


New Wire-Retained Method to Performing the Pre-Close Technique of Percutaneous Closure During Large-Bore Femoral Procedures
 Large-bore vessel sheaths are being utilized more frequently in the cardiac catheterization laboratory, especially with the advent of newer technologies which demand larger bore sheaths, such as the Impella 2.5 ventricular assist device (Abiomed, Danvers, Mass.), endovascular abdominal aortic aneurysm (AAA) stent grafts, and transfemoral percutaneous aortic valves. With the need for these large-bore sheaths, there has been a growing need to devise techniques to effectively provide hemostasis at the femoral arteriotomy site. The most widely utilized technique to perform closure of the femoral arteriotomy has been the Pre-Close technique1,2, which has involved the use of two sequentially deployed Perclose ProGlide suture-mediated closure devices (Abbott Vascular, Redwood City, Calif.). We describe a modification to the described Pre-Close technique, which saves a few procedural steps, and can theoretically be safer to the patient.
Large-bore vessel sheaths are being utilized more frequently in the cardiac catheterization laboratory, especially with the advent of newer technologies which demand larger bore sheaths, such as the Impella 2.5 ventricular assist device (Abiomed, Danvers, Mass.), endovascular abdominal aortic aneurysm (AAA) stent grafts, and transfemoral percutaneous aortic valves. With the need for these large-bore sheaths, there has been a growing need to devise techniques to effectively provide hemostasis at the femoral arteriotomy site. The most widely utilized technique to perform closure of the femoral arteriotomy has been the Pre-Close technique1,2, which has involved the use of two sequentially deployed Perclose ProGlide suture-mediated closure devices (Abbott Vascular, Redwood City, Calif.). We describe a modification to the described Pre-Close technique, which saves a few procedural steps, and can theoretically be safer to the patient.
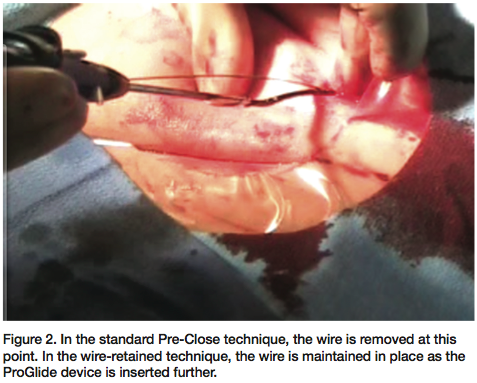 The traditional method to deploy a ProGlide suture-mediated closure device during large-bore vessel closure involves placing a long 0.035” wire through an existing sheath, removing the sheath, and then advancing the ProGlide suture-mediated closure device over the wire until the wire exits through the marked wire port. Once the ProGlide device is advanced so that the wire port is at the level of the puncture site, the wire is removed, and the ProGlide device is inserted further, until the bleed back marker demonstrates suitable position for suture deployment. The sutures are then deployed in the traditional fashion, and then the ProGlide device is withdrawn until the wire port is visible. At this time, the 0.035” wire is re-introduced, the device is removed, and another device is inserted over the wire. The same routine is then performed as described above to deploy the second device.
The traditional method to deploy a ProGlide suture-mediated closure device during large-bore vessel closure involves placing a long 0.035” wire through an existing sheath, removing the sheath, and then advancing the ProGlide suture-mediated closure device over the wire until the wire exits through the marked wire port. Once the ProGlide device is advanced so that the wire port is at the level of the puncture site, the wire is removed, and the ProGlide device is inserted further, until the bleed back marker demonstrates suitable position for suture deployment. The sutures are then deployed in the traditional fashion, and then the ProGlide device is withdrawn until the wire port is visible. At this time, the 0.035” wire is re-introduced, the device is removed, and another device is inserted over the wire. The same routine is then performed as described above to deploy the second device.
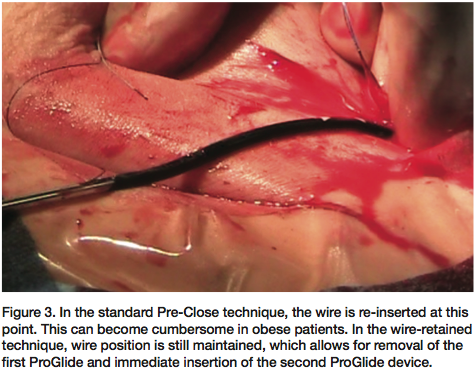 Re-introduction of the wire through the marked wire port can, many times, become time consuming, as the existing J shape on the wire must be straightened in order to introduce it through the wire port, and the ProGlide device must be situated such that the wire port faces upright, with care being taken not to pull the device back too far. During this step, an additional factor that tends to obscure visibility of the wire port is the presence of bleeding from the arteriotomy site, which then requires additional use of hands to apply pressure on the groin. In obese patients, this can become somewhat cumbersome.
