


Good Samaritan Hospital, Ron and Carol Cope Heart Center
 Tell us about the cath labs at Good Samaritan Hospital.
Tell us about the cath labs at Good Samaritan Hospital.

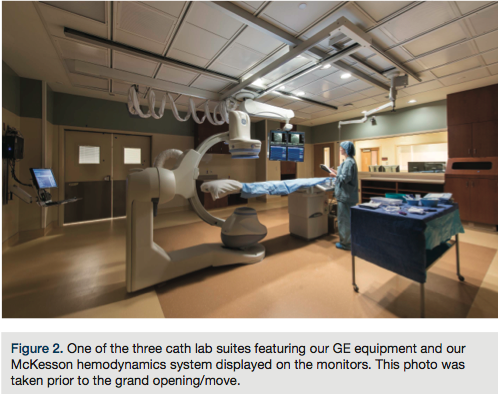
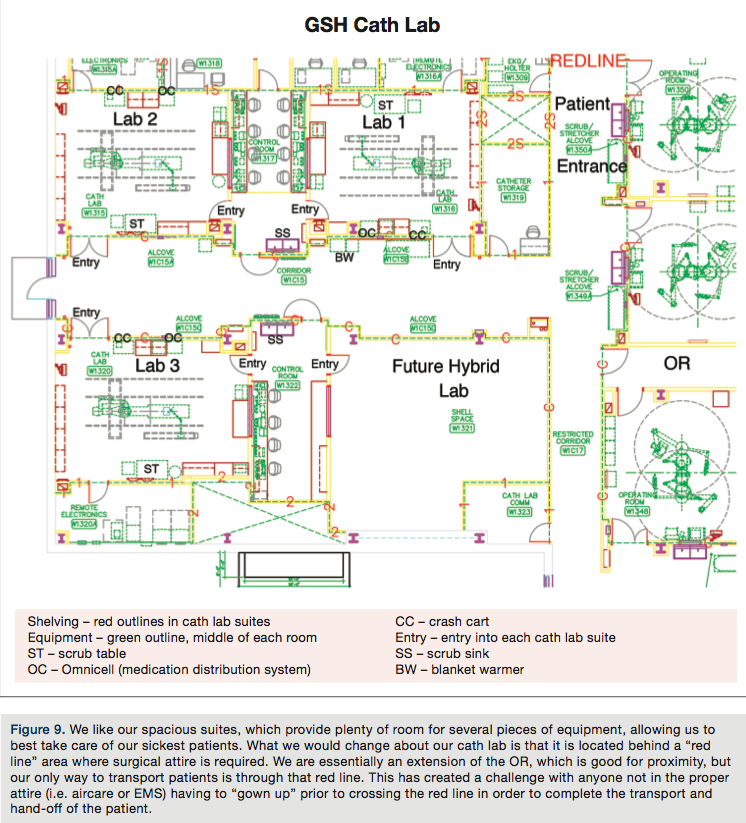
We recently moved into The Ron and Carol Cope Heart Center, a brand new addition to our hospital in September 2012. It features 3 GE labs with two primarily used for cardiac, and one dedicated to peripheral and pacemakers. A fourth lab is currently shelled out for a future hybrid lab. Our staff is comprised of seven registered nurses (RNs), two radiologic technologists (RTs), two cardiovascular technologists (CVTs), and four registered cardiovascular invasive specialists (RCISs). Staff ranges from 1-20+ years of cath lab experience.
What procedures does your cath lab perform?
We routinely perform right and left heart catheterization with coronary angioplasty and stenting, permanent pacemakers, implantable cardioverter defibrillators (ICDs), and bi-ventricular ICDs. We also perform peripheral vascular angiography with angioplasty and stenting, as well as valvuloplasty. We utilize intravascular ultrasound (IVUS), optical coherence tomography (OCT), fractional flow reserve (FFR), Impella 2.5 (Abiomed), coronary thrombectomy, and intra-aortic balloon pumps (IABPs). We are currently performing about 56 procedures per week.
Does your cath lab have surgical backup on site?
Yes, we have one cardiothoracic surgeon. He is available for surgical back up if necessary. As part of our new heart center addition, the OR is conveniently located just down the hallway from the cath lab.
How many of your diagnostic caths are normal?
In the CathPCI American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) ending in the third quarter of 2012, our incidence of non-obstructive coronary artery disease (elective patients only) is 35.1% (in US hospitals, 50th percentile is 44.1% and 90th percentile is 30.3%).
