


Improvement of Transfer Times Utilizing Systemization Development Leads to the First Mission: Lifeline STEMI Receiving Facility Accreditation in Ohio
 Summa Health System, headquartered in Akron, Ohio, is one of the largest integrated healthcare delivery systems in Ohio. Summa serves more than one million patients each year in comprehensive acute, critical, emergency, outpatient and long-term/home-care settings, and represents more than 2,000 licensed inpatient beds in our clinical settings. Within the 6-hospital system, there is one 24-hour primary percutaneous coronary intervention (PPCI) center located at Summa Akron City Hospital.
Summa Health System, headquartered in Akron, Ohio, is one of the largest integrated healthcare delivery systems in Ohio. Summa serves more than one million patients each year in comprehensive acute, critical, emergency, outpatient and long-term/home-care settings, and represents more than 2,000 licensed inpatient beds in our clinical settings. Within the 6-hospital system, there is one 24-hour primary percutaneous coronary intervention (PPCI) center located at Summa Akron City Hospital.
Summa Akron City Hospital identified poor transfer times for the ST-segment elevation myocardial infarction (STEMI) patient from outlying feeder hospitals to the PPCI center. An overall, very inclusive review revealed that one constant factor contributing to this delay was the lack of consistency in the policies and procedures across the system. Each facility was proceeding with the care and transfer of the STEMI patient following their own specific procedures, which can lead to oversight or even obvious omissions of care. Careful review of these inconsistencies led to the identification of the following objectives:
Objective 1: After reviewing variances in practices and policies, the hospital system will standardize and implement changes in the care of the STEMI patient prior to transfer from the outlying facilities.
Objective 2: After reviewing variances in practice and policies, the hospital system will utilize one Emergency Medical Service (EMS) provider to transport all STEMI patients from our outlying facilities.
Objective 3: After appropriate education and communication, the emergency department (ED) physicians will be empowered to activate the code STEMI from the outlying EDs before speaking with the interventional cardiologist on call.
Objective 4: Within 24 hours, a summarization of metrics and outcomes will be provided to all participants in the care of the transferred STEMI patient.
It was felt that the ability to meet these objectives would lead to consistency across the system and therefore improve patient outcomes.
Tacking the objectives
To meet the first objective, acute myocardial infarction case manager Anthony DeAngelis RN, BSN, CCRN, and chest pain coordinator Deborah Washington RN-BC, BSN, CCPC, performed on-site reviews at each of the outlying facilities. Practices, policies and procedures were reviewed. An agreement regarding standardization across the system was obtained at each facility. Practices, policies, and procedures were aligned as closely to Summa Akron City Hospital’s as possible. A system-wide STEMI protocol was created and implemented at all system facilities. The emergency physician group from Akron City Hospital also provides coverage at several of our other facilities. The standardized protocols within the system allow for more consistency and ease following the set protocol. Continuity across the system ensures the highest level of care for our patients.
The second objective was fulfilled by using one EMS provider for the care and transport of the STEMI patient. Using one EMS provider allowed for consistency with protocols, documentation, and facility awareness. A contract was secured with a local, private EMS company that committed to having a squad en route to the transferring facility within 8 minutes of receiving the STEMI transfer phone call. In order to facilitate a rapid transfer once EMS arrived, the outlying facilities were made aware of the documents the EMS crew would need and had them available upon EMS arrival. The hospital provided one of our group STEMI pagers to the dispatch office of the EMS provider, with the idea that it would facilitate and allow for a quicker EMS response. The dispatchers can send an ambulance toward the facility even before the official phone call is received from the sending facility requesting a squad for transport. The objective is to initiate early and then cancel or “stand down” the call if necessary.
