


Occupational Health Hazards in the Interventional Laboratory: Progress Report of the Multispecialty Occupational Health Group
The Multispecialty Occupational Health Group (MSOHG), formed in 2005, is an informal coalition of societies representing professionals who work in, or are concerned with, interventional fluoroscopy. The group’s long-term goals are to improve occupational health and operator and staff safety in the interventional laboratory while maintaining quality patient care and optimal use of the laboratory. MSOHG has conducted a dialogue with equipment manufacturers and has developed a list of specific objectives for research and development. The group has also represented the member societies in educating regulators, in educating interventionalists, and in fostering and collaborating on research into occupational health issues affecting interventionalists. Not least of the group’s accomplishments, as a result of their collaboration in MSOHG, the group’s members have developed a mutual respect that can serve as a basis for joint efforts in the future among interventionalists of different medical specialties.
Abbreviations: IAEA = International Atomic Energy Agency, MITA = Medical Imaging and Technology Alliance, MSOHG = Multispecialty Occupational Health Group
The Multispecialty Occupational Health Group (MSOHG) is an informal coalition of societies representing professionals who work in, or are concerned with, interventional fluoroscopy laboratories. The MSOHG was formed in 2005 to address the occupational hazards of interventionalists, with particular emphasis on the radiation-related and orthopedic hazards. The genesis of the group was a meeting, suggested and facilitated by Stephen Balter, PhD, of representatives of the Society for Cardiac Angiography and Interventions, the Heart Rhythm Society, and the Society of Interventional Radiology (SIR) on May 27, 2005, in Bethesda, Maryland. The purpose was to discuss occupational health issues common to interventional cardiologists and interventional radiologists.
The participants at the initial meeting concluded that a combined effort by multiple professional societies was more likely to succeed than individual efforts, and that common ground existed among the various groups of medical professionals. Subsequently, other professional societies were invited to join the group. At present, the member societies are the American Association of Physicists in Medicine, the American College of Radiology, Heart Rhythm Society, the Society for Cardiovascular Angiography and Interventions, SIR, the Society of Invasive Cardiovascular Professionals, and the Society of NeuroInterventional Surgery. The long-term goals of the group are to allow operators and staff to work a full career with minimal occupational radiation exposure and without incurring orthopedic injuries, and to improve operator and staff safety while maintaining optimal use of the interventional laboratory and quality patient care.
A position paper on occupational health issues in interventional medicine was published in 2009 in cardiology and radiology journals.1 This article reviewed available data on the prevalence of occupational health risks and concluded that sufficient data existed to demonstrate that the interventional laboratory presents workplace hazards that must be acknowledged, better understood, and mitigated to the greatest extent possible.
 Association headquarters in January 2009 to develop a list of specific objectives. MITA distributed the list (Table) to the relevant manufacturers. At a subsequent meeting in November 2009, the MITA representative reaffirmed his organization’s commitment to working with the MSOHG. A representative from one manufacturer reported that his company had used information from earlier meetings, and specifically the list in the Table, to prioritize its research and development initiatives. A representative from another manufacturer made the same statement to an MSOHG representative after the meeting. Because of sales, marketing, and regulatory concerns, none of the manufacturers could discuss current projects under development. Only products and technologies that had already been approved for sale in the United States by the Food and Drug Administration were discussed.
The serious and productive dialogue that MSOHG, on behalf of the various member societies, has opened with commercial vendors at the international level is an important accomplishment. Concrete changes will occur, but only if the members of MSOHG’s constituent societies make it clear to the manufacturers that the issues and goals in the Table are of great concern. As the physicians who are the end users of these products, we need to work with industry to implement these changes. A necessary first step is a clear public statement of what we need. To this end, we are publicizing the list in the Table so the members of all of MSOHG’s constituent societies have a common frame of reference. In addition, if members of any of these societies have suggestions for additions to this list, we need to know about them. Please contact your society, and ask that your suggestion be forwarded to your society’s liaison to MSOHG.
Association headquarters in January 2009 to develop a list of specific objectives. MITA distributed the list (Table) to the relevant manufacturers. At a subsequent meeting in November 2009, the MITA representative reaffirmed his organization’s commitment to working with the MSOHG. A representative from one manufacturer reported that his company had used information from earlier meetings, and specifically the list in the Table, to prioritize its research and development initiatives. A representative from another manufacturer made the same statement to an MSOHG representative after the meeting. Because of sales, marketing, and regulatory concerns, none of the manufacturers could discuss current projects under development. Only products and technologies that had already been approved for sale in the United States by the Food and Drug Administration were discussed.
