


Left Internal Mammary Artery Graft to Contralateral Subclavian Steal Syndrome
 Abstract: A coronary-ipsilateral subclavian steal phenomenon has been described in patients who have undergone prior coronary artery bypass surgery (CABG) utilizing the left internal mammary artery (LIMA). In the presence of a hemodynamically significant subclavian artery stenosis proximal to the origin of the ipsilateral IMA, flow through the IMA may reverse and “steal” flow from the coronary circulation during upper extremity exercise. We present a very unique case of left internal mammary artery (LIMA) graft–contralateral subclavian steal phenomenon.
Abstract: A coronary-ipsilateral subclavian steal phenomenon has been described in patients who have undergone prior coronary artery bypass surgery (CABG) utilizing the left internal mammary artery (LIMA). In the presence of a hemodynamically significant subclavian artery stenosis proximal to the origin of the ipsilateral IMA, flow through the IMA may reverse and “steal” flow from the coronary circulation during upper extremity exercise. We present a very unique case of left internal mammary artery (LIMA) graft–contralateral subclavian steal phenomenon.
Case
A 61-year-old Caucasian female with known history of coronary artery bypass grafting (CABG) 12 years prior was referred for coronary angiography secondary to jaw pain and shortness of breath with exertion, both relieved with sublingual nitroglycerine. At the time of presentation, she was found to have unequal blood pressures bilaterally and noted to have bilateral carotid and subclavian bruits. Subclavian and carotid duplex ultrasound confirmed right brachiocephalic artery occlusion with low internal carotid artery velocities (peak systolic velocity – 39 cm/sec; end diastolic velocity – unable to measure) and retrograde flow in the right vertebral artery.
 Aortic angiography revealed a heavily calcified porcelain arch with patent saphenous vein grafts. The left anterior descending artery (LAD) was noted to have a proximal 80% stenosis with retrograde flow from mid vessel into the patent left internal mammary artery (LIMA) graft. Both the left circumflex and right coronary arteries were 100% occluded proximally. The LIMA to LAD graft was patent with competitive retrograde flow from the native LAD and a large collateral noted from the proximal graft supplying the right subclavian and right carotid arteries
Aortic angiography revealed a heavily calcified porcelain arch with patent saphenous vein grafts. The left anterior descending artery (LAD) was noted to have a proximal 80% stenosis with retrograde flow from mid vessel into the patent left internal mammary artery (LIMA) graft. Both the left circumflex and right coronary arteries were 100% occluded proximally. The LIMA to LAD graft was patent with competitive retrograde flow from the native LAD and a large collateral noted from the proximal graft supplying the right subclavian and right carotid arteries 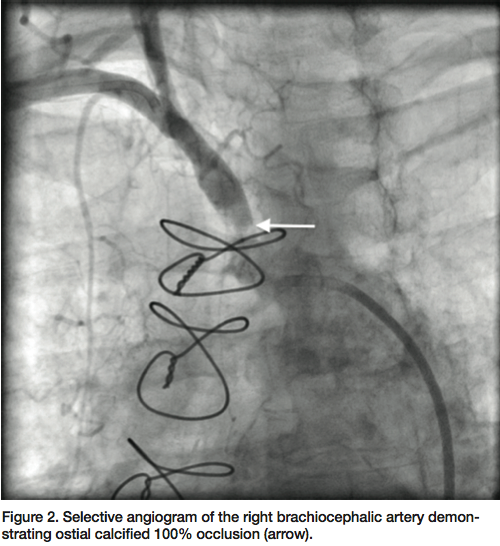 (Figure 1). The right brachiocephalic artery was observed to be heavily calcified, with a 100% ostial occlusion (Figure 2). At this point, a decision was made to intervene on the right brachiocephalic artery occlusion to allow antegrade flow into the right subclavian and carotid arteries to relieve the apparent steal phenomenon from the LIMA-LAD graft.
(Figure 1). The right brachiocephalic artery was observed to be heavily calcified, with a 100% ostial occlusion (Figure 2). At this point, a decision was made to intervene on the right brachiocephalic artery occlusion to allow antegrade flow into the right subclavian and carotid arteries to relieve the apparent steal phenomenon from the LIMA-LAD graft.
