoracic surgery.
Diabetic vascular disease
Along with metabolic syndrome, neuropathy is a major issue in understanding diabetic disease. About 60% to 70% of people with diabetes have mild to severe forms of diabetic autonomic neuropathy, which can be a direct result of long-term hyperglycemia, or be secondary to microangiopathy involving the small vessels that supply blood to the nerves.13 Diabetic autonomic neuropathy is important in cardiovascular disease because the autonomic nervous system plays a crucial role of regulating the heart rate and blood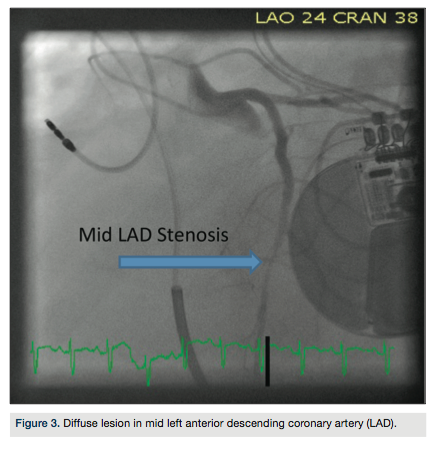 pressure. Arrhythmia, hypo-/hyper-tension, exercise intolerance, and poor surgical outcomes are common manifestations of diabetic autonomic neuropathy. It may also weaken angina symptoms or make them atypical. Diabetic autonomic neuropathy can reduce appreciation for myocardial ischemia or infarct, and delay critical acute treatment for cardiac patients.13 Cardiovascular autonomic neuropathy helps explain the high mortality of patients who have heart disease with diabetes, and appreciating both types of neuropathy is essential in the detection of cardiovascular disease.14
pressure. Arrhythmia, hypo-/hyper-tension, exercise intolerance, and poor surgical outcomes are common manifestations of diabetic autonomic neuropathy. It may also weaken angina symptoms or make them atypical. Diabetic autonomic neuropathy can reduce appreciation for myocardial ischemia or infarct, and delay critical acute treatment for cardiac patients.13 Cardiovascular autonomic neuropathy helps explain the high mortality of patients who have heart disease with diabetes, and appreciating both types of neuropathy is essential in the detection of cardiovascular disease.14
Macro and micro vascular complications. Diabetic vascular complications can be further divided into macrovascular complications (coronary artery disease, peripheral arterial disease, and stroke) and microvascular complications (diabetic nephropathy, neuropathy, and retinopathy).17 Diabetic blood vessels are prone to vasorestriction, platelet aggregation and thrombus, all of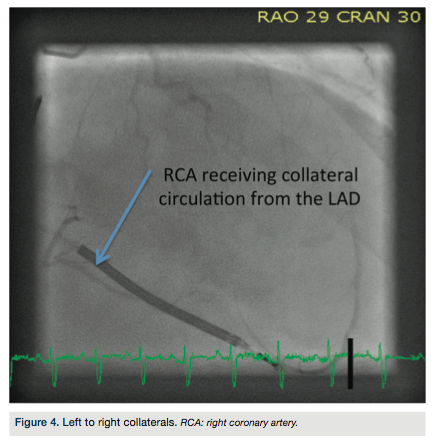 which contribute to the development and progression of cardiovascular disease, as well as the poor prognosis of medical or interventional therapies. They are also exposed to increased endothelial disease risks, due to the lack of nitric oxide production that is common in diabetics and other high-risk patient subsets.
which contribute to the development and progression of cardiovascular disease, as well as the poor prognosis of medical or interventional therapies. They are also exposed to increased endothelial disease risks, due to the lack of nitric oxide production that is common in diabetics and other high-risk patient subsets.
At the macrovascular level, coronary artery luminal area is decreased in diabetic patients and their arteries are more likely to be calcified.18 It is believed that a 3 mm is the threshold below which the coronary artery stent restenosis rates increase significantly, and small vessel size is a key predictor for in-stent restenosis in diabetic patients.19 This is also due to the presence of diabetic angiopathy, long, diffuse lesions, and small lumen vessels in diabetic patients. Small vessels, long lesions, and diabetes are major predictors of restenosis.20
Microvascular complications, especially retinopathy, predict cardiovascular disease and coronary artery disease death in individuals with type 2 diabetes who are free of cardiovascular disease at baseline. The association between retinopathy and mortality is independent not only of conventional cardiovascular disease risk factors, but also of glycemic control, duration of diabetes, and proteinuria.21 Understanding the complexity and magnitude of microvascular disease in diabetic patients helps to determine medical therapy, access routes, and interventional techniques for coronary artery disease.