Re-introduction of the wire through the marked wire port can, many times, become time consuming, as the existing J shape on the wire must be straightened in order to introduce it through the wire port, and the ProGlide device must be situated such that the wire port faces upright, with care being taken not to pull the device back too far. During this step, an additional factor that tends to obscure visibility of the wire port is the presence of bleeding from the arteriotomy site, which then requires additional use of hands to apply pressure on the groin. In obese patients, this can become somewhat cumbersome.
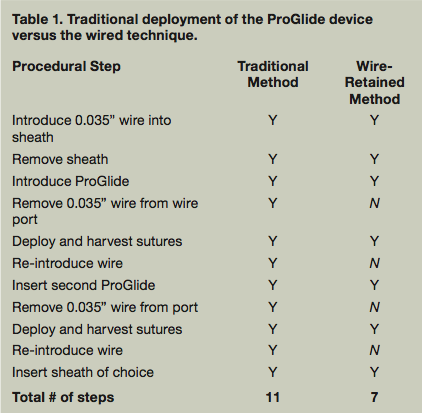 We have successfully performed the Pre-Close technique by eliminating the wire removal step. Once our wire has been placed in the sheath and the sheath has been removed, we proceed with the traditional steps as described above. Once the ProGlide device has been advanced such that the wire port is at the level of the puncture site, we continue to advance the device, with the wire remaining in the wire port. Gentle tension is maintained on the wire to ensure that the ProGlide device’s catheter rides adjacent to the wire, without the potential to introduce any slack in the wire. Once bleeding is confirmed in the bleed port, the foot processes are extended. The device and wire are then pulled back as a unit until the device is in a suitable position for suture deployment. The sutures are then deployed in the traditional fashion. Then the ProGlide device is pulled back until the wire port exits the skin surface. At this point, the device is removed, and wire access is maintained, allowing for immediate insertion of the next device. Table 1 summarizes the differences between the traditional deployment of the ProGlide device and the wired technique.
We have successfully performed the Pre-Close technique by eliminating the wire removal step. Once our wire has been placed in the sheath and the sheath has been removed, we proceed with the traditional steps as described above. Once the ProGlide device has been advanced such that the wire port is at the level of the puncture site, we continue to advance the device, with the wire remaining in the wire port. Gentle tension is maintained on the wire to ensure that the ProGlide device’s catheter rides adjacent to the wire, without the potential to introduce any slack in the wire. Once bleeding is confirmed in the bleed port, the foot processes are extended. The device and wire are then pulled back as a unit until the device is in a suitable position for suture deployment. The sutures are then deployed in the traditional fashion. Then the ProGlide device is pulled back until the wire port exits the skin surface. At this point, the device is removed, and wire access is maintained, allowing for immediate insertion of the next device. Table 1 summarizes the differences between the traditional deployment of the ProGlide device and the wired technique.
The wired approach to ProGlide deployment appears to work effectively, and technically appears to be more efficient, especially when multiple devices need to be deployed. By leaving the wire in place, the cumbersome task of trying to straighten a J wire and re-introduce it through the wire port is eliminated. This can prove to substantially save time and effort, especially in the case of a patient who tends to have oozing from the puncture site once the first device is deployed, and most importantly, in our obese patients. This technique can also prove to be safer, as the traditional method of inserting the ProGlide device involves inserting the distal portion of the device further into the vessel without a wire to rail over. Even though the distal end of the catheter is soft and atraumatic, there is always potential for lifting plaque during the procedural step of inserting the ProGlide catheter further into the vessel without wire support.
This article received double-blind peer review from members of the Cath Lab Digest editorial board.
The authors can be contacted via Dr. Mirvat Alasnag at mirvat@jeddacath.com.
Disclosure: Dr. Alasnag and Dr. Umakanthan report no conflicts of interest regarding the content herein.
References
- Lee, WA. Access for TEVAR. The Preclose technique and the Proglide device offer safe and effective percutaneous access for thoracic endovascular aortic repair. Endovascular Today 2008 Sept: 48-55.
- Michaels, AD, Ports, TA. Use of a percutaneous arterial suture device (Perclose) in patients undergoing balloon aortic valvuloplasty. Cathet Cardiovasc Intervent 2001;53:445-447.