Access was secured in the right brachial artery and right common femoral artery with 6 French 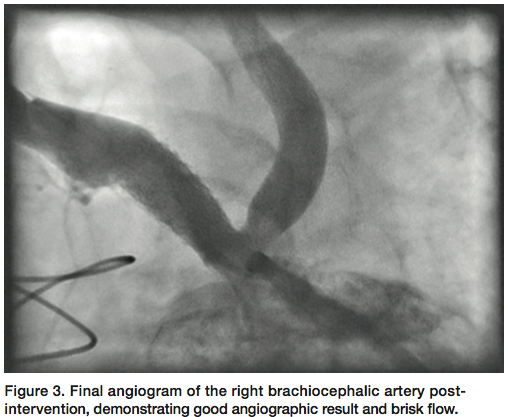 (Fr) and 7 Fr sheaths, respectively. A V-18 wire (Boston Scientific) was advanced with support of a Sterling 4 x 20 mm balloon (Boston Scientific) to cross the right brachiocephalic artery occlusion into the aorta. Selective angiogram through the balloon into the aorta confirmed an intraluminal position in the aortic arch. After serial dilatations, an iCAST (Atrium) 7 x 22 mm covered stent was deployed at the ostium of the right brachiocephalic artery at 14 atm, with good expansion. Final angiogram after post-dilation confirmed brisk flow through the stented segment (Figure 3). Subsequent angiogram of the LIMA graft revealed brisk
(Fr) and 7 Fr sheaths, respectively. A V-18 wire (Boston Scientific) was advanced with support of a Sterling 4 x 20 mm balloon (Boston Scientific) to cross the right brachiocephalic artery occlusion into the aorta. Selective angiogram through the balloon into the aorta confirmed an intraluminal position in the aortic arch. After serial dilatations, an iCAST (Atrium) 7 x 22 mm covered stent was deployed at the ostium of the right brachiocephalic artery at 14 atm, with good expansion. Final angiogram after post-dilation confirmed brisk flow through the stented segment (Figure 3). Subsequent angiogram of the LIMA graft revealed brisk 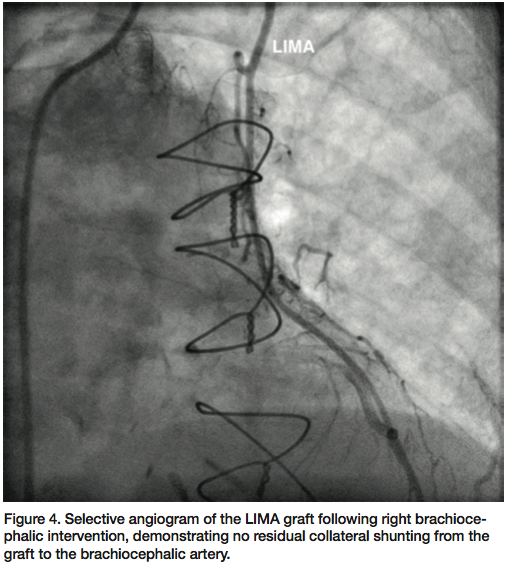 flow through the graft into the distal LAD (Figure 4). Follow-up carotid ultrasound showed peak systolic and diastolic velocities in the right internal carotid artery to be 149 and 36, respectively, with antegrade flow in the vertebral artery.
flow through the graft into the distal LAD (Figure 4). Follow-up carotid ultrasound showed peak systolic and diastolic velocities in the right internal carotid artery to be 149 and 36, respectively, with antegrade flow in the vertebral artery.
Discussion
A physiologic steal occurs when there is a pressure gradient between the donor and recipient arteries.1 LIMA graft-ipsilateral subclavian steal phenomenon has been described in patients who have undergone prior CABG utilizing the LIMA.2,3 The IMA originates from the subclavian artery, and blood flow is dependent on inflow by the vessels in the aortic arch.4 In the presence of a hemodynamically significant subclavian artery stenosis proximal to the origin of the ipsilateral IMA, flow through the IMA may reverse and “steal” flow from the coronary circulation during upper extremity exercise. The incidence of coronary-subclavian steal syndrome (CSSS) is less than 0.5 %.5,6 While atherosclerosis is the most common cause of steal syndrome, Takayasu’s arteritis, congenital aortic anomalies, and thoracic outlet syndrome have also been described as possible etiologies.7
The typical symptom of CSSS is angina, which depends on the degree of subclavian artery stenosis or occlusion and physical activity of the patient, but myocardial infarction is rare.4 A blood pressure differential between arms or a gradient across the lesion of more than 20 mm Hg is considered to be a clinically significant stenosis. Arch aortography and selective subclavian angiography are the gold standard for diagnosis, while Doppler, duplex ultrasonography, computed tomography, or magnetic resonance imaging, are all viable options as well.8
The treatment of choice for CSSS is percutaneous transluminal angioplasty with stent placement.8 If a percutaneous strategy is not feasible, surgical therapy including carotid-subclavian bypass or direct endarterectomy may be alternatives.
Our case report is a first of its kind where the right subclavian artery was involved in a steal phenomenon from the left internal mammary artery graft. It would appear that the symptoms of myocardial ischemia are likely to be the result of hemodynamic changes caused by functional coronary steal into the right subclavian artery and its branches. At follow up visit post-intervention, she did not exhibit any recurrence of anginal symptoms.
Dr. Jon George can be contacted at georgej@deborah.org.
References
- Elian D, Gerniak A, Guetta V, Jones M, Agranat O, Har-Zahav Y, et al. Subclavian coronary steal syndrome: an obligatory common fate between subclavian artery, internal mammary graft and coronary circulation. Cardiology. 2002; 97:175-179.
- Ochi M, Yamauchi S, Yajima T, et al. Simultaneous subclavian artery reconstruction in coronary artery bypass grafting. Ann Thorac Surg. 1997; 63: 1284.
- Takach TJ, Beggs ML, Nykamp VH, Reul GJ Jr. Concomitant cerebral and coronary subclavian steal. Ann Thorac Surg. 1997; 63: 853.
- Mandak J, Lojik M, Tuna M, Chek JL. Coronary subclavian steal syndrome causing acute myocardial infarction in a patient undergoing coronary-artery bypass grafting. Case Report Med. 2012; 798356.
- Tyras DH, Barner HB. Coronary-subclavian steal. Arch Surg. 1977; 112: 1125-1127.
- Takachi TJ, Reul GJ, Gregoric I, Krajcer Z, Duncan JM, Livesay JJ, et al. Concomitant subclavian and coronary artery disease. Ann Thorac Surg. 2001; 71: 187-189.
- Cardon A, Leclercq C, Brenugat S, Jego P, Kerdiles Y. Coronary subclavian steal syndrome after left internal mammary bypass in a patient with Takayasu’s disease. J Cardiovasc Surg. 2002; 43(4): 471-473.
- Wright IA, Laing AD, Buckenham TM. Coronary subclavian steal syndrome: non-invasive imaging and percutaneous repair. Brit J Radiol 2004; 77(917): 441-444.
