


Hyperdominant Left Anterior Descending Artery Continuing as Posterior Descending Artery: A Rare Coronary Artery Anomaly
Abstract: The posterior descending artery usually arises from either the right coronary artery or the circumflex artery. Here we report an unusual case of the left anterior descending artery continuing as the posterior descending artery beyond the crux in the presence of diminutive right coronary artery.
Key words: hyperdominant left anterior descending artery, posterior descending artery.
Case presentation
A 66-year-old man was admitted to our hospital with chest pain, diaphoresis and dyspnea of five hours duration. At admission, his pulse rate was 104 per minute and regular, while blood pressure was 80/50 mm Hg. On auscultation, an S4 was present. Rales were present over the lower one third of both lungs. Electrocardiography showed sinus tachycardia and ST elevations in leads V1-V4, II, III and aVF, suggestive of anterior and inferior wall myocardial infarction.
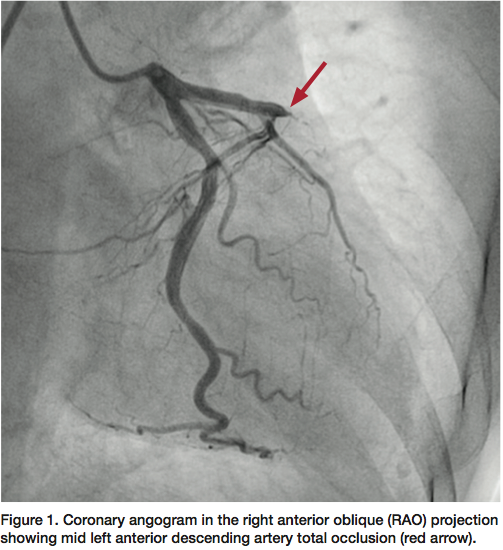 The patient was shifted immediately to the catheterization laboratory after informed consent was obtained for primary percutaneous intervention. Coronary angiography revealed that the left main coronary artery was normal and gave off the large left anterior descending (LAD) and left circumflex (LCX) arteries. The LCX was a non-dominant artery and free of disease. The LAD continued in the anterior interventricular groove with 100% occlusion after the septal branch (Figure 1). The right coronary artery was a nondominant, diminutive vessel arising from the right coronary sinus, ended in the right anterior atrioventricular groove, and was free of disease (Figure 2).
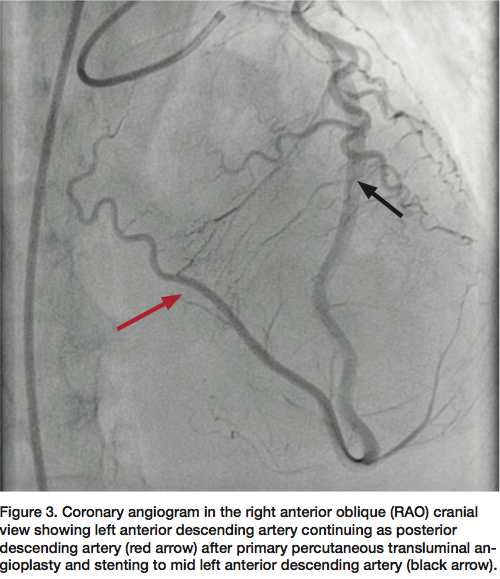
The patient was shifted immediately to the catheterization laboratory after informed consent was obtained for primary percutaneous intervention. Coronary angiography revealed that the left main coronary artery was normal and gave off the large left anterior descending (LAD) and left circumflex (LCX) arteries. The LCX was a non-dominant artery and free of disease. The LAD continued in the anterior interventricular groove with 100% occlusion after the septal branch (Figure 1). The right coronary artery was a nondominant, diminutive vessel arising from the right coronary sinus, ended in the right anterior atrioventricular groove, and was free of disease (Figure 2).  The patient underwent successful primary angioplasty and stenting to the mid LAD. Post procedure selective coronary angiogram of left coronary artery showed thrombolysis in myocardial infarction III (TIMI-III) flow in the LAD which continued as the posterior descending artery (PDA) (Figure 3). Post procedure, the patient was stable and discharged after five days from the hospital.
The patient underwent successful primary angioplasty and stenting to the mid LAD. Post procedure selective coronary angiogram of left coronary artery showed thrombolysis in myocardial infarction III (TIMI-III) flow in the LAD which continued as the posterior descending artery (PDA) (Figure 3). Post procedure, the patient was stable and discharged after five days from the hospital.
