


Impella 2.5-Supported Revascularization in a Patient with Normal EF and a Large Amount of Myocardial Jeopardy
Introduction
The advent of left ventricular assist devices has allowed the interventional cardiology community to perform complex coronary interventional procedures in a safe, effective manner. Initial iterations of left ventricular assist devices demanded a modest amount of technical abilities, and therefore adoption of this technology was not very widespread. The advent of the Impella 2.5 circulatory support device (Abiomed, Inc., Danvers, Mass.) has enabled interventional cardiologists to perform more complex coronary interventions.1
Recently, the PROTECT II trial demonstrated that revascularization of these complex patients is appropriate and improves their NYHA classification. Fifty-eight percent of patients in class III/IV were able to move their classification of heart failure down by one or more levels, thus improving their quality of life. The PROTECT II trial data, presented at the TCT 2011 conference in San Francisco, also demonstrated that more complete revascularization with Impella 2.5 leads to better outcomes, with a 34% reduction in major adverse events (MAE) over the intra-aortic balloon pump (IABP) arm. When PCI was performed in patients supported by Impella 2.5 and extensive revascularization was done, major adverse cardiac and cerebral events (MACCE) rates were 47% lower than the patients supported by an IABP.2 It is believed that the reduction in MAE is due to the ability of the interventional cardiologists to perform more thorough revascularization with the support provided by the Impella device.
Traditionally, a high risk percutaneous coronary intervention (PCI) is considered to be an intervention in which a patient has either left main disease or multivessel disease, suppressed LV ejection fraction, or a combination of the two. Recent data suggests that individuals with normal LV function who have lesions in coronary anatomy that place large territories of myocardium in jeopardy are also considered high risk.3 This case demonstrates such a scenario.
Case
 This patient is a 77-year-old male with a history of ulcerative colitis, severe chronic obstructive pulmonary disease (COPD), bladder cancer, and surgically removed pheochromocytoma, who presented to the hospital with angina and progressive dyspnea. Stress testing revealed a very large, reversible inferolateral defect. Cardiac catheterization revealed a high-grade stenosis in the ostium of a dominant circumflex (Cx) coronary artery and a left ventricular ejection fraction (LVEF) of about 45%. Because of the location of the lesion, medical therapy was recommended. Post procedurally, the patient developed an acute embolic thalamic stroke. He recovered from his stroke and within a few weeks was admitted to the hospital again with identical symptoms, while on optimal medical therapy. Given his recent stroke and significant COPD, surgical revascularization was declined.
This patient is a 77-year-old male with a history of ulcerative colitis, severe chronic obstructive pulmonary disease (COPD), bladder cancer, and surgically removed pheochromocytoma, who presented to the hospital with angina and progressive dyspnea. Stress testing revealed a very large, reversible inferolateral defect. Cardiac catheterization revealed a high-grade stenosis in the ostium of a dominant circumflex (Cx) coronary artery and a left ventricular ejection fraction (LVEF) of about 45%. Because of the location of the lesion, medical therapy was recommended. Post procedurally, the patient developed an acute embolic thalamic stroke. He recovered from his stroke and within a few weeks was admitted to the hospital again with identical symptoms, while on optimal medical therapy. Given his recent stroke and significant COPD, surgical revascularization was declined.
 In order to adequately cover the ostium of his Cx, we had to ensure that a small portion of the deployed stent would have to protrude into the distal left main. To properly position the stent, and to avoid plaque shifting into the left main and the left anterior descending (LAD) coronary artery, we chose to employ a modification of the balloon backstop technique described in the past.4 Dual balloon inflation with one balloon inflated from left main into the LAD and the treating balloon inflated in the ostial Cx would create a large area of global ischemia, especially given the left dominant nature of the patient’s coronary anatomy. In order to effectively position both balloons without having to hastily perform the procedure, we chose to support the intervention with the Impella 2.5 circulatory support device.
In order to adequately cover the ostium of his Cx, we had to ensure that a small portion of the deployed stent would have to protrude into the distal left main. To properly position the stent, and to avoid plaque shifting into the left main and the left anterior descending (LAD) coronary artery, we chose to employ a modification of the balloon backstop technique described in the past.4 Dual balloon inflation with one balloon inflated from left main into the LAD and the treating balloon inflated in the ostial Cx would create a large area of global ischemia, especially given the left dominant nature of the patient’s coronary anatomy. In order to effectively position both balloons without having to hastily perform the procedure, we chose to support the intervention with the Impella 2.5 circulatory support device.