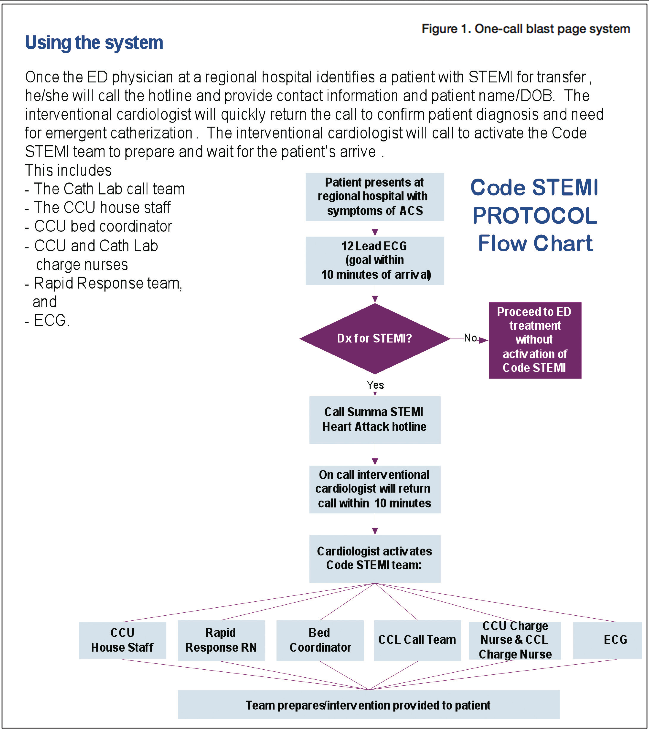 The third objective was met by providing education on a consistent method for activating the STEMI call. Prior to the ED physician being empowered to activate the code STEMI, the process required that the ED physician page the cardiologist, wait for the call back, consult with cardiologist, fax the electrocardiogram (ECG), and then the cardiologist would make the determination about whether the patient was a STEMI. An additional phone call was then made by the cardiologist to activate the code STEMI. Instead, a one-call process was put into place in which the transferring facility called the “STEMI Hotline” (Figure 1). This one call would send out a group or “burst” page that would then notify the STEMI cardiologist, cath lab call team, ECG staff, coronary care house staff and nursing staff, rapid response team, and bed coordinator. The entire team was mobilized at once, allowing for quicker arrival response times from the cath lab staff and cardiologist who may be responding from home. There was also an “auto accept” policy put into practice to ensure the ED physician would know that the cardiovascular medicine department would accept all STEMI patients.
The third objective was met by providing education on a consistent method for activating the STEMI call. Prior to the ED physician being empowered to activate the code STEMI, the process required that the ED physician page the cardiologist, wait for the call back, consult with cardiologist, fax the electrocardiogram (ECG), and then the cardiologist would make the determination about whether the patient was a STEMI. An additional phone call was then made by the cardiologist to activate the code STEMI. Instead, a one-call process was put into place in which the transferring facility called the “STEMI Hotline” (Figure 1). This one call would send out a group or “burst” page that would then notify the STEMI cardiologist, cath lab call team, ECG staff, coronary care house staff and nursing staff, rapid response team, and bed coordinator. The entire team was mobilized at once, allowing for quicker arrival response times from the cath lab staff and cardiologist who may be responding from home. There was also an “auto accept” policy put into practice to ensure the ED physician would know that the cardiovascular medicine department would accept all STEMI patients.
The fourth and final objective included a practice that allowed for a sense of inclusion, responsibility, and therefore, commitment to the process. A STEMI feedback form included staff that represented EMS/pre-hospital, the transferring facility, ED personnel, ECG staff, and cath lab staff that cared for the specific STEMI patient. A feedback template was created and used across the system to allow for review by all campuses. This immediate feedback provided a real-time review of processes done well and identified opportunities for improvement. Each area reviews the STEMI feedback forms and the appropriate departments follow up on any identified outliers. STEMI feedback forms are also discussed at the appropriate ED meetings, EMS reviews, cath lab meetings, ECG staff meetings, and other quality-focused venues. It provides for accountability from all participants, as well as recognition in a transparent forum. The level of accountability seems to increase with the idea of transparency, as does the pride in recognition for a job well done. We have found that the increased accountability and pride leads to a sense of ownership by all who provide care.
