


An Objective Allen’s Test
Today’s invasive vascular procedures demand trustworthy documentation of adequate collateral flow in the human palmar arch. For years, the modified Allen’s test1 served as the quick bedside test of radial and ulnar collateral flow to the hand. We know now that the Allen’s test is both subjective and insensitive.2-4 When a radial or ulnar artery is harvested for coronary grafting or dialysis fistula creation, it is imperative to document collateral flow to the fingers. Angiography and Doppler studies, currently used for this purpose, are both expensive and require technical expertise.5 Cannulation of the radial artery for continuous blood pressure monitoring and arterial phlebotomy is a popular procedure employed in the surgical suite and intensive care units. Embarrassment of flow to the thumb remains an important risk of even these temporary radial artery manipulations.6,7
Photoplethysmography (PPG) has been used by others to assess peripheral arterial blood flow.8,9 For our exams, we use a PPG device, FloChec™ (Semler Scientific, Inc., Portland, Oregon).10 The FloChec interfaces with standard computers to provide both a hard copy and a digital analysis that can be embedded into an electronic medical record.
The thumb (first digit) is essential for pinching, grasping, playing instruments and many other tasks. Because of its reliance on the princeps pollicis artery (the principal artery of the thumb), it is vulnerable to inadequate palmar collateral flow; therefore, one must confirm complete arterial compression (no blood flow to the thumb) when compressing both the radial and ulnar artery during any form of a modified Allen’s test. Likewise, one must unambiguously document the presence or absence of reperfusion upon release of the ulnar artery.
Methods
With the palm up and the hand resting on a flat surface, the PPG sensor is placed snugly on the thumb with the infrared light source and receptor touching the pad portion of the thumb. After ten seconds of baseline flow, both radial and ulnar arteries are compressed at the wrist for ten seconds. If compression is complete, in real time, the FloChec shows flow to the thumb dropping dramatically. At twenty seconds, the ulnar compression is released. If the princeps pollicis artery receives any contribution from the ulnar artery, the FloChec will reflect a return of pulsatile flow to the thumb. After ten more seconds (30-second mark) the ulnar artery is again compressed along with the radial artery for another ten seconds. At the 40-second mark, the radial artery alone is opened. At the 50-second mark, both arteries are opened and the flow should return to baseline.
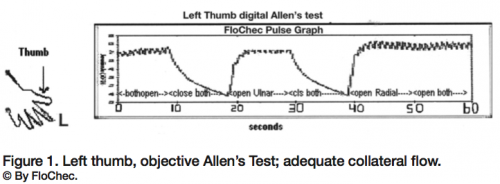 Twenty adult medical volunteers were tested using the FloChec-derived objective Allen’s test. Of the 40 hands tested, one was “abnormal” and two were “inconclusive.” The 37 remaining hands displayed markedly similar “normal” graphic results (Figure 1). The two “inconclusive” tests belonged to one patient with chronic Raynaud’s phenomenon. This demonstrates an inherent limitation of plethysmographic technology.
Twenty adult medical volunteers were tested using the FloChec-derived objective Allen’s test. Of the 40 hands tested, one was “abnormal” and two were “inconclusive.” The 37 remaining hands displayed markedly similar “normal” graphic results (Figure 1). The two “inconclusive” tests belonged to one patient with chronic Raynaud’s phenomenon. This demonstrates an inherent limitation of plethysmographic technology.
The first graph (Figure 1), generated by FloChec, shows the typical adequate collateral flow pattern.8 Both the ulnar artery alone and then the radial artery alone supply pulsatile flow to the left thumb.
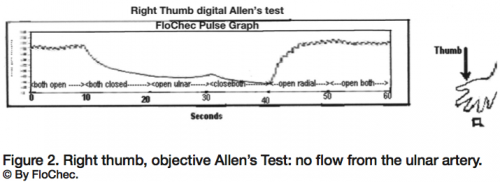 One hand, though, showed the absence of collateral flow to the right thumb. Mr. RM is a healthy 58-year-old Caucasian male volunteer. He is normotensive, with no vascular risk factors such as diabetes mellitus, dyslipidemia, obesity, injury, or family history of vascular compromise. His left-hand graphic was similar to above and was considered “normal.” The graphic of the right hand failed to show any contribution from the ulnar artery to pulsatile flow of his thumb (Figure 2).
One hand, though, showed the absence of collateral flow to the right thumb. Mr. RM is a healthy 58-year-old Caucasian male volunteer. He is normotensive, with no vascular risk factors such as diabetes mellitus, dyslipidemia, obesity, injury, or family history of vascular compromise. His left-hand graphic was similar to above and was considered “normal.” The graphic of the right hand failed to show any contribution from the ulnar artery to pulsatile flow of his thumb (Figure 2).