The serious and productive dialogue that MSOHG, on behalf of the various member societies, has opened with commercial vendors at the international level is an important accomplishment. Concrete changes will occur, but only if the members of MSOHG’s constituent societies make it clear to the manufacturers that the issues and goals in the Table are of great concern. As the physicians who are the end users of these products, we need to work with industry to implement these changes. A necessary first step is a clear public statement of what we need. To this end, we are publicizing the list in the Table so the members of all of MSOHG’s constituent societies have a common frame of reference. In addition, if members of any of these societies have suggestions for additions to this list, we need to know about them. Please contact your society, and ask that your suggestion be forwarded to your society’s liaison to MSOHG.
Work With Manufacturers
The MSOHG cannot specify particular modifications in equipment or laboratory design, as we do not have the expertise or authority to do so. Because achieving the MSOHG’s goals requires changes in the ways interventional laboratories are configured and improvements in the fluoroscopic equipment used in these laboratories, it was clear to us that direct conversations with the manufacturers of this equipment were essential. To avoid the possible appearance of favoritism, and to make sure that a consistent message was delivered to all manufacturers of this equipment, MSOHG representatives met with the Medical Imaging and Technology Alliance (MITA), a division of the National Electrical Manufacturers Association, in October 2008. MITA represents medical imaging equipment manufacturers, innovators, and product developers whose sales comprise more than 90% of the global market for medical imaging technology. The meeting was attended by representatives from MITA, General Electric, Philips, Siemens, and Toshiba. At this meeting, it became clear that the manufacturers needed a prioritized list of specific objectives, more details about the issues involved, and some assurance that, as a group, interventionalists would support the effort by recommending purchase of equipment that met these objectives. As a representative from one manufacturer put it, “If we develop technologies that reduce dose to the patient and the operator, but nobody buys it, does it matter?” MSOHG representatives met with MITA again at National Electrical Manufacturers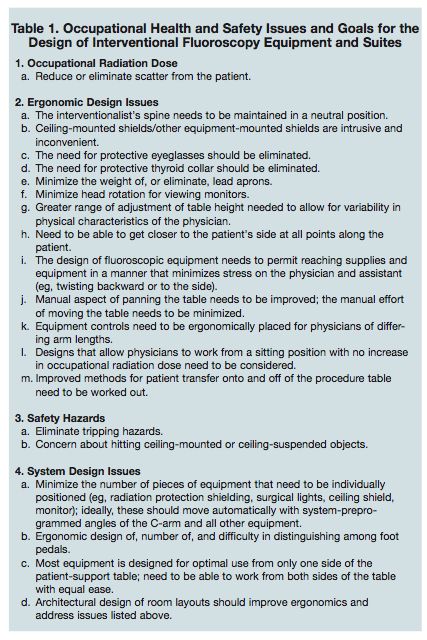 Association headquarters in January 2009 to develop a list of specific objectives. MITA distributed the list (Table) to the relevant manufacturers. At a subsequent meeting in November 2009, the MITA representative reaffirmed his organization’s commitment to working with the MSOHG. A representative from one manufacturer reported that his company had used information from earlier meetings, and specifically the list in the Table, to prioritize its research and development initiatives. A representative from another manufacturer made the same statement to an MSOHG representative after the meeting. Because of sales, marketing, and regulatory concerns, none of the manufacturers could discuss current projects under development. Only products and technologies that had already been approved for sale in the United States by the Food and Drug Administration were discussed.
The serious and productive dialogue that MSOHG, on behalf of the various member societies, has opened with commercial vendors at the international level is an important accomplishment. Concrete changes will occur, but only if the members of MSOHG’s constituent societies make it clear to the manufacturers that the issues and goals in the Table are of great concern. As the physicians who are the end users of these products, we need to work with industry to implement these changes. A necessary first step is a clear public statement of what we need. To this end, we are publicizing the list in the Table so the members of all of MSOHG’s constituent societies have a common frame of reference. In addition, if members of any of these societies have suggestions for additions to this list, we need to know about them. Please contact your society, and ask that your suggestion be forwarded to your society’s liaison to MSOHG.
Association headquarters in January 2009 to develop a list of specific objectives. MITA distributed the list (Table) to the relevant manufacturers. At a subsequent meeting in November 2009, the MITA representative reaffirmed his organization’s commitment to working with the MSOHG. A representative from one manufacturer reported that his company had used information from earlier meetings, and specifically the list in the Table, to prioritize its research and development initiatives. A representative from another manufacturer made the same statement to an MSOHG representative after the meeting. Because of sales, marketing, and regulatory concerns, none of the manufacturers could discuss current projects under development. Only products and technologies that had already been approved for sale in the United States by the Food and Drug Administration were discussed.