 A 13 French Peel-Away sheath (Cook Medical, Bloomington, In.) was positioned in the left common femoral artery, and the sheath was secured using two Proglide suture-mediated closure devices (Abbott Vascular, Redwood City, Ca.), utilizing the Preclose technique.5 An 8 French sheath was placed in the right common femoral artery. The Impella 2.5 circulatory support device was inserted through the 13 French sheath into the left ventricle, and adequate flow of about 2 L/min was achieved at a support level of P6. Through the 8 French sheath,
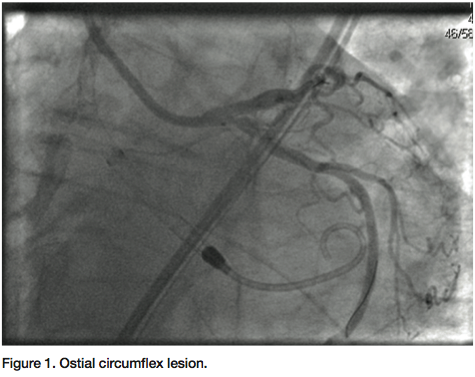
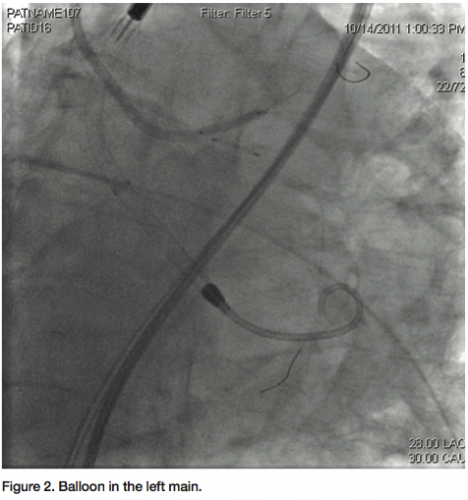
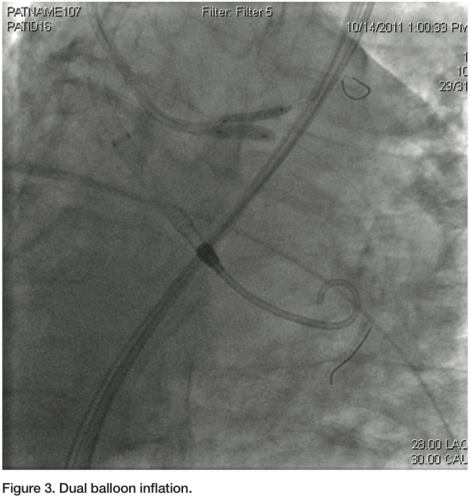
A 13 French Peel-Away sheath (Cook Medical, Bloomington, In.) was positioned in the left common femoral artery, and the sheath was secured using two Proglide suture-mediated closure devices (Abbott Vascular, Redwood City, Ca.), utilizing the Preclose technique.5 An 8 French sheath was placed in the right common femoral artery. The Impella 2.5 circulatory support device was inserted through the 13 French sheath into the left ventricle, and adequate flow of about 2 L/min was achieved at a support level of P6. Through the 8 French sheath,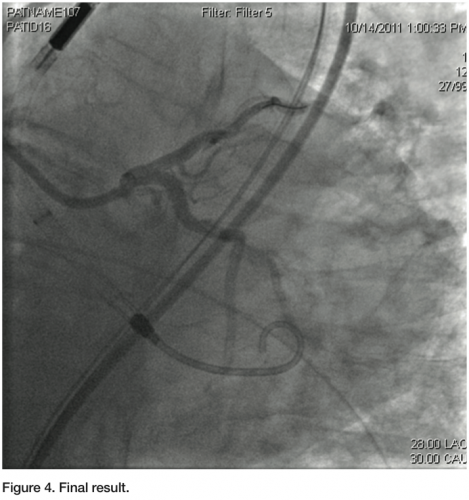 a Judkins left 3.5 guiding catheter was used to engage the left main. Two 0.014” angioplasty wires were introduced; one into the LAD, and one into the distal Cx. A 3.0 x 12 mm balloon was placed in the ostium of the Cx, and a diagnostic angiogram was obtained (Figure 1). Subsequently, a 2.5 mm balloon was placed from the left main into the LAD. A 3.5 x 8 mm bare-metal stent was placed in the proximal Cx. The 2.5 mm balloon was inflated to 10 atmospheres, protecting the left main and proximal LAD from plaque shifting during deployment of the Cx stent (Figure 2). The stent in the Cx was then withdrawn until it indented the left main balloon. The balloon in the left main was inflated for nearly a minute during this process, and the patient was completely asymptomatic. Systolic blood pressure did drop from about 130 mmHg to about 90 mmHg, but diastolic pressure was maintained due to support from the Impella 2.5 circulatory support device. Both balloons were then simultaneously inflated for about 25 seconds (Figure 3). The patient transiently developed global ST elevation and systolic hypotension, but remained asymptomatic. After both balloons were deflated, final images revealed excellent coverage of the ostial Cx lesion, with no significant compromise of the left main and LAD. Intravascular ultrasound (IVUS) analysis after stent deployment revealed a cross sectional area of 6.3 mm2 in the ostium of the LAD, with excellent visualization of the Cx stent in the ostium. At the conclusion of the procedure, the Impella 2.5 circulatory device was weaned off in the cath lab, and the 13 French sheath was removed, with the pre-placed sutures securing hemostasis. The right femoral sheath was also secured using a single Perclose Proglide device. The patient was uneventfully discharged home the following morning.
