


Management of an Unusual Cause of Refractory Hypertension: “Middle Aortic Syndrome”
Abstract
“Middle aortic syndrome” is a rare cause of hypertension. It typically leads to stenosis of the lower thoracic and upper abdominal aorta with or without involvement of renal arteries. Mid-aortic syndrome is a rare condition, comprising 0.5%–2.0% of aortic coarctations. This multifactorial condition needs to be ruled out in younger patients presenting with hypertension. We describe a case of middle aortic syndrome secondary to Takayasu’s aortoarteritis in a 20-year-old female and its successful management using percutaneous intervention with deployment of self-expanding stent. Percutaneous intervention in such cases has a higher success rate, offering fewer complications, clinical improvement of symptoms, and control of a cause of hypertension.
Introduction
Congenital coarctation of the thoracic aorta is well recognized, but a much less common variety of aortic coarctation is located in the distal thoracic aorta, abdominal aorta, or both, and is called “middle aortic syndrome.”1,2
Middle aortic syndrome is an unusual cause of arterial hypertension in the upper extremities secondary either to a congenital anomaly in the development of the aorta or to one of several acquired conditions.3,4 Acquired conditions include neurofibromatosis, retroperitoneal fibrosis, fibromuscular dysplasia, mucopolysaccharidosis, and Takayasu’s arteritis, all of which may result in narrowing of the abdominal aorta and other vessels.4
We describe the case of a 20-year-old female who presented with refractory hypertension and claudication on walking, who underwent percutaneous intervention using a stent that not only ameliorated her symptoms, but also eliminated her hypertension.
Case report
A 20-year-old female was admitted with complaints of increased neck pulsations and easy fatigability. She gave a history of bilateral lower limb claudication on walking.
Examination revealed bounding upper limb pulses and feeble lower limb pulses. Blood pressure recorded in both upper limbs was 220/60 mmHg and in both lower limbs, 100/60 mmHg. She was taking four anti-hypertensive
medications (a beta blocker, calcium channel blocker, clonidine and thiazide diuretic). Cardiovascular examination revealed normal heart sounds and no murmur. There were no palpable pulsations over the abdomen, but an abdominal bruit could be heard in the midepigastric area, with no radiation.
Laboratory investigations revealed a normal hemogram with acute phase reactants including an erythrocyte sedimentation rate (ESR) of 25 mm at the end of the first hour and a negative C-reactive protein (CRP) test. An abdominal ultrasound showed a small abdominal aorta with diffuse narrowing and an increased peak systolic velocity (412 cm/s). The presence of runoff flow throughout the entire diastole was also noted, with a significant gradient of 120 mmHg across it. Bilateral renal Doppler showed normal reno-vasculature. An electrocardiogram showed left ventricular hypertrophy by voltage criteria with left atrial overload. An echocardiogram showed moderate left ventricular hypertrophy and preserved systolic function.
Catheterization and aortic angiography (transradial and transfemoral study) using digital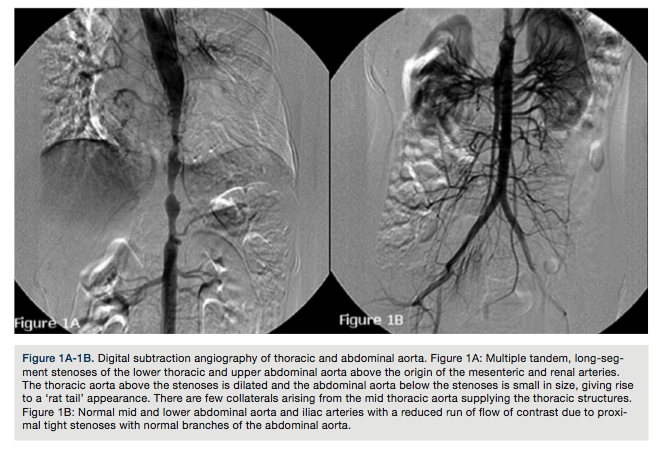 subtraction angiography showed a severe stenosis involving the distal thoracic and upper abdominal aorta above the renal arteries (Figures 1A and 1B). There was a pullback gradient of 100 mmHg from the ascending aorta to the descending abdominal aorta. The renal and mesenteric vasculature was normal.
subtraction angiography showed a severe stenosis involving the distal thoracic and upper abdominal aorta above the renal arteries (Figures 1A and 1B). There was a pullback gradient of 100 mmHg from the ascending aorta to the descending abdominal aorta. The renal and mesenteric vasculature was normal.