The serious and productive dialogue that MSOHG, on behalf of the various member societies, has opened with commercial vendors at the international level is an important accomplishment. Concrete changes will occur, but only if the members of MSOHG’s constituent societies make it clear to the manufacturers that the issues and goals in the Table are of great concern. As the physicians who are the end users of these products, we need to work with industry to implement these changes. A necessary first step is a clear public statement of what we need. To this end, we are publicizing the list in the Table so the members of all of MSOHG’s constituent societies have a common frame of reference. In addition, if members of any of these societies have suggestions for additions to this list, we need to know about them. Please contact your society, and ask that your suggestion be forwarded to your society’s liaison to MSOHG.
Research Initiatives
Mortality One of the primary purposes for which the MSOHG was formed was to develop plans for surveys of members of the participating societies. The goal was to better define the health detriment from working as an interventionalist. It quickly became clear that the MSOHG did not have the expertise or the financial resources to design and conduct a scientifically valid survey or to analyze the results. Fortunately, some of the participants at the initial MSOHG meeting had contacts at the Radiation Epidemiology Branch of the National Cancer Institute. The Radiation Epidemiology Branch has been conducting research on radiation-related mortality in medical radiation workers for some time and is interested in examining radiation-related health effects in interventionalists.2,3 With the cooperation of the member societies of the MSOHG, the Radiation Epidemiology Branch began the Interventional Fluoroscopist Occupational Health study, which is ongoing at present. For the Interventional Fluoroscopist Occupational Health study, the Radiation Epidemiology Branch is using membership lists from SIR, the Society for Cardiovascular Angiography and Interventions, Heart Rhythm Society, Society of NeuroInterventional Surgery, Radiological Society of North America, and American College of Cardiology, as well as information from the American Medical Association Physician Masterfile and the American Board of Medical Specialties, to identify the members of three groups of physicians: a high radiation exposure group (e.g., interventionalists), a moderate exposure group (e.g., other radiologists) and a low exposure group (e.g., family medicine physicians and psychiatrists). The Radiation Epidemiology Branch are determining which individuals in these groups are deceased and submitting these names to the National Death Index to determine cause of death. This will permit a determination of whether there is increased death rate in physicians exposed to higher occupational radiation doses and, if so, what the causes of death are. Cataracts There is increasing evidence that occupational radiation exposure in the interventional laboratory may be sufficient to cause the development of cataracts.4,5 The International Atomic Energy Agency (IAEA) is actively investigating this issue with the Retrospective Evaluation of Lens Injuries and Dose study by using surveys of interventional cardiologists in Asia, Europe, and South America. (Details are available at https://rpop. iaea.org/RPOP/RPoP/Content/News/des-relid.htm.) At the November 2009 MSOHG meeting, Norman Kleiman, PhD, an expert in this field and a participant in the Retrospective Evaluation of Lens Injuries and Dose study, expressed interest in extending this work to interventionalists in the United States. The MSOHG is highly supportive of this endeavor and is working with Dr. Kleiman to develop an appropriate survey instrument that can be distributed to the memberships of the member societies.Liaison with the International Atomic Energy Agency (IAEA)
Madan Rehani, PhD, of the IAEA was present at the November 2009 meeting of the MSOHG. He presented the IAEA perspective on occupational exposure in interventionalists. The IAEA is concerned about radiation doses to patients and interventionalists. Dr. Rehani provided additional information from the IAEA radiation cataract study, including evidence of increased lens opacities in the eyes of nurses. This implies the need to provide ceiling-suspended radiation shields at locations besides the operator’s working position.6 He also noted that there are substantial changes in eye lens dose with minor adjustments of ceiling-suspended shields. The IAEA is conducting an international survey of interventional cardiologists as part of a larger project to determine and follow occupational radiation doses: the Information System on Occupational Exposure in the Medical, Industrial and Research Areas. A preliminary survey of interventional cardiologists has shown that occupational dose data are not readily available. Because it is difficult to get accurate occupational doses for staff in the interventional suite, the IAEA Working Group on Interventional Cardiology, a component of the Information System on Occupational Exposure in the Medical, Industrial and Research Areas, suggests that some form of automated dosimetry system be integrated into the fluoroscopy equipment. Also through the IAEA Working Group on Interventional Cardiology, an international guideline on occupational radiation protection in interventional radiology is being modified as a guideline for interventional cardiologists.7 It is intended that this new guideline will be published as official guidance of the Asian Pacific Society of Interventional Cardiology, the Sociedad Latinoamericana de Cardiologia Intervencionista, and possibly the Society for Cardiac Angiography and Interventions. It is intended that these two documents, for interventional radiologists and for interventional cardiologists, will serve as a basis for IAEA guidance on this topic.Monitoring of Occupational Dose
