Isolated Single Coronary Artery in a Patient Presenting with an Abnormal ECG
A 45-year-old male with a history of hypertension, exertional and self-limiting chest pain, and an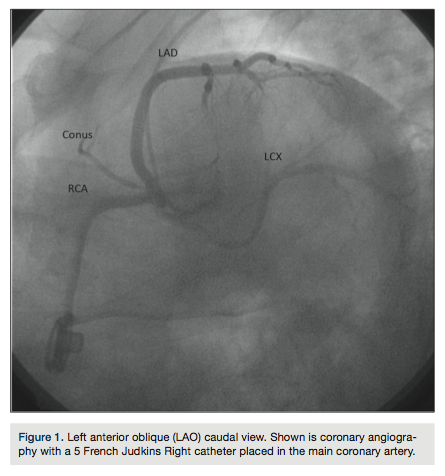 abnormal electrocardiogram (ECG) was referred for further evaluation. Review of his ECG showed 2-mm ST elevation in leads V2 and V3, and 1-mm ST elevation in leads V4-V6. Transthoracic echocardiography showed only mild global left ventricular (LV) hypokinesis. Subsequent coronary angiography (Figure 1) revealed a single common coronary artery (SCA) arising from the right coronary cusp with no significant obstructive disease and a dominant right coronary artery (RCA) that wrapped around the left ventricular apex. Computed tomography coronary angiography (Figures 2-5) confirmed the right coronary cusp origin. The left anterior
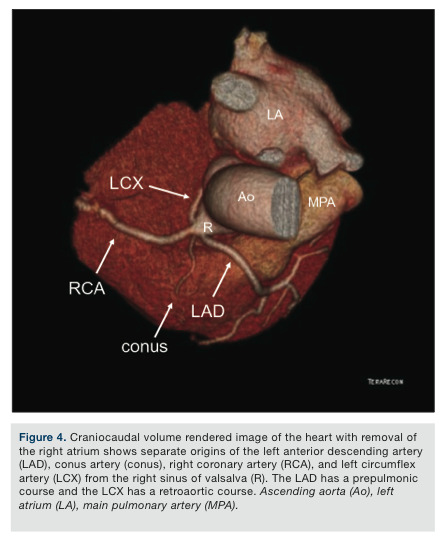
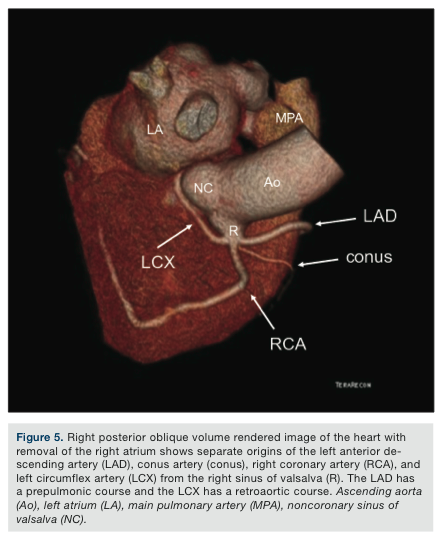
abnormal electrocardiogram (ECG) was referred for further evaluation. Review of his ECG showed 2-mm ST elevation in leads V2 and V3, and 1-mm ST elevation in leads V4-V6. Transthoracic echocardiography showed only mild global left ventricular (LV) hypokinesis. Subsequent coronary angiography (Figure 1) revealed a single common coronary artery (SCA) arising from the right coronary cusp with no significant obstructive disease and a dominant right coronary artery (RCA) that wrapped around the left ventricular apex. Computed tomography coronary angiography (Figures 2-5) confirmed the right coronary cusp origin. The left anterior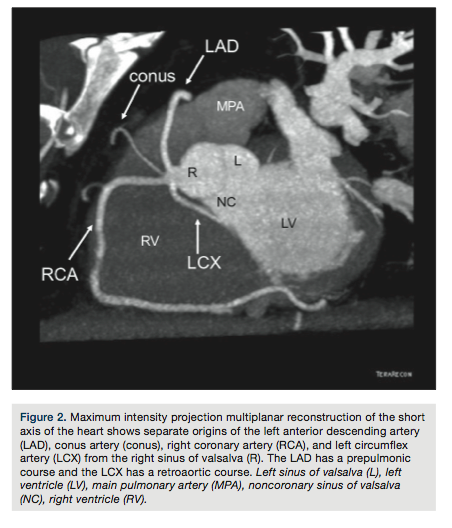 descending coronary artery (LAD) was shown to course anterior to the pulmonary artery. The left circumflex and RCA followed a relatively normal course; the RCA was confirmed to be large and to cover an extensive part of the inferior and apical left ventricular walls.
descending coronary artery (LAD) was shown to course anterior to the pulmonary artery. The left circumflex and RCA followed a relatively normal course; the RCA was confirmed to be large and to cover an extensive part of the inferior and apical left ventricular walls.
SCA arising from the right sinus of valsalva is a very rare anomaly, accounting for 0.3%1 of all coronary anomalies and just 0.026%-0.066%2,3 of the general population. This anomaly is labeled R-III (A) by the modified1 Lipton classification system.3 Although associated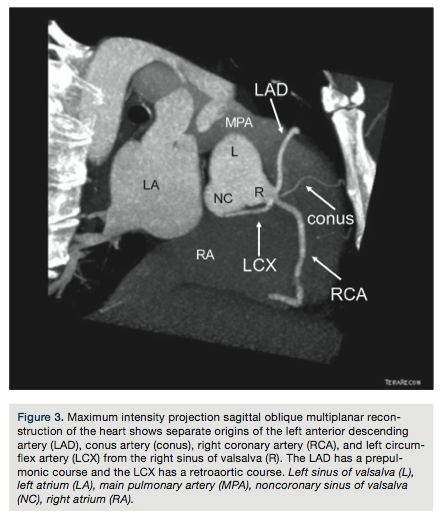 with exertional chest pain, this anomaly does not have an intra-arterial course and therefore is thought to not be associated with compression between the great arteries, myocardial infarction, or sudden death.4
with exertional chest pain, this anomaly does not have an intra-arterial course and therefore is thought to not be associated with compression between the great arteries, myocardial infarction, or sudden death.4
The authors can be contacted via Ihab Alomari, MD, at ialomari@salud.unm.edu.
References
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing
 coronary arteriography. Cathet Cardiovascular Diagn. 1990; 21: 28–40.
coronary arteriography. Cathet Cardiovascular Diagn. 1990; 21: 28–40. - Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956; 14: 800–805.
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979; 130: 39–47.
- Barth CW, Roberts WC. Left main coronary artery originating from the right sinus of valsalva and coursing between the aorta and pulmonary trunk. J Am Coll Cardiol. 1986;
 7(2): 366-373. doi: 10.1016/S0735-1097(86)80507-1.
7(2): 366-373. doi: 10.1016/S0735-1097(86)80507-1.