


Overcoming Calcified, Tortuous Access for Large Devices with the SoloPath Balloon-Expandable and Collapsible Sheath
This article has been altered from the print version.
Disclosures: Dr. Tuchek reports he is a consultant to Terumo, and is a Medtronic consultant and CoreValve investigator.
J. Michael Tuchek, DO, FACS, can be contacted at mtuchek@openheart.net.
Can you tell us about your facility and practice?
I am a cardiovascular surgeon and a senior partner in one of the largest groups of cardiac surgeons in the country, Cardiac Surgery Associates, which covers over 30 hospitals in 3 states. At Loyola University, I am involved as an investigator in several thoracic stent graft trials, including the last three large Medtronic stent graft trials, and I am also an investigator in the Medtronic CoreValve trial.
I still do private practice with stent graft work, thoracic and peripheral vascular surgery, open-heart surgery and valves, and so on. I try to do a little bit of everything. I was first introduced to the SoloPath device during the early CoreValve trial as a result of access issues in small, elderly, female patients with calcified, tortuous iliacs.
How is the SoloPath useful?
In patients receiving a large device, whether it is a percutaneous aortic valve such as the CoreValve, a thoracic stentgraft, or an abdominal stent graft for an aneurysm, one of the issues has always been access. Can we get there? We go through the groin almost all the time for these cases. CoreValve is different than aneurysms because there are alternative access sites. We can do mini-sternotomies and mini-thoracotomies, or go through the subclavians, or even the carotids, to really push the envelope. But in the United States, we mostly go through the groin, and that means for all comers: patients with small arteries, or people who have done a lot of smoking and abused themselves over the years, diabetics, and/or patients with high cholesterol, etc. These patients tend to have a lot of plaque formation, and their iliac arteries may be in bad shape. When we put big devices in these patients, it can be dangerous. The most difficult section to move through runs from the femoral artery up to the abdominal aorta, because it is so narrow. We can crack things, or perhaps can’t get devices in at all. We can cause bleeding when we are pulling devices out. There is something called ‘iliac on a stick’ that has happened to me a few times, where the iliac artery literally gets stuck to the device, is pulled out, and of course, catastrophically bleeds. The most common complication with thoracic stent graft trials, one of the largest with abdominal stent graft trials, and also in the CoreValve percutaneous valve trials, is, in fact, from problems with vascular access. It is not necessarily heart or valve issues that are problematic for operators, but vascular access. As a result, investigators have struggled to decide which patients can be entered into trials of large devices. Many of the decisions about who gets into a trial and who doesn’t actually result from an evaluation of vascular access, not about what a patient’s valve needs or if they don’t meet gradients, for example. It is the problem of getting the device where it needs to be in a safe manner.
The SoloPath balloon-expandable transfemoral access system (Terumo) has a very small profile, allowing you to gain access in really small, calcified, tortuous vessels, and then you blow it up like a stent, except the SoloPath consists of a flexible, reinforced polymer sheath with an external collapsible outer jacket and specially folded distal end (the sheath) pre-mounted over a central balloon dilatation catheter (the expander).
It is designed to be inflated up to 20 atmospheres (atm), and assist in ballooning out stenoses and creating a straight path. I use the SoloPath mostly in CoreValve cases. In a bad artery, without the protection offered by the SoloPath sheath, there is a much greater risk of rupture, spasm, embolization, and injury to the artery. Using the SoloPath helps reduce the risk of passing catheters in and out of the artery. All activity takes place inside the sheath; as a result, there is a decreased risk of catastrophic vascular complications, which are directly associated with operative mortality. In both thoracic stent graft and percutaneous aortic valve trials, there is almost a three-fold increased risk of mortality resulting directly from vascular access complications. SoloPath significantly lowers the vascular access complication rate by straightening out the artery and making it easier for us to place large devices.