Do any of your physicians regularly gain access via the radial artery?
Six of our seven cardiologists routinely perform heart catheterizations using the right radial artery, as long as the patient passes an Allen’s test prior to cath. If a patient has had a previous coronary artery bypass graft surgery (CABG) in which the left internal mammary artery (LIMA) was used, we may access the left radial artery instead.
Who manages your cath lab?
Our cath lab management is a triad consisting of cath lab manager Stefanie Roper RN, RT(R)(CI), lead nurse Todd Tvrdik, RN, and lead tech Ashley Voet, RCIS.
Who scrubs, who circulates and who monitors?
Our lab utilizes the RCISs, CVTs, and RTs to scrub, and the RNs to circulate (give medications). Monitoring can be performed by either a nurse or a technologist. We recently implemented a four-person call team, which consists of two nurses and two technologists. Our fourth person, be it a nurse or technologist, helps circulate, get supplies, fill out paperwork, and answer phones. Our goal is to eventually have our staff cross-trained to allow flexibility in staffing and scheduling.
Does an RT (radiologic technologist) have to be present in the room for all fluoroscopic procedures in your cath lab?
An RT does not have to be present in the room for fluoroscopy to be performed; however, a physician must be present.
Which personnel can operate the x-ray equipment [position the image intensifier (II), pan the table, change angles, step on the fluoro pedal] in your cath lab?
Depending on the physician, the technologist or physician may position the II and table or change angles on the II. A physician must step on the fluoro pedal.
 How does your cath lab handle radiation protection for the physicians and staff?
How does your cath lab handle radiation protection for the physicians and staff?
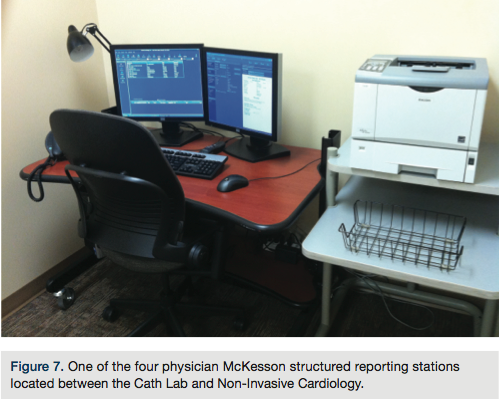
All staff members are instructed on radiation safety and annual competencies are maintained. Lead aprons are provided by the hospital and are checked for lead damage annually. Badge reports are available for all members of the cath lab to view. Fluoro times as well as radiation doses are monitored for each procedure and documented in our McKesson hemodynamics system. This information is then carried through to the physician-structured report.
What are some of the new equipment, devices and products introduced at your lab lately?
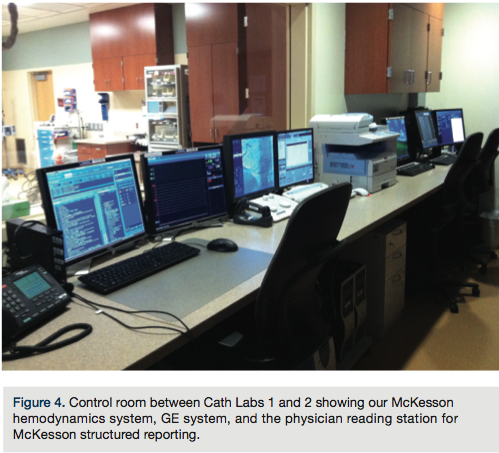
With the move into our new heart center, we updated all of x-ray equipment to GE, and implemented the McKesson hemodynamics monitoring system and physician-structured reporting. In the last year, we have purchased the Impella 2.5 (Abiomed) and OCT (St. Jude Medical), and started performing valvuloplasty.
 How does your lab communicate information to staff and physicians to stay organized and on top of change?
How does your lab communicate information to staff and physicians to stay organized and on top of change?

Our lead nurse is primarily in charge of the day-to-day phone calls and communication between departments. The lead tech is primarily in charge of staff scheduling and room/case assignments. They are in constant communication with our Procedure and Surgical Care Center, the nursing floors, physicians, and staff, and work together to keep everyone informed as to what needs to be done as the day progresses. As far as change and education, we are fortunate that our physicians take an active part in teaching and keeping our staff current with new studies, technologies, and equipment. We have also recently implemented a vendor clinical education day. We invite all of our vendors to come one morning every other month, and educate staff and physicians regarding new product or changes to any existing product. Our physicians meet monthly with our leadership team at a Cardiology Clinical Council to evaluate outcomes data and changes in processes. This information is then communicated at a cardiology management team meeting and then to staff at biweekly department meetings. A peer review process has recently been put in place as well to discuss mortalities and best practices. This process is completely physician driven and they have established a 75% mandatory attendance. With all of these processes in place, we strive to stay connected, ensuring the safest care for our patients.
