


Interfacing the GE Mac-Lab Patient Data Acquisition System and the VA Hospital Information System: A Case Study
The San Francisco Veterans Affairs (VA) cardiac cath lab has now been using an automated, all-electronic method of sending procedure reports generated in our GE Medical Systems Mac-Lab to the patient record for over a year and a half. Recently, we have had several inquiries regarding how the San Francisco VA cardiac cath lab’s Mac-Lab to VistA reporting system works and how to implement the process at other VA medical centers. (Veterans Health Information Systems and Technology Architecture (VistA) is the name for the Veterans Health Administration health care information technology system.) I decided to document the process to make it easier for others to get started with a similar system, and to clarify its advantages and disadvantages.
Before
Originally, to document cases we had a Marquette system that recorded pressures and rhythms on a 10 inch-wide strip recorder. At the end of the case, we had a ½ to 1-inch thick stack of strip chart that was sent to medical records, never to be seen again. For recording medications and sedation, we had a four-page VA form that was mandated by anesthesia and used in all areas of the hospital that needed conscious sedation. After a couple of upgrades and Marquette being bought out by GE, we moved into a new lab and used the first all-digital Mac-Lab. By that time, I had been in the cath lab as full-time staff for about five years. The entire hospital was becoming more digitized as well; images and scanned documents could now be saved in the patient’s Computerized Patient Record System (CPRS) via a link to the VistA Imaging server, and viewed on any workstation that had access to CPRS. We were still using a version of the same four-page conscious sedation form to chart medications and vital signs, IV fluids, and anything else. We kept cramming more and more information on it, and of course, some nurses’ records were more legible than others, but now the end result was sent to medical records to be scanned into VistA Imaging.
In 2007, a new cath lab manager was hired, and there was again talk of getting rid of all the paper. Someone mentioned that there was a way to print out a case report on a PDF file and send it to VistA Imaging. Unfortunately, over the next two years, the new manager became preoccupied with other matters and this issue got put on the back burner. The Mac-Lab to VistA idea never went anywhere. Meanwhile, the nurses were tired of filling out the four-page sedation form for more and more cases, writing a separate note in CPRS, and filling out a pre and post briefing checklist, not to mention having to focus on legibility, completeness, and changing requirement issues. At some point, I learned that the PDF report to VistA system was in use at the Edward Hines, Jr. VA Hospital in Chicago.
Using class training that came with the Mac-Lab upgrade, I went to the GE class on advanced clinical reports, thinking that they would discuss the report sent to VistA. The Mac-Lab has an Oracle database built into it that can be queried using Crystal Reports software to produce just about any kind of report you want. About halfway through the class, I realized that they were teaching us about a different report, but I did learn a great deal about the way data was handled in the Mac-Lab. The Mac-Lab has two different reporting systems: administrative and case, and it is the case reports that can be sent to VistA.
The process and project