Part of the difficulty in obtaining accurate occupational doses for staff in the interventional suite appears to be lack of compliance with personnel dose monitoring regulations. MSOHG representatives attribute this in large part to the policies used in regulation of occupational exposure. Typical policies are based on the assumption that virtually all occupational exposure is avoidable. The data on health care occupational exposure presented in National Council on Radiation Protection and Measurements Report 1608 reinforce this belief, as 95% of all monitored health care workers have minimal occupational dose. Many regulators have a poor understanding of what interventionalists do, and how they work. There is often little understanding that occupational radiation exposure is, at present, an unavoidable consequence of performing fluoroscopically guided procedures. In addition, effective dose is often calculated based on formulas that overestimate the actual dose.9 As a result, some interventionalists are subjected repeatedly to reviews of their radiation exposure despite occupational doses that are within the expected range for their occupation. It is not surprising that many operators do not wear their radiation badges.6,10 A substantial opportunity exists for education of regulators, as the need for radiation monitoring is an issue of health and safety, and regulations should encourage this behavior rather than discourage it.Intersociety Cooperation
Finally, one of the most significant accomplishments of MSOHG has been the development of a truly collegial atmosphere among the participants as we work together as colleagues on common goals. Often in the past, relationships between the cardiology and radiology communities have been characterized by anger and discord. Despite the frequently negative relationships among the member societies, the individual MSOHG members have developed outstanding working relationships, based on a profound respect and admiration for each other. Working as a team, this committee has identified a number of areas of mutual interest. We have worked diligently to find agreement in our approach and objectives, and collaborated constructively to develop an ongoing program with important objectives. It may not be clear immediately to all readers, but the diplomatic detente we have forged is singular within medical circles. The constructive nature of this alliance can serve as an example for intersocietal relations. This committee can serve as a unique resource for our societies to find common ground for our mutual benefit.Summary
The interventional laboratory presents occupational hazards to operators and staff that must be acknowledged, understood, and mitigated to the greatest extent possible. In a truly collaborative effort among the member societies, the MSOHG has made considerable progress toward this end in the past 5 years through interactions with manufacturers and national and international organizations. Much remains to be done, but a beginning has been achieved.References
- Klein LW, Miller DL, Balter S, et al. Occupational health hazards in the interventional laboratory: time for a safer environment. J Vasc Interv Radiol 2009;20:147–152.
- Yoshinaga S, Mabuchi K, Sigurdson AJ, Doody MM, Ron E. Cancer risks among radiologists and radiologic technologists: review of epidemiologic studies. Radiology 2004; 233:313–321.
- Sigurdson AJ, Doody MM, Rao RS, et al. Cancer incidence in the US radiologic technologists health study, 1983–1998. Cancer 2003; 97:3080–3089.
- Kleiman NJ. Radiation cataract. In: Working Party on Research Implications on Health and Safety Standards of the Article 31 Group of Experts, eds. Radiation Protection 145. EU Scientific Seminar 2006: new insights in radiation risk and basic safety standards. Brussels: European Commission, 2007; 81–95. Available at: https://ec.europa.eu/energy/nuclear/radioprotection/publication/doc/145_en.pdf Accessed May 18, 2010.
- Vano E, Gonzalez L, Fernández JM, Haskal ZJ. Eye lens exposure to radiation in interventional suites: caution is warranted. Radiology 2008; 248:945–953.
- Vaño E, Gonzalez L, Fernandez JM, Alfonso F, Macaya C. Occupational radiation doses in interventional cardiology: a 15-year follow-up. Br J Radiol 2006; 79:383-388.
- Miller DL, Vañó E, Bartal G, et al. Occupational radiation protection in interventional radiology: a joint guideline of the Cardiovascular and Interventional Radiology Society of Europe and the Society of Interventional Radiology. Cardiovasc Intervent Radiol 2010; 33:230 –239.
- National Council on Radiation Protection and Measurements. Ionizing radiation exposure of the population of the United States. NCRP Report No. 160. Bethesda, MD: National Council on Radiation Protection and Measurements, 2009.
- National Council on Radiation Protection and Measurements. Use of personal monitors to estimate effective dose equivalent and effective dose to workers for external exposure to low-LET radiation. NCRP Report No. 122. Bethesda, MD: National Council on Radiation Protection and Measurements, 1995.
- Marx MV, Niklason L, Mauger EA. Occupational radiation exposure to interventional radiologists: a prospective study. J Vasc Interv Radiol 1992; 3:597–606.