How is coding and coding education handled in your lab?
Rocky Bailar, RCIS, is currently in charge our inventory. We have recently brought Tim Jones, RN, up to speed on coding and between the both of them, they are responsible for reconciling charges. They receive education via online courses and through the in-house hospital coding team. Rocky and Tim both provide education to cath lab staff on a day-to-day basis, as well as at our department meetings. Each cath lab nurse is responsible for coding/billing their own procedures and reordering equipment/supplies by scanning a barcode for each individual procedure and piece of equipment with our PAR Excellence scanning system. A report is printed from this system following the procedure and the monitor person is responsible for double-checking the charges. Rocky and Tim then do the final reconciliation of these charges prior to sending them to the finance department.
 Who pulls the sheaths post procedure, both post intervention and diagnostic?
Who pulls the sheaths post procedure, both post intervention and diagnostic?
Due to the high percentage of radial cases we perform and utilization of femoral closure devices, it is rare that we have to pull a femoral sheath. In the event that a femoral sheath does need to be pulled, it is the responsibility of the cath lab staff or cardiologist. For diagnostic cases, the sheath is pulled in the cath lab, while interventional cases are sent to a nursing floor and pulled at a later time. Sheaths are only left in if a closure device is contraindicated. For heparin patients, the activated clotting time (ACT) must be <150 per hospital policy to hold manual pressure when closure is not indicated. For other anticoagulants, it is left up to physician discretion as to when the sheath will be pulled. These would be the instances where patients are sent to a nursing floor (if intervention is performed) and pulled at a later time per physician order. Otherwise, sheaths are always pulled in the cath lab, with a closure device being the first preference. With most of our cases being radial, the manual pressure situation occurs infrequently. Post femoral closure device, patients may elevate the head of their bed 15-30 degrees. They usually remain this way for 2-3 hours and then are able to ambulate or sit in a chair. For radial patients, the compression band is weaned over the next 1-2 hours. They are instructed to not use that hand or wrist for the next two days. If cath lab staff is not available at the time of sheath removal, our interventional radiology technologists serve as a back-up sheath pull team. As part of the education of new staff, they are required to learn the sheath pull policy. Then, they must complete three assisted sheath removals and prove competency before being checked off to perform on their own.
 Where are patients prepped and recovered (post sheath removal)?
Where are patients prepped and recovered (post sheath removal)?
A pre-op telephone call is made to all outpatients prior 1-2 days prior to the procedure date. Much of their history is collected at this point and entered into a database. Upon arrival to our facility, our outpatient caths begin in our Procedure and Surgical Care Center (PSCC), where the patients are prepped for their procedure. In the PSCC, their history is reviewed and a physical assessment is added to the database. An IV is started, wrist/groin prep is completed, and procedure permits are signed. Once the patient is ready, the cath lab staff is responsible for transporting them to the cath lab. Upon completion of their cath, depending on the access site, arterial compression or closure is performed. We utilize the D-Stat Rad-Band (Vascular Solutions) and R-Band (Vascular Solutions), which are placed by the technologists. The R-Band works in a similar way to a FemoStop (St. Jude Medical) for the groin. The R-Band is simply a plastic band that velcros around the wrist, with a marker placed just proximal to the insertion site. Using an R-Band syringe, a small balloon is then inflated while the sheath is pulled. Enough air is then let out to ensure just enough pressure for hemostasis. For femoral access, hemostasis is achieved by either tech or physician deployment of Perclose (Abbott Vascular) or Angio-Seal (St. Jude Medical). Manual compression is used any time contraindication to a closure device is present.
How is inventory managed at your cath lab? Who handles the purchasing of equipment and supplies?
Rocky Bailar, RCIS, is in charge of our inventory. He works with the physicians, staff, and vendors to provide the appropriate equipment needed in the lab. He is in constant communication with the hospital’s Materials Management department and inventory team to verify the appropriateness of the equipment and to keep cost at a minimum. When considering using a new product (depending on the extent of education needed for physicians and staff), it must go through a process in Materials Management to determine cost effectiveness, whether any other CHI facility is already using it, and what other devices could be comparable. If approved, the vendor is invited to the facility and meets with manager Stefanie Roper, Inventory Specialist Rocky Bailar, Lead RN Todd Tvrdik, and Lead Tech Ashley Voet. Physicians may be invited to this meeting as well, if they have expressed previous interest in the product.