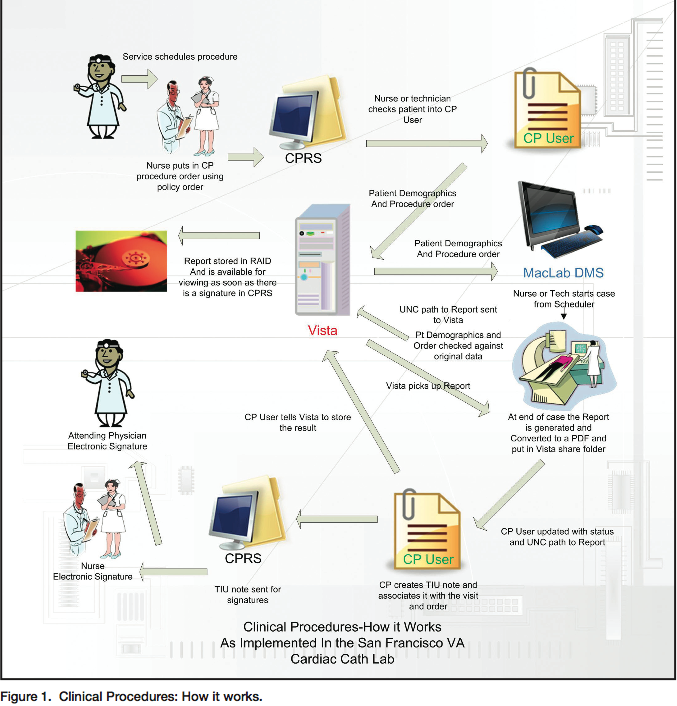 I began contacting the people at Hines Hospital in Chicago at the end of 2009/start of 2010, and at the same time, set about creating a set of custom forms in the Mac-Lab that would meet moderate sedation, medical center documentation, and nursing requirements. On March 10, 2010, the cath lab physicians, clinical informatics personnel, and nursing management met to review the idea. I learned that I had to use a CPRS module known as Clinical Procedures to link the Mac-Lab to VistA, and that there had already been some attempts to use it in other departments with varying degrees of success and one outright failure. After some discussions with GE and Hines, I was told that only the full bidirectional implementation would do what we wanted. It was all or nothing. Due to previous experiences with Clinical Procedures, some of the clinical application coordinators were skeptical of the idea, but thanks to Katie Miskovic, RT, and Karen Mclean, RN, a cath lab nurse manager at Hines, a “users manual” was assembled with enough information for the San Francisco VA IT and clinical applications people to start implementing the process. A primary requirement for implementing the Mac to VistA report is that the Clinical Procedures bidirectional interface must be used1 (Figure 1).
I began contacting the people at Hines Hospital in Chicago at the end of 2009/start of 2010, and at the same time, set about creating a set of custom forms in the Mac-Lab that would meet moderate sedation, medical center documentation, and nursing requirements. On March 10, 2010, the cath lab physicians, clinical informatics personnel, and nursing management met to review the idea. I learned that I had to use a CPRS module known as Clinical Procedures to link the Mac-Lab to VistA, and that there had already been some attempts to use it in other departments with varying degrees of success and one outright failure. After some discussions with GE and Hines, I was told that only the full bidirectional implementation would do what we wanted. It was all or nothing. Due to previous experiences with Clinical Procedures, some of the clinical application coordinators were skeptical of the idea, but thanks to Katie Miskovic, RT, and Karen Mclean, RN, a cath lab nurse manager at Hines, a “users manual” was assembled with enough information for the San Francisco VA IT and clinical applications people to start implementing the process. A primary requirement for implementing the Mac to VistA report is that the Clinical Procedures bidirectional interface must be used1 (Figure 1).
The first hurdle was getting GE remote access to our servers. Due to the rigorous information security, our biomedical and IT departments were having a difficult time obtaining remote access for GE, but finally, by September 22, 2010, remote connectivity was established. A test version of Clinical Procedures User was installed on my desktop and our biomed department set up the network connections between VistA and the Mac-Lab digital media server (DMS). The GE technician installed the necessary software and initial configurations. To initiate the process, an order and consult are needed, and the nursing policy committee approved a policy order allowing me to enter these. After testing and setup by biomed and the clinical application coordinators assigned to this project, a successful send of a test patient report to VistA occurred on December 9, 2010.
Since then, we have added the electrophysiology (EP) module to our orders and on this system, are now also doing ablations, diagnostic EP, and device implants that do not require anesthesia. There have been some rough patches where the multiple connections required meant a breakdown and some problems with the data acquisition during the cases also have prevented a report from going to VistA. Since we now meet all conscious sedation requirements, pre- and post- briefing, and time out requirements using this report, all problems had to be tracked down and fixes found as fast as possible, but we now have a greater than 90% success rate with the automatic system. Any problem reports are fixed in routine follow-ups by a variety of means. One cath lab-specific problem was identified with the fractional flow reserve (FFR) module that prevented conversion of the report to a PDF. A manual fix has been used, but hopefully GE will change this in a future upgrade.