coronary artery disease death in individuals with type 2 diabetes who are free of cardiovascular disease at baseline. The association between retinopathy and mortality is independent not only of conventional cardiovascular disease risk factors, but also of glycemic control, duration of diabetes, and proteinuria.21 Understanding the complexity and magnitude of microvascular disease in diabetic patients helps to determine medical therapy, access routes, and interventional techniques for coronary artery disease.
Cath lab care for the diabetic patient
Since diabetes is associated with a significant increase in cardiovascular disease, even with intensive glycemic control, cath lab practice is significantly impacted by diabetic vascular disease. Interventional treatment strategies have changed since drug-eluting stents (DES) have become broadly used, and DES significantly improves the early and longer-term success rate of percutaneous coronary intervention in patients with diabetes, thereby offering more patients non-surgical treatment options. In particular, the Resolute stent (Medtronic) was studied in clinical trials that concluded that long-term clinical data of patients with non-insulin-treated diabetes is equivalent to patients without diabetes, but patients with insulin-treated diabetes remain a higher risk subset.22
The implantation of drug-eluting stents in diabetics is associated with overall excellent in-hospital and long-term results. However, the long-term effectiveness in insulin-dependent patients is lower, because of the greater risk of restenosis.23 Coronary artery bypass graft surgery (CABG) is still the recommended standard of care for diabetics with multi-vessel or left main coronary artery disease, especially insulin-dependent diabetics.
The optimal treatment strategy for diabetic patients has been a continuous subject of debate over the last decades.24 While stent technology and medical therapies improve, numerous trials25, including the recent FREEDOM trial, shows primary endpoints that favor CABG to stents in multi-vessel and left main disease. In 2012, the FREEDOM trial studied 1900 patients with multiple vessel disease and diabetes.26 Patients treated with CABG had lower rates of myocardial infarction and death from any cause than those undergoing PCI, at both 2 years and 5 years after intervention. Repeat revascularization within one year after the initial treatment was more common with PCI than with CABG. The results of the FREEDOM trial validated numerous other studies that have been performed and support CABG in the presence of left main and multi-vessel coronary artery disease. However, it is important that a multi-disciplinary approach, including cardio-thoracic surgery consultation, should be utilized when treating diabetics with complex coronary artery disease.
In patients with types 1 and 2 diabetes, an improvement in blood sugar levels has clearly been shown in several clinical studies to reduce the risk of development of small-vessel disease and to slow the progression of established small-vessel disease like retinopathy, nephropathy and neuropathy.25,27 Therefore, medical therapy, diet, exercise and glucose control are also vital components for medically treating diabetics, even if they require no revascularization at the time of cardiac catheterization.
Suggested guidelines
In the cath lab setting, the following guidelines are helpful in caring for diabetic patients:
- Anti-diabetic medications, especially insulin, and fasting may cause iatrogenic hypoglycemia.28 Therefore, diabetic medication dosing needs to be coordinated around the NPO period that begins pre-cath.29 Insulin may be given on sliding scales or other modified dosing, depending on the patient’s blood glucose levels.
- Blood glucose monitoring needs to be performed pre and post cath to reduce chances of hypoglycemia, and patients should resume a normal diet as soon as possible post catheterization.
- Metformin is usually discontinued 1 day pre procedurally and 2 days post cath due to the possibility of causing lactic acidosis and acute nephropathy.30
- Pre-procedural labs, especially renal function tests like creatinine and eGFR, should be performed as close to the procedure time as possible, because there is a strong clinical correlation between chronic kidney disease and diabetes.
- Because of a higher risk for renal failure in diabetics, limit contrast and hydrate diabetics whenever possible to prevent cath lab-induced nephropathies.31
- Be vigilant with physical assessment, perform comprehensive pulse assessments, and assess the integrity of the skin to ensure that there are no ulcers, skin lesions, or diminished pulses.
- Access site selection should consider metabolic syndrome, poor distal circulation in the feet, and skin ulcers. The large pannus of patients with metabolic syndrome can complicate hemostasis. Radial access should be considered in these patients, as they are at significantly higher risks for leg complications and infections than the general population.