 Can you tell us more about your recent expansion and move?
Can you tell us more about your recent expansion and move?
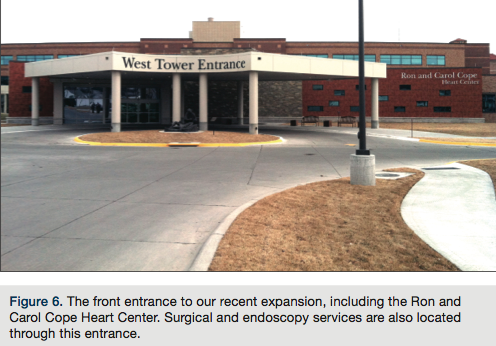
Our new heart center opened in September 2012. Our previous lab consisted of three cath lab suites (two for cardiac, and one for peripherals and pacemakers), as does our current lab. However, with the move, we almost doubled the size of our cath suites and purchased a new GE lab to make all three of our labs GE equipment. We also have a shelled-in fourth lab for future hybrid use. With the recent closure of an outpatient cath lab, we have seen our volume grow, as far as diagnostic cases are concerned. We provided the angioplasty coverage for those patients previously.
Is your lab involved in clinical research?
We are not currently involved in any clinical research.
Can you share your lab’s average door-to-balloon (D2B) times and some of the ways employees at your facility have worked together to keep D2B times under 90 minutes?
We collect this data in the CathPCI NCDR registry, and we are also members of the ACC D2B Alliance. Our median time to immediate PCI for STEMI patients (in minutes) for the rolling four quarters ending 2012Q3 is 52.5 minutes (US hospitals 50th percentile is 61.6 minutes and 90th percentile is 49.6). We are very excited to report our proportion of STEMI patients receiving immediate PCI within 90 minutes is 96.7% during the same timeframe (US hospitals 50th percentile is 93.4% and 90th percentile is 100%). We developed a Code STEMI policy in 2007. We have been working with the PDCA model (plan–do–check–act) for performance improvement to make improvements to our processes since that time.
Who transports the STEMI patient to the cath lab during regular and off hours?
During regular and off hours, a Code STEMI team is always available. This includes the house manager, ICU RN, lab, EKG, radiology, pharmacy, and a float secretary. Per hospital policy, it is the responsibility of the ICU RN responding to help transport the patient with one cath lab RN. Our hospital serves as a large rural referral center, so a large volume of our STEMI patients comes via aircare or ambulance. When coming by flight, the flight team brings them to the cath lab from the rooftop helipad upon arrival. If the STEMI patient is being transported by ambulance, the EMS crew transports them directly to the cath lab.
 What do you do when the call team is already busy doing a procedure and a STEMI comes into the ED?
What do you do when the call team is already busy doing a procedure and a STEMI comes into the ED?
We have recently revised our policy regarding after-hours cases. Guidelines have been signed off on by each cardiologist to determine whether patients are elective, urgent, or emergent. Only urgent and emergent cases are to be done after hours and on the weekends. Although our lab performs most of the pacemakers for our facility during normal operating hours, the cath lab staff is not available for pacemaker insertions on the weekends or after hours. The OR serves as the back up if such procedure is needed. If our call team is performing a procedure and a STEMI comes to the ED, the case will either be finished (if time allows) and the room quickly turned over, or the sheath is sewn in place and that patient may be brought back at a later time. Although we do not have a second call team in place, staff may be called in if warranted.
What measures has your cath lab implemented in order to cut or contain costs?
Rocky Bailar, RCIS, who is in charge of our inventory, maintains a close relationship with our vendors. He stays familiar with pricing changes, and new or changing equipment. This allows him to add or change our inventory as well as some of our practices to keep cost down. He also helps educate staff to make them more aware of procedure and equipment cost, and reimbursement.
What quality control measures are practiced in your cath lab?
Daily quality control is performed on our Avox Oxygen Saturation machine, as well as our Lifepack and crash carts. Our clinical engineering department works closely with vendors from various companies for quality assurance on a routine basis.
Are you recording fluoroscopy times and dosages?
Each patient’s fluoro time and dose is calculated by the GE equipment and recorded as part of the cath lab procedure log. This procedure log is part of the patient’s permanent medical record. The fluoroscopy times/dosages are also pulled into the physician-structured report.