The newest version of the SoloPath not only balloons up to allow operators a new pathway to insert devices, but at the end of the procedure, it will actually shrink back down again, using another set of balloons. As a result, when the SoloPath is pulled out, it is less likely to rip or pull the artery. It collapses down and you sneak it right back out again. There are three points at which damage takes place in vascular access: 1) gaining access; 2) putting devices in and out multiple times; and 3) when the sheath is removed. The SoloPath minimizes risk during these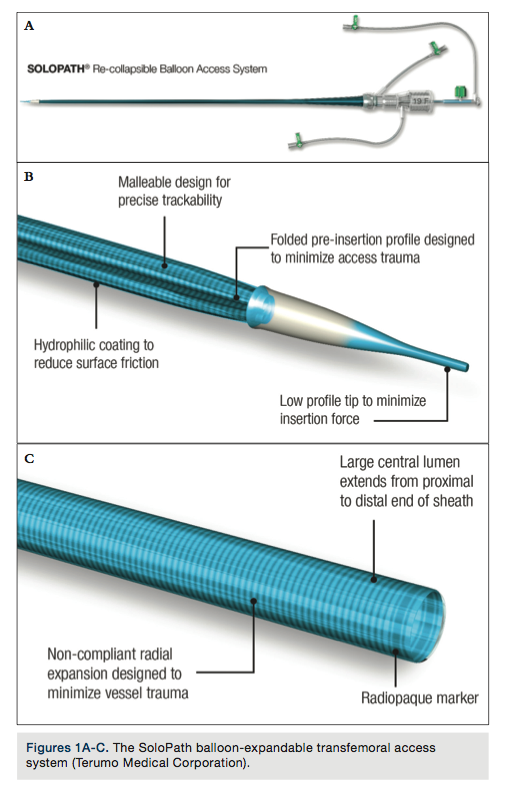 periods, because the operator inflates the sheath to improve access and then shrinks it back down again to pull it out. This is a huge advantage that makes it possible for us to treat patients that we might not have been able to treat otherwise, due to the risk of putting anything through their arteries. It also allows us to take patients on the cusp, the marginal patients, and treat them more safely, because we have protected their arteries by putting in the SoloPath sheath.
periods, because the operator inflates the sheath to improve access and then shrinks it back down again to pull it out. This is a huge advantage that makes it possible for us to treat patients that we might not have been able to treat otherwise, due to the risk of putting anything through their arteries. It also allows us to take patients on the cusp, the marginal patients, and treat them more safely, because we have protected their arteries by putting in the SoloPath sheath.
How long is the device?
The SoloPath sheath comes in two different lengths, 25 cm and 35 cm. We essentially want the sheath to be long enough to go from the groin through the external iliac artery, the common iliac artery, and up into the abdominal aorta. The abdominal aorta is large enough that it will take almost any device. Outer diameter ranges from 17 to 24 French (F), with inner diameters from 14 to 21F.
Can you share more about what happens when the SoloPath is inflated in the artery?
The SoloPath puts pressure against any calcium, pushing it against the wall of the vessel. It is the same process as placing a balloon angioplasty and stent. Problems in vascular access can occur when sheaths are moved perpendicular to the calcium, as well as from the act of pushing catheters and devices through the artery and pulling them back out again. Moving catheters perpendicular to the plaque, going in and out of the artery, becomes disruptive. Blood can start to dissect under the plaque, causing it to rupture, and that can lead to catastrophic closure of the arteries and/or distal embolization. The SoloPath is designed to minimize disruption from passes up and down the artery, because all activity takes place in the sheath, which has pushed the calcium aside, just as balloon angioplasty or a stent would.
Have you experienced any complications?
There have been no significant complications with the device since we started using it. I am even more pleased with the new SoloPath that has the balloon-collapsible sheath. Not only does it go up just like the original SoloPath, but now it shrinks back down again, making it easier to pull out with minimal forces tugging or pulling on the artery/plaque.