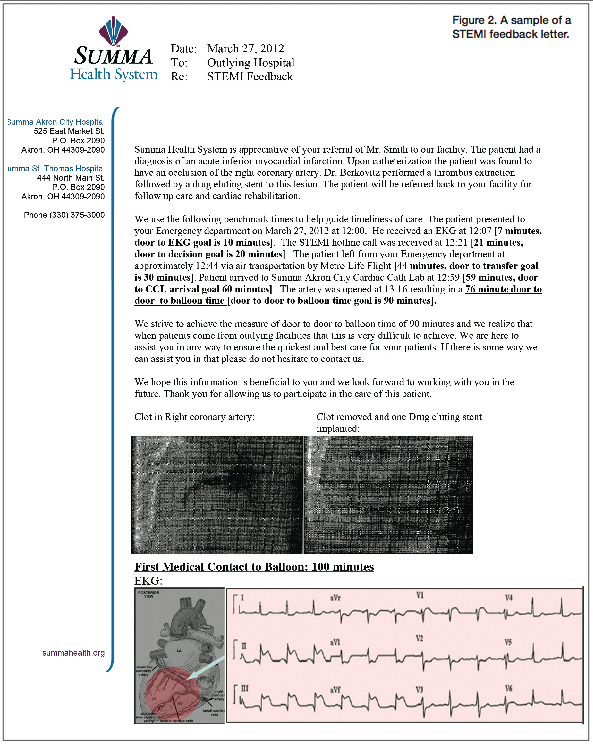 Figure 2 shows a sample of the feedback letter that is sent out to the participants of a STEMI patient. We provide case specifics, as well as the ECG and the pre and post cath lab pictures in the feedback letter. The images allow for a better understanding and further education for those who may not be aware of what the cath lab images look like before and after the culprit lesion is addressed. The ECG also allows the EMS providers the ability to connect what they have learned with the actual visual aspect of the anatomy and physiology of the STEMI process. We educate the EMS providers that the inferior changes on the ECG generally affect the right coronary artery, so they are better able to visualize the physical process when looking at the ECG. The benefits of sending this feedback letter out have been far-reaching and allow for improved care of the STEMI patient from the initiation of the 9-1-1 phone call.
Figure 2 shows a sample of the feedback letter that is sent out to the participants of a STEMI patient. We provide case specifics, as well as the ECG and the pre and post cath lab pictures in the feedback letter. The images allow for a better understanding and further education for those who may not be aware of what the cath lab images look like before and after the culprit lesion is addressed. The ECG also allows the EMS providers the ability to connect what they have learned with the actual visual aspect of the anatomy and physiology of the STEMI process. We educate the EMS providers that the inferior changes on the ECG generally affect the right coronary artery, so they are better able to visualize the physical process when looking at the ECG. The benefits of sending this feedback letter out have been far-reaching and allow for improved care of the STEMI patient from the initiation of the 9-1-1 phone call.
Results
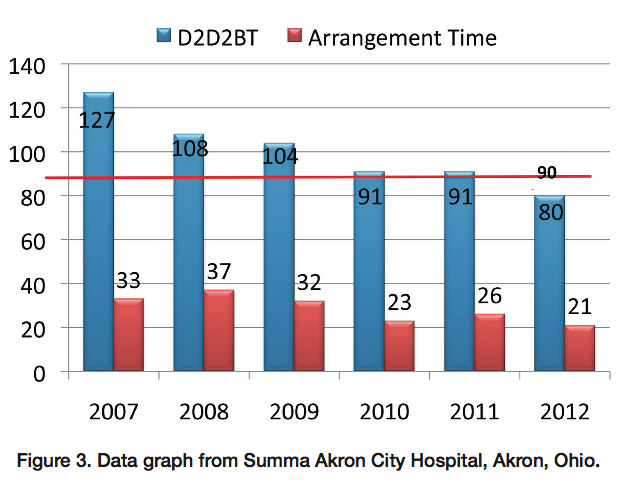 We are very pleased with the results of the implemented changes. We measure door-to-door-to-balloon (D2D2B) time, which is from the patient arrival at the outlying facility until the artery is opened at the STEMI receiving facility. The average transfer arrangement time is measured from when the code STEMI system is activated until the patient leaves the outlying transfer facility. Our results have shown that our hospital system has reduced both our D2D2B time and our average transfer arrangement time after initiating the process of STEMI transfer protocol standardization across our health system (Figure 3). Since 2007, we have demonstrated a decrease of 53 minutes in our D2D2B time. The current average D2D2B time at Summa Akron City Hospital is 80 minutes, 10 minutes less than the American College of Cardiology/American Heart Association (ACC/AHA)¹ guidelines of 90 minutes. Since implementing a one-call EMS transport system process, we have also achieved a decrease in transfer arrangement time by 12 minutes.