System components, and who did what
Physically, the system consists of acquisition workstations (two in our case), an INW network server, and a cardiovascular information systems (CVIS) patient data server. This runs the GE software that is the Mac-Lab/CardioLab acquisition system. The VistA Imaging application accesses a shared folder on the CVIS Admin Server. The HL7 Orders interface from VistA CP connects to the CVIS HL7 Orders interface. On the hospital network, there is the CP User software that runs on the regular hospital PC workstations, where the nurse checks the patient in for the procedure. There is CP Gateway software that runs on a server in the hospital network that connects the report to the patient’s chart using two interfaces: a CP MUMPS device interface and a package interface. Lastly, there are the VistA Imaging servers that contain all of the electronically generated documents for the patient’s medical record.
The GE field service technician installed all the software components. Remote configuration and troubleshooting by the GE interface specialist was coordinated by the GE project manager. The GE interface specialist has been a primary resource for handling errors and how things work in general. The Clinical Procedures (CP) software was installed by the VistA programmers and our IT department. For details of the Clinical Procedures/VistA interface software, see the Clinical Procedures website.2 Basically, Clinical Procedures is an electronic paper clip that associates the study information with patient information, along with the locations on the network where it is stored.
Network configuration was done by the biomed/IT departments. Medical informatics personnel gave overall guidance and the clinical applications coordinator was constantly involved in configuring the software to our specific demands.
How it works, and the positives and negatives
 It should be noted that the Clinical Procedures software was designed for a standard medical model of a physician ordering a consult for some kind of instrument-acquired data performed by a technologist under the supervision of an attending physician (Figure 1). The technologist is supposed to then complete the study and send the report to VistA. The Clinical Procedures system alerts the attending and he signs a note automatically created by Clinical Procedures. The ordering provider is then alerted that the result is ready to view. The vehicle for doing this is the consult.
It should be noted that the Clinical Procedures software was designed for a standard medical model of a physician ordering a consult for some kind of instrument-acquired data performed by a technologist under the supervision of an attending physician (Figure 1). The technologist is supposed to then complete the study and send the report to VistA. The Clinical Procedures system alerts the attending and he signs a note automatically created by Clinical Procedures. The ordering provider is then alerted that the result is ready to view. The vehicle for doing this is the consult.
 In our cath lab, the process has been adapted as follows. At the end of the case, the nurse verifies that all required information is in the forms, generates a report and closes the case. One to five minutes later, a report shows up in VistA Imaging that can be viewed from any workstation in the hospital. At the end of the day, designated nurses complete the consult associated with the report and send it to the attending physician for sign off.
In our cath lab, the process has been adapted as follows. At the end of the case, the nurse verifies that all required information is in the forms, generates a report and closes the case. One to five minutes later, a report shows up in VistA Imaging that can be viewed from any workstation in the hospital. At the end of the day, designated nurses complete the consult associated with the report and send it to the attending physician for sign off.
 It is gratifying to see the time saved in nursing documentation and the enthusiastic response from the staff. It took a team effort, which is ongoing, but the results have been worth it: no paper to scan, and no forms to fill out or misplace. I did a retrospective survey of three months worth of cases from the previous year and found that the average time for medical records to scan the paper into the patient chart was from three to seven days. In one case, it was five weeks and there were several cases where it took two to three weeks. There were about three cases totally missing and two cases where the scanning was bad enough that many parts of the record were not legible. Overall, despite the difficulties in setting up a new system, it is already beating the old one in completeness. The advantages of the electronic system are multiple:
It is gratifying to see the time saved in nursing documentation and the enthusiastic response from the staff. It took a team effort, which is ongoing, but the results have been worth it: no paper to scan, and no forms to fill out or misplace. I did a retrospective survey of three months worth of cases from the previous year and found that the average time for medical records to scan the paper into the patient chart was from three to seven days. In one case, it was five weeks and there were several cases where it took two to three weeks. There were about three cases totally missing and two cases where the scanning was bad enough that many parts of the record were not legible. Overall, despite the difficulties in setting up a new system, it is already beating the old one in completeness. The advantages of the electronic system are multiple:
- Legibility: The old note was a four-page document with lots of handwriting by different people, with different charting styles.
- Reliability: The old note had to be filed by the nurse, transported to medical records by a clerk, and then scanned into the computer. A review of records indicates that some of the records have gone missing. Once that happens, the document cannot be recreated. In the Mac-Lab system, there will always be a PDF generated and stored at the end of the case. If the communication with VistA goes down, the cases can be reopened and closed, and the report will be retransmitted.