How long have you been using the SoloPath?
I have been using it since it was first cleared by the FDA in 2009. In the CoreValve world, the SoloPath has become fairly popular, because it has allowed us to push the envelope more with smaller arteries. There are many little old frail ladies who weigh ninety pounds, with real access issues. We have gone as far as having to do a mini-sternotomy to put in these devices, because they just have no access and there is nothing you can do. The SoloPath can’t fix everything, but for any patient who holds the possibility of access, it allows us to do it more safely.
Do you have any tips or tricks for use?
Use of the SoloPath is simple if you follow the instructions. It goes in easily. Inflate the sheath to 4 atm, wait a few seconds and then inflate to 20 atm. Count a minute, then you are done. Go ahead and do the procedure.
The SoloPath is very hemostatic, meaning there isn’t much leakage out of the sheath introducer, which is a nice aspect of the device. For some sheaths, this can mean it is hard to push the devices through. Other sheaths allow the devices to go through easily, but there is an issue with back bleeding. The SoloPath doesn’t leak and it also allows devices to go in fairly easily. Once the procedure is finished, with the single balloon SoloPath device, the operator would twist it 90˚ to make sure that there is nothing sticking or spasming, and then pull it straight out, like any normal sheath. With the new, balloon-collapsible SoloPath, you simply inflate the balloon that shrinks down the catheter and then pull out the sheath.
The SoloPath doesn’t require any extra work other than the one-minute inflation time. It is just as fast as any other sheath, plus one minute, and is well worth that one minute of inflation time, because it means worry-free access to the abdominal aorta.
It seems the SoloPath would improve clinical outcomes, because it lessens the risk of difficult vascular access.
Right. Particularly in the transcatheter aortic valve world, the SoloPath has been accepted and embraced emphatically by many operators not only in the U.S., but globally. That is a testimony to the fact that it works. Physicians are pleased with the ability to get access in areas that they otherwise couldn’t, or get very safe access in areas where it might not be so safe to put in a regular sheath. In fact, I will be using the SoloPath tomorrow in a very marginal set of iliac arteries for a CoreValve case.
When would use of a SoloPath not be appropriate?
The amount of blockage is one thing. We can balloon and stent almost any blockage out there. But access isn’t only about stenting and leaving the artery open. Our main concern is trying to get a large device through the sheath. Let’s say a patient has an artery that is 4 mm normally, but it has blockages essentially making it 3 mm. Now you are going to balloon this artery to 18F, which is 6+ mm? In this scenario, the artery will tear, no matter what you do. As soon as that sheath comes out, the patient is going to bleed. So there is a small size limit to everything we put in. We can’t put a 21F device into an artery that is only 4 mm in diameter, because the artery simply isn’t large enough, even if it is perfectly clean, to accept something that large. The difference with SoloPath is that it allows us to really push the envelope with arteries that are highly calcified or highly diseased with plaque, without having to sacrifice the safety margins of multiple passes with devices and getting the sheath back out again without tearing the artery. The SoloPath can get around the plaque burden, the narrowing due to blockages and tortuosities, and make it safer to do so.
Any final thoughts?
I have been very pleased with the availability of the SoloPath representatives; they are a service-oriented group. There is a very short learning curve to use this device. It has multiple ports at the end of the sheath. You need to learn the port to inflate the balloon and the port to make the sheath shrink down again, and that takes all of 3 seconds to figure out. Otherwise, it is standard operating procedure. Terumo is the first company out there with expandable and now recollapsible sheaths. Everyone is following in Terumo’s footsteps, with multiple companies working on similar devices. The SoloPath is a hot item when it comes to access for large devices such as percutaneous aortic valves and stent grafts. This device is not for putting in a 6F coronary catheter. It is meant for placing large devices into patients with difficult vascular access. SoloPath is the 800lb gorilla when it comes to this technology, because it was out first and, as far as I am aware, is the best product to date.
