


Hurry, It’s a STEMI! But How Quick is Too Quick for Safety?
Betty Brooks, RN, Manager of Quality Outcomes, from Heart and Vascular Institute at Memorial University Health Medical Center (MUHMC), in Savannah, Georgia, asked me to address a question from one of the cardiologists practicing at MUHMC:
University Health Medical Center (MUHMC), in Savannah, Georgia, asked me to address a question from one of the cardiologists practicing at MUHMC:
“Without an on-site, on-call interventionalist and lab team, there is a limit to how low the D2B [door-to-balloon] time can go before someone gets killed trying to get to the hospital to meet an arbitrary time frame. Is there a statistically significant difference in mortality, CHF [congestive heart failure], structural heart complications (ventricular septal defect, mitral regurgitation, and cardiac rupture) or life-threatening arrhythmias if the median D2B is 49 minutes vs. 70 minutes?”
I asked my expert cath lab colleagues to weigh in on this issue with 3 quick answers on whether forced reduction of D2B time is 1) beneficial for the patient or 2) the hospital or 3) the interventionalist, and if you have time, a short rationale. Here’s what they said.
Myocardial Ischemic Time (also known as Onset of Symptoms to Door, OTD) vs. D2B
Christopher White, Ochsner Clinic, New Orleans:
- The problem is the D2B time doesn’t tell you the “myocardial ischemic time,” which is what really matters. D2B is merely a surrogate. Certainly, the shorter the ischemic time, the better for the patient.
- Forcing very short D2B times will cost money, as teams will have to stay in the hospital, which is a loser for the hospital.
- Depending on the individual interventionalist’s status, the extra-on call money to stay in the hospital could be good for him/her, but for a more mature individual, the comfort of sleeping in their own bed may be more valued.
- Therapeutic hypothermia will be a game changer. STEMIs will be placed in hibernation and brought out of the freezer each morning for “elective PCI.”
David Holmes, Mayo Clinic: There has been no change in mortality since the D2B time has almost been halved (published from Michigan [e.g. Hanlon Study] and now the data from the NCDR [National Cardiovascular Data Registry]).
Peter Berger, The Geisenger Clinic: David (Holmes), well, about half the studies show no reduction in mortality, and about a half show, or suggest, a reduction in mortality — including this one [M. Kern: Onset of symptoms < 4 and D2B < 90 minutes had lowest mortality of all comparisons rather than just D2B < 90 minutes alone, Hanlon Study] from you. I don’t know any that showed an increase in mortality.
Barry Uretsky, University of Arkansas: Mortality reduction is a continuous function. The rise in mortality is trivial between 70-90 minutes. The goal is to save lives for the patient and preserve lives of the operators!
The Very Longest D2B
Magnus Ohman, Duke University: No study has suggested that having a whole interventional team in-house lowers mortality. If the interventional MD drives at breakneck speed and has an accident, the D2B time will be really, really long. So a measured response is the most appropriate.
Eric Bates, University of Michigan: No recent studies show further mortality reduction by shaving a few more minutes after the gains made with the initial interventions (see Rathore et al. Association of door-to-balloon time and mortality in patients admitted to hospital with ST elevation myocardial infarction: national cohort study. BMJ 2009; 338: b1807. doi: 10.1136/bmj.b1807.) An NCDR analysis (in press) will show no mortality reduction with a 15-minute time reduction over three years. Note the difference between an association between ischemic time and mortality, and the association between changing time and changing mortality rates. The same conundrum exists for high on-treatment platelet reactivity.
Inappropriate STEMI Activations?
Bob Applegate, Wake Forest University: As we shorten the D2Bs, we are doing so by relinquishing the interaction of those most experienced in the management of acute coronary syndromes, i.e. interventional cardiologists, to those least experienced, e.g. EMS and emergency department MDs. The potential benefit is an improvement in outcomes, but this is yet to be proven. The downside is an increase in inappropriate activation of health care resources for possible STEMI. In our system, at least, activation of the cath lab inappropriately is higher than comfortable and on a trajectory that is stretching cath lab resources thin.