After diagnosis, a management strategy was discussed with the rheumatologist, interventional cardiologist, vascular surgeon, and cardiothoracic surgeons. It was decided to proceed with percutaneous transluminal angioplasty with stenting. The patient also opted for the interventional option in view of cosmetic reasons.
The stenotic lesion measured 110 mm in length with proximal diameter of 18 mm and distal diameter of 12 mm. Oral aspirin 150 mg and clopidogrel 75 mg once a day were begun 24 hours before the procedure. During the procedure, the patient received a bolus of 5000 IU of heparin. The right radial artery was canulated using a 5 French radial sheath for aortic angiography using a pigtail catheter. Right femoral artery cannulation used a 5 French radial sheath exchanged for a 7 French femoral sheath. A 16 x 120 mm E-Luminexx self-expanding stent (C. R. Bard, Inc.) was positioned over an Amplatzer stiff wire. The stent was positioned under angiographic guidance and released gradually. After deployment of the stent, areas of under expansion still existed. Hence, the stent was post dilated using a 14 x 40 mm Atlas balloon (C. R. Bard, Inc.) (Figures 2a-2f).
Final angiogram revealed no residual stenosis with a brisk normal aortic flow pattern. The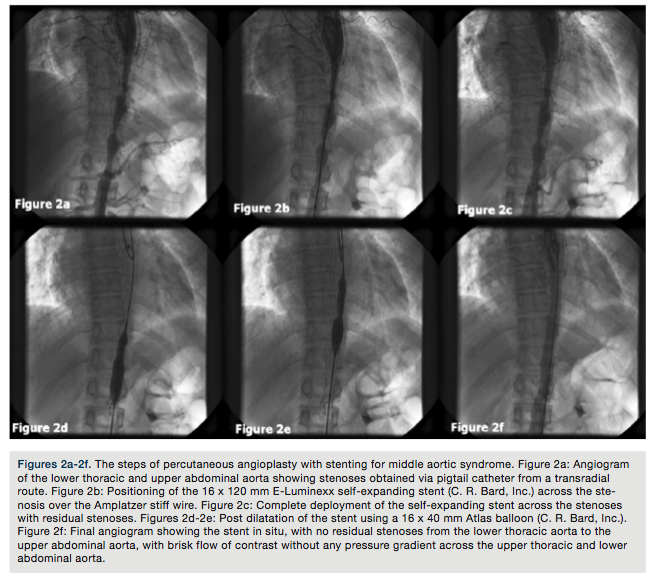 gradient disappeared completely. The patient has completed 6-month follow-up with no symptoms. With the patient on one prescribed anti-hypertensive, blood pressure was 140/90 mmHg, with palpable lower limb pulses.
gradient disappeared completely. The patient has completed 6-month follow-up with no symptoms. With the patient on one prescribed anti-hypertensive, blood pressure was 140/90 mmHg, with palpable lower limb pulses.
Discussion
The term “middle aorta syndrome” was first used by Sen et al1 to describe narrowing of the sub-isthmal aorta, in distinction to the Takayasu’s-type aortic arch and Leriche-type aortic bifurcation obliterative disease.1,5 In an earlier series, these stenoses were grouped at two distinct sites — in the supra-diaphragmatic aorta within a few centimeters of the diaphragm, and below the diaphragm, with frequent involvement of the visceral and renal branches of the upper abdominal aorta.1
The name ‘’coarctation’’ implies a congenital origin; some authors prefer a more neutral name, such as “middle aortic syndrome”.6
In one-third of patients, the onset of symptoms commonly occurs at a very early age.7 Mid-aortic syndrome is a rare condition, comprising 0.5%-2.0% of aortic coarctations.8,9
When inflammation is in the burned-out state, patients with middle aortic syndrome who have symptomatic reno-vascular hypertension, claudication, or both, are good candidates for revascularization, with a high expectation for long-term reversal of end-organ dysfunction.7
The mean age at diagnosis is 20.7 years, with a second peak during the fourth or fifth decade. Renal artery stenosis is found in 80% of patients, and 25% have involvement of the superior mesenteric artery, inferior mesenteric artery, or celiac axis.10 Modalities to treat include surgery, bypass grafts, auto-transplantation of kidneys and percutaneous transluminal angioplasty. Surgical reconstruction is a definitive procedure with a high incidence of suture line complications, including aneurysm formation.9,10
Open surgery is the primary treatment of middle aortic syndrome and is associated with reno-vascular hypertension and visceral artery stenosis. It entails aorto-aortic bypass of the diseased segment or, less often, patch aortoplasty, and usually bypass grafting of the stenosed renal and visceral arteries performed with autologous conduits. Hypertension is thus improved or cured in more than 70% of patients.9 Patients require clinical follow-up once in three months with measurement of blood pressure in the upper and lower limbs for possible restenosis. A computed tomography (CT) scan would be performed only if clinically indicated.