We are very pleased with the results of the implemented changes. We measure door-to-door-to-balloon (D2D2B) time, which is from the patient arrival at the outlying facility until the artery is opened at the STEMI receiving facility. The average transfer arrangement time is measured from when the code STEMI system is activated until the patient leaves the outlying transfer facility. Our results have shown that our hospital system has reduced both our D2D2B time and our average transfer arrangement time after initiating the process of STEMI transfer protocol standardization across our health system (Figure 3). Since 2007, we have demonstrated a decrease of 53 minutes in our D2D2B time. The current average D2D2B time at Summa Akron City Hospital is 80 minutes, 10 minutes less than the American College of Cardiology/American Heart Association (ACC/AHA)¹ guidelines of 90 minutes. Since implementing a one-call EMS transport system process, we have also achieved a decrease in transfer arrangement time by 12 minutes.
As a multi-campus health system, it was imperative that we provide the highest level of care to our STEMI patient at each facility. To facilitate quality care, we made changes throughout our system to empower all our ED physicians to activate the code STEMI before having to speak to anyone personally at the STEMI PPCI receiving center. This ensured the patient was mobilized as quickly as possible to decrease the D2D2B times. The identification of loopholes within our own campuses allowed us to systemize our policies and procedures in order to decrease any variances, and therefore decrease and prevent errors. All healthcare providers appreciated the timely feedback, whether positive or negative. We determined that the more immediate the feedback, the more value it provided to each of the team members. We were able to provide feedback to all entities involved in the care of the STEMI transfer, including EMS, transferring facility staff, ECG staff, PPCI center ED staff, and cardiac cath lab staff. This allowed for rapid identification of when predetermined targets were not being met, and rapid review and correction of identified problems. The process of securing one EMS transport company for our STEMI transfer patients allowed for more consistency across our facilities. The same paperwork, protocols, and procedures allowed for less time spent in the ED before transfer occurs. This decreased our transfer arrangement time and our overall D2D2B times. Instituting all of these changes allowed us to provide the highest level of care for the STEMI patient. We were able to reduce times in specific areas, which led to overall reductions in our D2D2B time.
Commitment and accreditations
 Summa Akron City Hospital obtained our Chest Pain Center with Percutaneous Coronary Intervention Accreditation in November 2010. These additional significant results achieved with the systemization of protocols have allowed us to obtain the FIRST and only Mission: Lifeline STEMI Receiving Facility Accreditation in the state of Ohio! (Figure 4) At the time of this writing, there are only 11 facilities in the United States to have achieved this honored accreditation. We are very proud to be both an Accredited Chest Pain Center with Percutaneous Coronary Intervention and Mission: Lifeline STEMI Receiving Accredited Center. The mission of Summa Health System is to provide the highest quality, compassionate care to our patients and to contribute to a healthier community. We believe that these results have shown our commitment to our mission. Most importantly, these results have allowed us to save lives in our community.
Summa Akron City Hospital obtained our Chest Pain Center with Percutaneous Coronary Intervention Accreditation in November 2010. These additional significant results achieved with the systemization of protocols have allowed us to obtain the FIRST and only Mission: Lifeline STEMI Receiving Facility Accreditation in the state of Ohio! (Figure 4) At the time of this writing, there are only 11 facilities in the United States to have achieved this honored accreditation. We are very proud to be both an Accredited Chest Pain Center with Percutaneous Coronary Intervention and Mission: Lifeline STEMI Receiving Accredited Center. The mission of Summa Health System is to provide the highest quality, compassionate care to our patients and to contribute to a healthier community. We believe that these results have shown our commitment to our mission. Most importantly, these results have allowed us to save lives in our community.
Acknowledgements. Many of these objectives were met with the help of our acute myocardial infarction case manager, Anthony DeAngelis RN, BSN, CCRN. We would like to thank Anthony for his hard work and dedication in the care of the STEMI patient.
Deborah Washington can be contacted at washindl@summahealth.org.
Reference
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol 2004; 44:e1-e211.