Sunil Rao, Duke University: You asked for a “quick” thumbs up/thumbs down, but as you can see, the issues are complex! My understanding is that many hospitals are now requiring a 60-minute D2B time (like in the city of Miami), and while we can all agree that rapid treatment is important, I am not sure that reducing it way below 90 minutes at the expense of safety — operator, cath lab staff, and patient — is a good thing.
The fundamental problem is that we are mandated to reduce a surrogate endpoint, namely D2B time, rather than reduce mortality, which should be the goal. So many hospitals have complied by improving care processes and maybe also by “refining” the denominator. That is, by dropping out the sickest patients. What you end up with is low-risk patients getting super-fast door-to-balloon times. I once heard an interventionalist say “Well, if they’re going to measure door-to-balloon times, I’ll just deploy the balloon on the table,” which of course misses the point.
It reminds me of the likely apocryphal story of a post-WW II Eastern bloc country where the communist government realized that the annual production of tractors in the government-owned factory had dropped by 200 tons. So they mandated that the production of tractors increase by 200 tons the following year. Sure enough, the factory met that goal. The problem was that they didn’t make any more tractors; they just made each tractor heavier.
To answer your query directly: 1) Beneficial for the patient? Yes; 2) Beneficial for the hospital? Yes (CMS “forces” hospitals to reduce D2B times, and those with super-short times advertise this on billboards); 3) Beneficial for the interventionalist? Maybe (in some centers, operators that consistently have long D2B times get less cath lab time).
Gregg Stone, Columbia University: Numerous large-scale observational studies have shown a relationship between D2B time (and OTD) regarding mortality. But, now that we have shaved more than 30 minutes off our national D2B time, several studies show no effect of this reduction on decreasing mortality (Arch Intern Med 2009;169:1411-1419; Arch Intern Med 2010;170:1842-1849, NCDR, etc.). How can we rationalize these disparate findings? First is the issue of confounders. In large registry studies, who are the patients with long D2B times? This isn’t a chance occurrence. Long D2B times occur in patients who are the most ill (requiring medical stabilization), such as pulmonary edema, hypotension, arrhythmias, confusion, those unable to provide consent, etc. Of course their mortality will be higher, and the most sophisticated multivariable analysis cannot adequately control for all these variables.
Second, studies by our group, Brodie, and others have repeatedly shown that the relationship with D2B time and mortality is only present in high-risk patients with a large amount of myocardium at risk (e.g. anterior MI), and those presenting early in whom the myocardium is still viable (i.e. within 1-2 hours of symptom onset). Most [STEMI] patients present later, and a transmural infarct is complete in 2-3 hours, after which a shorter D2B time will matter little. For some reason, the guidelines have largely ignored this.
Third, institutions may be achieving shorter D2B times while inadvertently sacrificing (or ignoring) other important processes of care, such as medical stabilization prior to cath, optimal PCI procedures, and administration of guideline-based medical therapies after PCI. For example, bivalirudin and ticagrelor will have a greater effect on mortality than will 20 minutes of shorter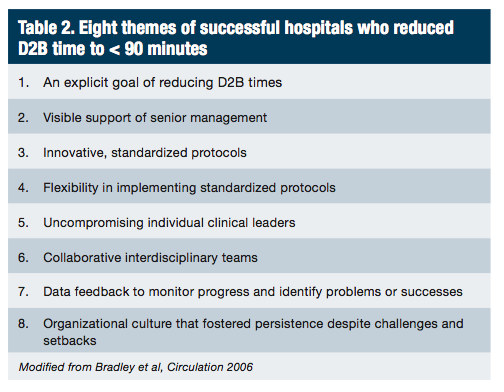 D2B time in most patients with STEMI. In contrast to what we are seeing with the D2B time experience, large registry studies have confirmed the results of these randomized trials, at least in terms of bivalirudin and survival (EHJ 2010; 31: 561-72; JACC Intv 2010; 3: 669-677; Am J Cardiol 2012; 110: 599-606; J Interv Cardiol 2012; 25: 278-288). This grand experiment once again reveals the difference in validity between the results of randomized trials and observational associations.