 Who documents medication administration during the case?
Who documents medication administration during the case?
Medications are hand charted as a verbal order on an order set by the circulating RN, signed off on by the physician at the end of the case. The monitor person is also responsible for documenting medications on the McKesson hemodynamics system. The medication is time stamped through the McKesson system and becomes part of the cath lab procedure log. The documents are compared and verified at the end of the case, and both are made a part of the permanent chart.
How does your cath lab compete for patients? Has your institution formed an alliance with others in the area?
Being in south central Nebraska, we provide cardiac services for a very large area of patients. Our cardiologists cover outreach clinics as far north as the Nebraska/South Dakota state line and as far south as north central Kansas. Our physicians also provide coverage as far west as the Nebraska/Colorado state line. Each cardiologist has a number of outlying facilities they visit on a rotating schedule to establish physician and patient relationships, and provide care for patients living miles away. This also makes follow-up care easier for patients who live in the outlying communities. Stephanie Kee, Cardiology Clinical Coordinator, along with physician support, provides STEMI education to these communities to help establish a standard of care for all of our patients. As of December 2012, our cardiac area became part of a statewide cardiovascular service line called Nebraska Heart Institute. Currently, this includes four other facilities, three of which also have cath labs. With this service line, we aim to provide faster and safer care to our patients throughout the state of Nebraska.
How are new employees oriented and trained at your facility?
New employees receive an orientation workbook and a dedicated preceptor. They start by just observing in the cath lab and pre/post areas. Nurses also get the opportunity to spend time in the ICU recovering coronary artery bypass graft surgery patients to gain critical care experience. All staff is encouraged to observe an open-heart surgery to help them further understand cardiac anatomy. After that, the orientee is introduced to their primary role (scrubbing or circulating). Much of the remainder of the orientation process is spent becoming familiar with their primary role. We do, however, like to have nurses scrub in a few times during their orientation, as well as technologists circulate (within their scope) to understand the whole picture of the team. Towards the end of orientation, staff is introduced to monitoring. They are educated on ACC definitions and the importance of accurate point of care documentation. The Wes Todd Review CDs and books (www.westodd.com) are used for further staff education, and assignments are made for all staff biweekly to maintain competence and encourage job growth. Vendors provide education on a rotating basis for staff on our low volume/high risk procedures and equipment. This also ensures everyone maintains competency and confidence. Our vendor clinical education also serves as a good education opportunity.
What continuing education opportunities are provided to staff members?
Our hospital performs an annual audit to determine areas of opportunity for continuing education. Various seminars are then set up during the year for staff to attend and gain CE credits. Our nursing profession development council (part of our shared governance) also ensures continuing education, and provides opportunities such as skills labs and nursing noon conferences. Vendor education is provided specifically for cath lab staff, as well as various webinars and PESI Healthcare conferences.
 How do you handle vendor visits to your lab?
How do you handle vendor visits to your lab?
Vendors are allowed in by appointment only. Per our vendor policy, any vendor present in the cath lab must be participating in direct patient care. If they need to in-service on a new or changing product, this is done outside of the cath lab, away from the procedural area. Upon arrival to the facility, the vendors are required to check in (our hospital uses the Reptrax system). Through this program, they receive a badge for staff throughout the hospital to identify them.
How is staff competency evaluated?
Each time education is presented by a vendor, an attendance record is kept and stored in a notebook for future reference. All Wes Todd quizzes that are completed are also kept for reference. We evaluate competency annually based on performance and education. At the end of each year, staff must turn in a skills checklist. This list includes all of the education staff has attended in the last year. HealthStream education is also a big part of hospital-wide competency. Staff is assigned modules frequently throughout the year. This must be completed by the set due date in order for staff to continue working.
Does your lab have a clinical ladder?
Our hospital does have a clinical ladder for nursing. The cath lab currently does not have a separate one, but will be considering it in the near future.
How does your lab handle call time for staff members?
Call is scheduled on a rotating basis. We currently schedule every third weekend and 1-2 nights per week. The call teams are comprised of four staff, two nurses and two technologists. The teams stay the same unless call is traded between individuals. We currently place an experienced tech or nurse with one of less experience to continue to provide education for new employees and provide a safe environment for our patients.
Within what time period are call team members expected to arrive to the lab after being paged?
The call team is expected to arrive in the lab within 30 minutes of the page. Most people live within call range; however, we do have an apartment that is dedicated to the cath lab in the event of severe weather and for staff who reside outside of the call area.