For long-segment lesions, chronic total occlusions, and ostial lesions, an unsatisfactory result with percutaneous transluminal angioplasty can be improved by stenting. Stenting has increased the procedural success rates, achieved larger luminal diameter and seems to decrease the incidence of restenosis, particularly in Takayasu’s aortoarteritis.10
In our patient, the stent size was selected with a diameter 2 mm smaller than the proximal diameter in order to avoid over-dilation and dissection of the lower end, as it was smaller than the upper end.
Conclusion
This case highlights: 1) the importance of a thorough physical examination, which raised the suspicion of aortic coarctation or renal artery stenosis as the cause of hypertension; and 2) coarctation of the abdominal aorta, although rare, can be the cause of secondary hypertension and should be considered during the diagnostic workup of hypertension, especially in young patients.
Disclosure: The authors report no conflicts of interest regarding the content herein.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
The authors may be contacted via Dr. Pankaj V. Jariwala at pankaj_jariwala@hotmail.com.
References
- Watson NA, Chalmers N, Naqvi N. Supradiaphragmatic middle aorta syndrome--MR and angiographic imaging. Br J Radiol. 1998 Feb; 71(842): 213-216.
- Fujino S, Mabuchi T, Yoshida S, et al. Emergent thoracic aortic angioplasty and stenting for middle aortic syndrome in non-specific aortitis. Cardiovasc Interv Ther. 2010 Feb; 25(2): 117-121.
- Bialkowski J, Szkutnik M, Bermúdez-cañete R, et al. Middle aortic syndrome caused by Takayasu’s disease and treated by stent implantation: a report of medium-term follow-up. Revista Española de Cardiologia. 2002; 55: 1-4.
- Daghero F, Bueno N, Peirone A, et al. Coarctation of the abdominal aorta: an uncommon cause of arterial hypertension and stroke. Circ Cardiovasc Imaging. 2008; 1(1): e4-e6.
- Sen PK, Kinare SG, Engineer SD, Parulkar GB. The middle aortic syndrome. Heart. 1963 Sep; 25(5): 610-618.
- Alehan D, Kafali G, Demircin M. Middle aortic syndrome as a cause of dilated cardiomyopathy. Anadolu Kardiyol Derg. 2004 Jun; 4(2): 178-180.
- Connolly JE, Wilson SE, Lawrence PL, Fujitani RM. Middle aortic syndrome: distal thoracic and abdominal coarctation, a disorder with multiple etiologies. J Am Coll Surg. 2002 Jun; 194(6): 774-781.
- Matsumoto M, Suehiro K, Kubo H. Ascending aorta-abdominal aorta bypass with the reconstruction of superior mesenteric and bilateral renal arteries for mid-aortic syndrome. Jpn J Thorac Cardiovasc Surg. 2006 Dec;54(12):535-538.
- Delis KT, Gloviczki P. Middle aortic syndrome: from presentation to contemporary open surgical and endovascular treatment. Perspect Vasc Surg Endovasc Ther. 2005 Sep; 17(3): 187-203.
- Gomes R, Rossi R, Lima S, Carmo P, Ferreira R, Menezes I, et al. Pediatric cardiology and telemedicine: seven years’ experience of cooperation with remote hospitals. Rev Port Cardiol. 2010 Feb; 29(2): 181-191.