Discussion
 Coronary artery anomalies are usually discovered incidentally and have an incidence of 0.2-1.2% in the general population.1 Some of these anomalies are hemodynamically significant and are associated with adverse outcome. Banchi first described that there is considerable variation in the blood supply to the inferior and posterior wall of heart.2 Later, Schlesinger proposed the concept of coronary dominance.3 The term ‘right dominant circulation’ (85% of patients) refers to a pattern in which the right coronary artery (RCA) will give rise to the PDA, posterolateral branches and the atrioventricular (AV) nodal artery. The term ‘left dominant circulation’ (8% of patients) refers to when the LCX gives origin to these vessels. The term ‘co-dominance’ (7% of patients) refers to when the PDA arises from the RCA and the posterolateral branches from the LCX.4 Phillips et al described anomalous origin of the PDA from the vascular ring formed between the RCA and LCX.5 Ilia et al reported anomalous origin of the PDA from the obtuse marginal artery.6 Errichtti et al reported anamolous origin of the PDA from the first septal perforator.7 Levin and Baltaxe observed a double PDA in 6% and early origin of PDA in 5% of patients.8
Coronary artery anomalies are usually discovered incidentally and have an incidence of 0.2-1.2% in the general population.1 Some of these anomalies are hemodynamically significant and are associated with adverse outcome. Banchi first described that there is considerable variation in the blood supply to the inferior and posterior wall of heart.2 Later, Schlesinger proposed the concept of coronary dominance.3 The term ‘right dominant circulation’ (85% of patients) refers to a pattern in which the right coronary artery (RCA) will give rise to the PDA, posterolateral branches and the atrioventricular (AV) nodal artery. The term ‘left dominant circulation’ (8% of patients) refers to when the LCX gives origin to these vessels. The term ‘co-dominance’ (7% of patients) refers to when the PDA arises from the RCA and the posterolateral branches from the LCX.4 Phillips et al described anomalous origin of the PDA from the vascular ring formed between the RCA and LCX.5 Ilia et al reported anomalous origin of the PDA from the obtuse marginal artery.6 Errichtti et al reported anamolous origin of the PDA from the first septal perforator.7 Levin and Baltaxe observed a double PDA in 6% and early origin of PDA in 5% of patients.8
It is rare for the PDA to originate from the LAD even though continuation of the LAD around the apex is common. Baroldi and Scomazzoni described a patient whose PDA formed from the LAD and terminated at the crux.9 Clark et al described three patients whose PDA originated from the LAD and in all, the PDA terminated before the crux.10
Musselman and Tate reported a case in which the PDA originated from the LAD and continued beyond the crux. Later, the PDA divided in to two branches that went through both the left and right sides of atrioventricular groove; it also gave rise to atrioventricular nodal branch.11
Javangula and Kaul described another case in which a hyperdominant LAD continued as the PDA with coexistent aortic stenosis, probably an incidental finding, with diminutive RCA. However, in their case report, the LAD continued as the posterior descending artery up to the crux of the heart, and thereafter travelled for a brief distance as the distal right coronary artery after giving a smaller left ventricular branch to the inferior surface of the left ventricle. There was no communication between the atretic proximal RCA and the anomalous distal RCA.12 Hamodraka et al reported another case in which LAD continued as PDA in the presence of a small RCA.13
In our case, the LAD continued as the PDA beyond the crux into the left posterior atrioventricular groove with a small RCA. To the best of our knowledge, this is the second case report where the LAD continued as a PDA beyond the crux, and the first case for which successful primary percutaneous intervention was done.
The clinical implication of this anomaly is that if this type of hyperdominant LAD is occluded, a large infarction of the anterior wall, septum and inferior wall would be expected to occur, leading to cardiogenic shock, similar to our patient. An interventional cardiologist must be aware of such anomalies whenever performing a catheterization on patients who have suffered a large infarction involving both the anterior and inferior walls. Early revascularization is probably lifesaving for these patients, as in our case.
Acknowledgements
Written consent for publication was obtained from the patient.
Dr. M. Boochi Babu can be contacted at e_mbb99@yahoo.co.in.
References
- Cingoz F, Bingol H, Turan Yilmaz A, Tatar H. Left anterior descending artery arising as a terminal extension of posterior descending artery (a rare coronary artery anomaly). Interact Cardiovasc Thorac Surg. 2003 Dec; 2(4): 680-681.
- Banchi A. Morfologia delle arteriae coronariae cordis. Arch Ital Anat e Embriol. 1904; 3: 87-164.
- Schlesinger MJ. Relation of anatomic pattern to pathologic conditions of the coronary arteries. Arch Pathol. 1940; 30: 403-415.
- Baim DS. Coronary angiography. In: Baim DS, ed. Grossman’s Cardiac Catheterization, Angiography, and Intervention. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Phillips DA, Berman J. A variation in the origin of the posterior descending coronary artery. Cardiovasc Intervent Radiol. 1984;7(2):75-77.
- Ilia R, Gilutz H, Gussarsky Y, Gueron M. Anomalous origin of the posterior descending artery from the obtuse marginal. Cathet Cardiovasc Diagn. 1990 Jul;20(3):200-201.
- Errichetti A, Mills RM Jr, Mercadante NM, Lingley JF. Anomalous origin of the posterior descending artery from the first septal perforator. Cathet Cardiovasc Diagn. 1986;12(6):402-404.
- Levin DC, Baltaxe HA. Angiographic demonstration of important anatomic variations of the posterior descending artery. Am J Roentgenol Radium Ther Nucl Med. 1972 Sep;116(1):41-49.
- Baroldi G, Scomazzoni G. Coronary circulation in the normal and pathological heart. 2nd ed. Washington, D.C.: Office of the Surgeon General, Department of the Army; 1967: 10-13.
- Clark VL, Brymer JF, Lakier JB. Posterior descending artery origin from the left anterior descending: an unusal coronary artery variant. Cath Cardiovasc Diagn. 1985;11:167-171.
- Musselman DR, Tate DA. Left coronary dominance due to direct continuation of the left anterior descending to form the posterior descending artery. Chest. 1992; 102: 319-320.
- Javangula K, Kaul P. Hyperdominant left anterior descending artery continuing across left ventricular apex as posterior descending artery coexistent with aortic stenosis. J Cardiothorac Surg. 2007 Oct 21; 2: 42.
- Hamodraka ES, Paravolidakis K, Apostolou T. Posterior descending artery as a continuity from the left anterior descending artery. J Invasive Cardiol. 2005 Jun;17(6):343.