Do you have flextime or multiple shifts?
Our cath lab staff is scheduled to work four ten-hour shifts per week, from 0700 to 1730. Due to our physicians’ outreach and clinic schedules, we do have some slower days. Staff are given the opportunity to stay and complete chart audits for ACC-NCDR, work on our “to-do” list given our recent move, or flex out.
Has your lab recently undergone a national accrediting agency inspection?
We have not recently undergone an inspection; however, our hospital was the first in Nebraska to become accredited as a Chest Pain Center in 2005. We are currently working on our 4th level of PCI accreditation with the Society of Cardiovascular Patient Care.
Where is your cath lab located in relation to the operating room (OR) and emergency department (ED)?
With the recent expansion of the hospital and new heart center, there has been both good and bad, as far as location. We previously were close to the ED and had an elevator directly down from the helipad. With our new location, we are farther from the ED and helipad, but share the same location as the OR. The cath lab, ED, and OR are all on the ground floor. With the distance between the cath lab and ED, some process changes have taken place to ensure safe patient transport and handoff.
What trends have you seen in your procedures and/or patient population?
The biggest trends we are seeing are an elevation of our average patient age and sicker patients, having a history of coronary artery disease and possibly multiple prior cardiac procedures. With emphasis being placed on appropriate use criteria, non-invasive stress testing prior to a cath lab procedure has also become a standard of care due to reimbursement purposes.
What is unique or innovative about your cath lab and staff?
Our cath lab focuses a lot on quality outcomes, and understanding the importance of accurate data entry and the ACC-NCDR. Point-of-care data input is a part of both an RN and technologist’s job from the beginning. As part of orientation, they meet with Stephanie Kee to review ACC definitions. Notebooks with updated ACC definitions are available for all staff and quizzes are done randomly throughout the year to ensure growing knowledge in the area of ACC definitions. At each department meeting, there is time set aside to discuss ACC items and upcoming deadlines. Staff are not only very involved in point-of-care data entry, but they also help in auditing charts to collect discharge data on each patient. This data is then cleaned up by Stephanie Kee to submit to the NCDR. Although this process may not be a common practice throughout our state, it has definitely helped deliver accurate outcomes while keeping staff engaged in the process.
Is there a problem or challenge your lab has faced?
The past year was met with many challenges. We orientated many new staff, implemented a change in management team, launched the McKesson hemodynamics system and structured reporting system, and we moved into our new heart center. We have been very fortunate with our new manager and new management team. They have worked hard to provide a very structured orientation process for new employees, build relationships within the hospital, and rewrite and update many policies and procedures. Our new heart center and cath labs are spacious and beautiful, and our staff has adjusted to the move well. Our new employees have stepped up to the challenge of learning the ways of a cath lab and are doing very well. They have dedicated a great deal of time into developing themselves as cath lab employees and worked well with experienced staff to form a great cath lab team. We have all worked very hard this past year and it has definitely paid off.
What’s special about your city or general regional area in comparison to the rest of the U.S.? How does it affect your “cath lab culture”?
Good Samaritan Hospital is located in a small community of approximately 30,000 people in Kearney, Nebraska. We provide cardiovascular services to half of the state of Nebraska and parts of north central Kansas. A vast majority of our patients are farmers and ranchers who live many miles away. Most of our STEMIs are brought in by aircare or ground ambulance, and are referred to us through physician and patient relationships set up through our cardiology outreach services. Having gone through so many changes in the past year, our “cath lab culture” has become very strong. Our community is small, which creates a close work environment. Our physicians have a strong sense of trust in our cath lab staff that helps develop teamwork and creates a safe environment for both patients and physicians.
The Society of Invasive Cardiovascular Professionals (SICP) has added two questions to our spotlight:
Do you require your clinical staff members to take the registry exam for Registered Cardiovascular Invasive Specialist (RCIS)? Does staff receive an incentive bonus or raise upon passing the exam?
We do not currently require our technologists to be RCIS-certified or Cardiac Interventional-certified. We do, however, highly encourage it and would like to incorporate the RCIS and CI credentials into our clinical ladder as an incentive for increase in salary for both nurses and technologists.
Are your clinical and/or managerial team members involved with any professional organizations that support the invasive cardiology service line, such as the SICP, ACVP, or regional organizations?
Yes, Stephanie Kee maintains Cardiac Care Associate (CCA) membership with the American College of Cardiology.
The authors can be contacted via Stefanie Roper, RN, RT(R)(CI), at: StefanieRoper@catholichealth.net.