- Accountability/Availability: The old system kept the cath lab case documents inaccessible, except to cath lab staff. Any review of data required someone to come to the cath lab and open the case. Any review of case events that was not recorded on the forms therefore was not available. The VistA Imaging document is available about five minutes after a case is closed. A receiving unit, for example, would be able to check to see what medications were given and exactly when, if questions arise. Quality improvement can be more automated.
- Flexibility: New requirements can easily be added to reports. The paper document had become cluttered with added-on requirements that were not clear due to space restrictions.
- Attentiveness: Nurses are able to devote more attention to the cases as duplicate and tedious hand charting during the case is reduced.
- During STEMI call-in cases, there is no need to take up nurse time to create the conscious sedation form, or work around the process by reverse engineering the form afterwards.
- Overall flow is now more like other related procedures elsewhere in the hospital: order, consult and report; and in line with the trend to all-electronic record keeping.
- Accurate case identification is maintained because the order system populates the case demographics directly from the patient’s hospital chart, eliminating manual transcription errors.
- As an added bonus, the Siemens x-ray equipment has been fitted with an interface to allow the data on the digital media server (DMS) imported from the hospital information system to be used to identify the x-ray images, eliminating another potential transcription error.
- VA policy directs that patient records be electronic whenever possible.3
Unfortunately, the cath lab workflow is more dynamic and the requirements more complex than the system was originally designed for. It is more suited for routine echocardiograms, EKGs, scans, and minor interventional radiology procedures. The system had to be adapted to fit the needs of the cath lab, so some creativity and cooperation was required. It takes someone in the cath lab that knows the Mac-Lab well to constantly push for a system that works for the end users: the physicians, nurses, and technologists in the lab. In another unit that tried to implement Clinical Procedures, this type of champion was not present and the unit failed (but may now try again.) In the end, I think this is what made the difference between a failure and the success we have experienced so far. Anyone contemplating this type of project should identify one person early on and give them the time, resources, and administrative support necessary.
Although the overall results are good, there is a downside to the system in that on the hospital information side, the connection is made through four separate software packages to VistA, with many potential failure sites. Clinical Procedures User software has not been upgraded past version 1.1. Almost all the persistent failures in sending reports so far have been on the VistA side, where the interface, called Clinical Procedures Manager, runs and handles all services, using this module to send instrument data to VistA. There has been more maintenance and troubleshooting than initially planned. To make this work, we have needed one person possessing the necessary permissions, who knows how to manually correct errors and resend reports as needed. We have also developed a backup method that gets around Clinical Procedures by using the VistA Imaging Capture software. This is similar to the print and scan method, except there is no need to print out anything, just get the PDF off the server.
With time out documentation, conscious sedation, verbal orders issues, and hand off issues making documentation more complex, I think more and more labs will be interested in implementing an all-electronic reporting system. In addition, there is the Joint Commission requirement.4 Even though the physicians may use CART-CL or another system to document their findings immediately, it is not a complete record of the procedure itself, with all vital signs and events. Although it is possible to meet these requirements by printing out and scanning, this is a waste of time and paper, lacking many of the advantages enumerated above, and there is already a report in PDF form available.
Any VA lab that uses Mac-Lab is welcome to contact me at michael.jackson2@va.gov for the information needed to start their own Mac to VistA project. I would also be interested in the experiences of any lab that has implemented a similar system with other acquisition systems.
References
- “Mac-Lab/CardioLab + VistA Imaging B-directional Interface.” 3/15/2009. General Electric Company. Owner Greg White. Doc0583787 Rev no. 1.
- Clinical Procedures website. Available online at https://vista.med.va.gov/ClinicalSpecialties/clinproc/
- VA policy re electronic records. Department of Veterans Affairs Medical Center, San Francisco, CA. Medical Center Memorandum 136-31, Standards for Medical Records, Section 4. Procedures, a) Medical Records Content/Documentation:, Subpart (2).
- Joint Commission standard RC.02.01.03 #5 states, “an operative or other high-risk procedure report is written or dictated upon completion of the operative or other high risk procedure and before the patient is transferred to the next level of care.”