- The use of closure devices in diabetics can create an environment for infection. To reduce infection risk, consider re-prepping the groin and changing gloves to produce the safest possible environment for closure device deployment. Diabetic patients have a higher risk of access site infection because micro vascular dysfunction may compromise circulation and the wound healing processes are prolonged.32
- For patients with metabolic syndrome, closure devices can greatly assist femoral artery hemostasis by eliminating the need for difficult line pulls.
- Anti-coagulation therapy needs to be carefully managed in diabetic patients, as insulin may inhibit the reversal effect of protamine. Patients exposed to protamine through the use of protamine-containing insulin or during heparin neutralization may experience life-threatening reactions and fatal anaphylaxis upon receiving large doses of protamine intravenously.33
Because diabetics have significantly higher rates of cardiovascular disease, and a greater potential for complications and severe disease than the general population, it is important to appreciate working with this increasingly large segment of the population. Diabetics require highly skilled care providers to optimize their outcomes, and will continue to become a larger portion of the cath lab patient base, especially if current trends continue. Therefore, refining clinical skills and practice guidelines to work with diabetics should be an important focus for all cardiovascular care providers.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
The authors may be contacted via Richard Merschen at richardmerschen@verizon.net.
References
- American Diabetes Association. Diabetes basics. Diabetes statistics. Available online at https://www.diabetes.org/diabetes-basics/diabetes-statistics/. Accessed April 23, 2013.
- Centers for Disease Control. Diabetes Public Health Resource: 2011 National Diabetes Fact Sheet. Available online at: https://www.cdc.gov/diabetes/pubs/factsheet11.htm. Accessed April 29, 2013.
- Diabetes Pro. Meeting reports: American Heart Association’s Scientific Sessions 2012 (AHA). Cardiovascular innovations: the future is now. Available online at https://professional.diabetes.org/CongressReport_Display.aspx?CID=92091. Accessed May 1, 2013.
- Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, et al; American Heart Association; American Diabetes Association. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Diabetes Care. 2007 Jan; 30(1): 162-172.
- Boudina S, Abel ED. Diabetic cardiomyopathy, causes and effects. Rev Endocr Metab Disord. 2010 Mar; 11(1): 31-39. doi: 10.1007/s11154-010-9131-7.
- Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, Mitch W, Smith SC Jr, Sowers JR. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation. 1999 Sep 7; 100(10): 1134-1146.
- Reaven GM, Lithell H, Landsberg L. Hypertension and associated metabolic abnormalities: the role of insulin resistance and the sympatho-adrenal system. N Engl J Med. 1996; 334: 374-382.
- National Kidney Foundation. Kidney disease: causes. Available online at https://www.kidney.org/atoz/content/kidneydiscauses.cfm. Accessed August 6, 2013.
- American Diabetes Association. Living with diabetes: women’s health. Coronary heart disease. Available online at https://www.diabetes.org/living-with-diabetes/women/coronary-heart-disease.html. Accessed May 2, 2013
- Takamiya T, Zaky WR, Edmundowics D, Kadowak T, Ueshima H, Kuller LH, Sekikawa A. WHO-defined metabolic syndrome is a better predictor of coronary calcium than ATPIII criteria in American men age 40-49. Diabetes Care. 2004; 27(12): 2977-2979.
- American Heart Association. About metabolic syndrome. Available online at https://www.heart.org/HEARTORG/Conditions/More/MetabolicSyndrome/About-Metabolic-Syndrome_UCM_301920_Article.jsp. Accessed August 6, 2013.
- PubMed Health. Metabolic syndrome: insulin resistance syndrome; syndrome X. Available online at https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004546. Accessed August 6, 2013.
- Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care. 2003; 26(5): 1553-1579.
- Maser RE, Mitchell BD, Vinik AI, Freeman R. The association between cardiovascular autonomic neuropathy and mortality in individuals with diabetes: a meta-analysis. Diabetes Care. 2003 Jun; 26(6): 1895-1901.
- Hinkes M. Diabetes: Taking steps to prevent amputation. Lower Extremity Review. August 2009. Available online at https://lowerextremityreview.com/article/diabetes-taking-steps-to-prevent-amputation. Accessed August 6, 2013.