D2B time in most patients with STEMI. In contrast to what we are seeing with the D2B time experience, large registry studies have confirmed the results of these randomized trials, at least in terms of bivalirudin and survival (EHJ 2010; 31: 561-72; JACC Intv 2010; 3: 669-677; Am J Cardiol 2012; 110: 599-606; J Interv Cardiol 2012; 25: 278-288). This grand experiment once again reveals the difference in validity between the results of randomized trials and observational associations.
[Stone] Summary: Short D2B times are critical in a minority of patients, but the benefit of shortening D2B time in broad populations is masked when diluted by the vast majority in whom 15-30 minute faster reperfusion really doesn’t make much of a difference given late presentation, spontaneous reperfusion, or a small amount of myocardium at risk. Thus, if national outcomes are to be further improved we have to focus our considerable resources and efforts on other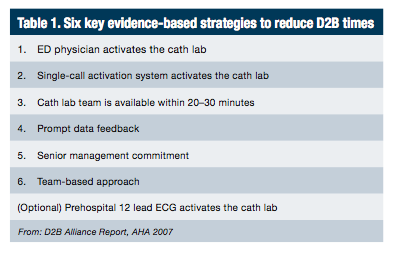 measures that have been shown to be beneficial.
measures that have been shown to be beneficial.
Ted Feldman, Evanston, Illinois: As both Bob Applegate and Gregg Stone have noted, we are activating our ER/code systems for many patients who derive little or no benefit. Guidelines that focus on the patients that benefit and triage the rest to less intensive early therapy are needed, especially as we are cutting budgets everywhere.
The Bottom Line
Morton Kern: From my take and in synthesizing my colleagues’ views, I doubt there is a measurable individual (but not national) hospital mortality difference between 90-70 minutes. I am not sure about less than 50 minutes, but we (our system) could never achieve this number no matter what we did, unless doctors and nurses lived in the hospital. One of our real methods to improve outcomes would be to reduce ‘ischemic time,’ that is, shortening the time from onset of symptoms to door of the ED. To answer Ms. Brooks questions as to whether forced reduction of D2B time is 1) beneficial for the patient or 2) the hospital or 3) the interventionalist, my answers are no, no, and no.
Finally, I thank my colleagues for their wonderful insights into this common and important problem. I have provided some practical suggestions from the literature on the subject. Please see Tables 1-3 to help reduce your D2B time and improve mortality in your STEMI program.
References
- Granger CB, Henry TD, Bates WE, Cercek B, Weaver WD, Williams DO. Development of systems of care for ST-elevation myocardial infarction patients. The primary percutaneous coronary intervention (ST-elevation myocardial infarction-receiving) hospital perspective. Circulation. 2007; 116 (2): e55-59.
- Bradley EH, Roumanis SA, Radford MJ, et al. Achieving door-to-balloon times that meet quality guidelines: how do successful hospitals do it?. J Am Coll Cardiol. 2005; 46 (7): 1236-1241.
- Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med. 2006 Nov; 355 (22): 2308-2320.
- Hannan EL, Zhong Y, Jacobs AK, Holmes DR, Walford G, Venditti FJ, Stamato NJ, Sharma S, King. Effect of onset-to-door time and Door-to-balloon time on mortality in patients undergoing percutaneous coronary interventions for ST-segment elevation myocardial infarction. Am J Cardiol. 2010; 106: 143-147.
- Cannon CP, Gibson CM, Lambrew CT et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000; 283 (22): 2941-2947.