a Judkins left 3.5 guiding catheter was used to engage the left main. Two 0.014” angioplasty wires were introduced; one into the LAD, and one into the distal Cx. A 3.0 x 12 mm balloon was placed in the ostium of the Cx, and a diagnostic angiogram was obtained (Figure 1). Subsequently, a 2.5 mm balloon was placed from the left main into the LAD. A 3.5 x 8 mm bare-metal stent was placed in the proximal Cx. The 2.5 mm balloon was inflated to 10 atmospheres, protecting the left main and proximal LAD from plaque shifting during deployment of the Cx stent (Figure 2). The stent in the Cx was then withdrawn until it indented the left main balloon. The balloon in the left main was inflated for nearly a minute during this process, and the patient was completely asymptomatic. Systolic blood pressure did drop from about 130 mmHg to about 90 mmHg, but diastolic pressure was maintained due to support from the Impella 2.5 circulatory support device. Both balloons were then simultaneously inflated for about 25 seconds (Figure 3). The patient transiently developed global ST elevation and systolic hypotension, but remained asymptomatic. After both balloons were deflated, final images revealed excellent coverage of the ostial Cx lesion, with no significant compromise of the left main and LAD. Intravascular ultrasound (IVUS) analysis after stent deployment revealed a cross sectional area of 6.3 mm2 in the ostium of the LAD, with excellent visualization of the Cx stent in the ostium. At the conclusion of the procedure, the Impella 2.5 circulatory device was weaned off in the cath lab, and the 13 French sheath was removed, with the pre-placed sutures securing hemostasis. The right femoral sheath was also secured using a single Perclose Proglide device. The patient was uneventfully discharged home the following morning.
Discussion
Treatment of high risk, complex coronary lesions has become feasible to perform in a safe manner with the use of percutaneous ventricular assist devices. Traditional thinking has taught us that high-risk patients benefiting from percutaneous assist devices include those with suppressed LVEF, multivessel/left main disease, or a combination of the two.6 Complete revascularization, performed without the pressure of having to operate in a hasty fashion, has clearly shown to reduce the incidence of subsequent clinical events, as evidenced by the PROTECT II trial.2 Patient subsets who may not be considered high risk due to the absence of a low LV ejection fraction or multivessel disease may still pose a high risk for hemodynamic compromise due to the amount of myocardium potentially in jeopardy when performing percutaneous intervention. The case described herein is an excellent example of a patient who had a reasonable LVEF and single vessel disease, but who was felt to be high risk. Performing revascularization in a manner allowing for the precise positioning of a stent at a critical location meant putting myocardium in potential jeopardy. The patient’s hemodynamic parameters during dual balloon inflation confirmed the hemodynamic compromise to which he was subject, but it was tolerated without any untoward effects, due to support from the Impella 2.5 circulatory assist device. It is possible future studies may show clinical benefit in this patient subset. Coupled with the ease of use of the Impella 2.5 circulatory device, indications for use of circulatory support devices in the setting of percutaneous coronary interventions may expand accordingly.
The authors can be contacted via Dr. Umakanthan at: bumakanthan@yahoo.com
Disclosure: Dr. Umakanthan reports he is a consultant to Abiomed. Dr. Alasnag report no conflicts of interest regarding the content herein.
References
- Henriques JP, Remmelink M, Baan J Jr., et al. Safety and feasibility of elective high-risk percutaneous coronary procedures with left ventricular support of the Impella Recover LP 2.5. Am J Cardiol 2006;97:990-992.
- O’Neill W. PROTECT II: A prospective multicenter randomized clinical trial of intra-aortic balloon pump vs Impella for hemodynamic support during high-risk PCI. Presented at: ACC.11. American College of Cardiology Annual Scientific Session; 2011 April 2-5; New Orleans, Louisiana.
- Perera D, Stables R, Booth J, Thomas M, Redwood S. The balloon pump-assisted coronary intervention study (BCIS-1). Am Heart J 2009 Dec; 158(6): 910-916.
- Colombo A, Spanos V. Commentary: a new technique for coronary bifurcations: good news! J Invas Cardiol 2003;15(4): 184-185.
- Lee, WA. Access for TEVAR. The Preclose technique and the Proglide device offer safe and effective percutaneous access for thoracic endovascular aortic repair. Endovascular Today 2008 Sept: 48-55.
- O’Neill W. USPELLA: U.S. multicenter registry of Impella 2.5 patients evaluating the safety and feasibility of left ventricular support with the Impella 2.5 during high-risk percutaneous coronary intervention (PCI) and treatment of acute myocardial infarction (AMI). Transcatheter Cardiovascular Therapeutics Annual Scientific Session; 2010 September 21-25; Washington, D.C.