- Centers for Disease Control and Prevention. Press release: CDC report finds large decline in lower-limb amputations among U.S. adults with diagnosed diabetes. Available online at https://www.cdc.gov/media/releases/2012/p0124_lower_limb.html. Accessed August 6, 2013.
- Fowler MJ. Microvascular and macrovascular complications of diabetes. Clinical Diabetes. 2008 April; 26(2): 77-82. doi: 10.2337/diaclin.26.2.77.
- Hatada K, Sugiura T, Nakamura S, Kamihata H, Fujimoto T, Baden M, Takahashi N, Iwasaka T. Coronary artery diameter and left ventricular function in patients on maintenance hemodialysis treatment: comparison between diabetic and nondiabetic patients. Nephron. 1998 Nov; 80(3): 269-273.
- Süselbeck T, Latsch A, Siri H, Gonska B, Poerner T, Pfleger S, Schumacher B, Borggrefe M, Haase KK. Role of vessel size as a predictor for the occurrence of in-stent restenosis in patients with diabetes mellitus. Am J Cardiol. 2001 Aug 1; 88(3): 243-247.
- Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol. 2010 Feb 2; 55(5): 432-440. doi: 10.1016/j.jacc.2009.10.014.
- Laakso M. Heart in diabetes: a microvascular disease. Diabetes Care. 2011 May; 34 (Supplement 2): S145-S149. Available online at https://care.diabetesjournals.org/content/34/Supplement_2/S145.full#corresp-1. Accessed August 6, 2013.
- Silber S, Serruys PW, Leon MB, Meredith IT, Windecker S, Neumann FJ, Belardi J, et al. Clinical outcome of patients with and without diabetes mellitus after percutaneous coronary intervention with the resolute zotarolimus-eluting stent: 2-year results from the prospectively pooled analysis of the international global RESOLUTE program. JACC Cardiovasc Interv. 2013 Apr; 6(4): 357-368. doi: 10.1016/j.jcin.2012.11.006. Epub 2013 Mar 22.
- Voudris V, Karyofillis P, Thomopoulou S, Doulaptsis C, Manginas A, Pavlides G, Cokkinos DV. Long-term results after drug-eluting stent implantation in diabetic patients according to diabetic treatment. Hellenic J Cardiol. 2011; 52(1): 15-22.
- Harskamp RE, Park DW. Percutaneous coronary intervention in diabetic patients: should choice of stents be influenced? Expert Rev Cardiovasc Ther. 2013 May; 11(5): 541-553. doi: 10.1586/erc.13.38.
- Cutlip DE. Percutaneous coronary intervention in patients with diabetes and multi-vessel or left main disease — a review. Interventional Cardiology. 2012; 7(1): 37-40. Available online at https://www.radcliffecardiology.com/articles/percutaneous-coronary-intervention-patients-diabetes-and-multivessel-or-left-main-disease-r. Accessed August 6, 2013.
- Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, et al; FREEDOM Trial Investigators. Strategies for multivessel revascularization in patients with diabetes N Engl J Med. 2012 Dec 20; 367(25): 2375-2384.
- Goldfine AB, Goldfine HL. Cardiology patient pages. Cardiovascular disease in the diabetic patient. Circulation. 2003 Jan 21; 107(2): e14-6.
- Maynard GA, Huynh MP, Renvall M. Iatrogenic inpatient hypoglycemia: risk factors, treatment, and prevention. Analysis of current practice at an academic medical center with implications for improvement efforts. Diabetes Spectrum 2008 Oct; 21(4): 241-247.
- Loh-Trivedi M, Rothenberg DM, Schade DS, Schwer WA. Perioperative management of the diabetic patient. Updated June 10, 2013. Available online at https://emedicine.medscape.com/article/284451-overview. Accessed August 6, 2013.
- Marks JB. Perioperative management of diabetes. Am Fam Physician. 2003 Jan 1; 67(1): 93-100.
- Pecoraro RE, Ahroni JH, Boyko EJ, Stensel VL. Chronology and determinants of tissue repair in diabetic lower-extremity ulcers. Diabetes. 1991 Oct; 40(10): 1305-1313.
- Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010 Mar; 89(3): 219-229. doi: 10.1177/0022034509359125. Epub 2010 Feb 5.
- Drugs.com. Protamine Sulfate Injection. Available online at https://www.drugs.com/pro/protamine-sulfate-injection.html#indications. Accessed June 1, 2013.