Conclusion
This patient has no ulnar artery contribution to the princeps pollicis artery of his right thumb.
In this same volunteer, a subjective modified Allen’s test was performed with ambiguous results (i.e., the right palm flushed @ 8 seconds, while the left palm flushed @ 6 seconds). As demonstrated here, the vascular anatomy of a patient’s hands may not be symmetrical.
Discussion
Radial dominance to the princeps pollicis artery occurs in approximately 87% of hands, but “radial-dependent” anatomy occurs in < 5% of hands.5,11 The consequences of missing radial-dependent architecture can be devastating.
In this series of patients, we discovered a case of absent collateral flow in the palmar arch. We did not subsequently test the subject with the Doppler. (An arterial angiogram would also define the vasculature.) We recognize that Doppler is currently the standard test, and do recognize the limitations of FloChec, which are shared by every other plethysmographic device. For plethysmography to “work,” there must be pulsatile arterial flow. If there is peripheral spasm (as in Raynaud’s or hypothermia) or small vessel disease (diabetes mellitus, multiple sclerosis, or Buerger’s), the device results may be inconclusive. Furthermore, if there is cardiogenic shock or proximal vascular occlusion, the measurable flow may also be too low to interpret. These later diseases will diminish the sensitivity of Doppler technology as well.
Nevertheless, as a simple, quick, and low-cost bedside screening test, FloChec surpasses the Doppler apparatus. It generates both paper and computerized record, can be employed with any laptop computer, and can be administered without advanced formal training.
 By using the PPG function with a computer, the FloChec provides documentable objectivity to the modified Allen’s test.8 We use this device interfacing with a portable, battery-powered PC Netbook computer (Figure 3). The compact and portable qualities of FloChec enable this assessment in the office setting, at the hospital bedside, in the pre-op clinic or operating room.
By using the PPG function with a computer, the FloChec provides documentable objectivity to the modified Allen’s test.8 We use this device interfacing with a portable, battery-powered PC Netbook computer (Figure 3). The compact and portable qualities of FloChec enable this assessment in the office setting, at the hospital bedside, in the pre-op clinic or operating room.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
The authors can be contacted at tftolan@comcast.net.
References
- Allen EV. Thromboangiitis obliterans; methods of diagnosis of chronic occlusive arterial lesion distal to the wrist with illustrative cases. Am J Med Sci 1929;178:237–244.
- Jarvis MA, Jarvis CL, Jones PR, Spyt TJ. Reliability of Allen’s test in selection of patients for radial artery harvest. Ann Thorac Surg 2000 Oct;70(4): 1362–1365.
- Cheng EY, Lauer KK, Stommel KA, Guenther NR. Evaluation of the palmer circulation by pulse oximetry. J Clin Monit 1989;5:1–3.
- Greenhow DE. Incorrect performance of Allen’s test: ulnar artery flow erroneously presumed adequate. Anesthesiology 1972;37:356–357.
- Kleinert JM, Fleming SG, Abel CS, Firrell J. Radial and ulnar artery dominance in normal digits. J Hand Surg 1989;14A:594–598.
- Downs JB, Rackstein AD, Klein EF Jr., Hawkins IF Jr. Hazards of radial artery catheterization. Anesthesiology 1973;38:283–286.
- Gardner RM, Schwartz RN, Wong HC, Burke JP. Percutaneous indwelling radial-artery catheters for monitoring cardiovascular function: Prospective study of the risk of thrombosis and infection. N Engl J Med 1974;290:1227–1231.
- Stead SW, Stirt JA. Assessment of digital blood flow and palmar collateral circulation. Allen’s test vs. photoplethysmography. Int J Clin Monit Comput 1985;2:29–34.
- Semler HJ, et al. A novel method for identifying patients with peripheral artery disease. Thirteenth World Congress on Heart Disease; Vancouver, B.C., Canada, July 28-31, 2007.
- Semler Scientific Inc., 2330 NW Everett, Portland, Oregon 97210.
- Coleman SS, Anson BJ. Arterial patterns in the hand based upon a study of 650 specimens. Surg Gynec and Obstet 1961;113:409–424.
Disclosure: Tod Tolan, MD, and Gil Tolan, MD, have no conflicts of interest regarding the content herein. Herb Semler, MD, reports he is an initiator and principal in Semler Scientific, Inc., the producer of FloChec®. Phillip Benz, MBA, MPH, reports he has worked with Semler Scientific during the early development of FloChec. He does not currently work for Semler Scientific, Inc.
