


FY 2013 Financial Update & Value-Based Purchasing: How the Cardiac Cath Lab Can Influence Reimbursement
 This is an interesting and exciting time in healthcare — the industry is abuzz with new ideas, changing regulations, and innovative strategies leading to a transformation in how care is provided in this country. The paradigm shift that healthcare is experiencing consistently circles back to several common themes, though the most consistent topic is related to healthcare finances!
This is an interesting and exciting time in healthcare — the industry is abuzz with new ideas, changing regulations, and innovative strategies leading to a transformation in how care is provided in this country. The paradigm shift that healthcare is experiencing consistently circles back to several common themes, though the most consistent topic is related to healthcare finances!
 In addition to the customary annual payment updates, provider facilities can now expect to work harder to achieve payment rewards and/or avoid payment penalties associated with performance. The CMS Fiscal Year (FY) 2013 Inpatient Prospective Payment System (IPPS) Final Update and proposed FY 2013 Outpatient Prospective Payment System (OPPS) payment changes reflect a positive outlook for hospitals providing cardiovascular services. The CMS Hospital Value-Based Purchasing (VBP) program, however, provides an element of “mandatory competition” to the already complex healthcare landscape for FY 2013 and subsequent years.
In addition to the customary annual payment updates, provider facilities can now expect to work harder to achieve payment rewards and/or avoid payment penalties associated with performance. The CMS Fiscal Year (FY) 2013 Inpatient Prospective Payment System (IPPS) Final Update and proposed FY 2013 Outpatient Prospective Payment System (OPPS) payment changes reflect a positive outlook for hospitals providing cardiovascular services. The CMS Hospital Value-Based Purchasing (VBP) program, however, provides an element of “mandatory competition” to the already complex healthcare landscape for FY 2013 and subsequent years.
This article covers the FY 2013 updates, the impact that VBP has on reimbursement, and how cath labs can strive for the best possible reimbursement scenario.
FY 2013 IPPS Payment Update
Under the final rule, overall payment rates to general acute care hospitals will increase by 2.8% in FY 2013. This percentage reflects a net update after the market basket update, improvements in productivity, a statutory adjustment factor, and adjustments for hospital documentation and coding changes. The overall rate increase is slightly reduced when combined with other adjustments in the final rule. This results in a net increase of Medicare’s operating payments to acute care hospitals by approximately 2.3% in FY 2013.
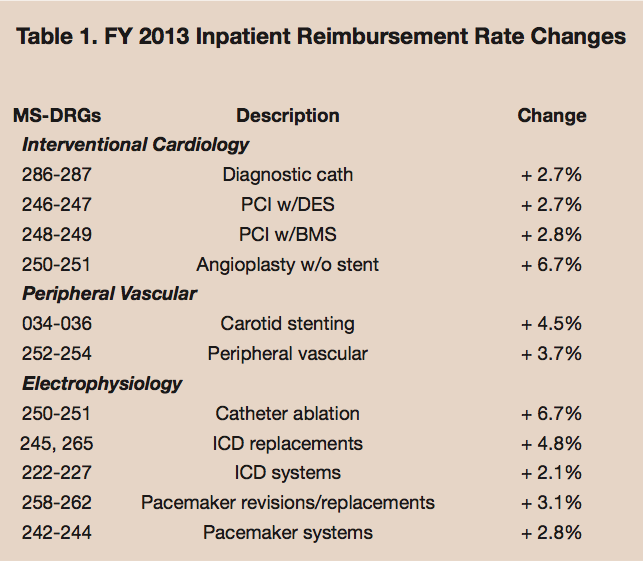 The overall FY 2013 IPPS financial forecast for cath lab-related MS-DRGs is also positive. In nearly all categories, the majority of the MS-DRGs show an increase in payment over last year, and every cath lab-related MS-DRG category likewise shows an increase in reimbursement. Table 1 summarizes the FY 2013 weighted average cath lab-related MS-DRG category reimbursement rate changes.
The overall FY 2013 IPPS financial forecast for cath lab-related MS-DRGs is also positive. In nearly all categories, the majority of the MS-DRGs show an increase in payment over last year, and every cath lab-related MS-DRG category likewise shows an increase in reimbursement. Table 1 summarizes the FY 2013 weighted average cath lab-related MS-DRG category reimbursement rate changes.
CY 2013 OPPS Proposed Payment Update
An overall outpatient payment increase of 2.1% is proposed for those hospitals that have reported their performance on identified quality measures. While the proposed payment for most cath lab outpatient procedures has increased, there are a few procedures that are proposed to reflect a significant decrease. This can be a cause for concern, especially as procedures that have been traditionally billed as inpatient continue to move to an outpatient status. The Ambulatory Payment Category (APC) experiencing the most negative impact in the proposed rule is APC 0083 — coronary angioplasty and percutaneous transluminal angioplasty (PTA) of a lower extremity without a stent, which could experience a 12% reimbursement decline.
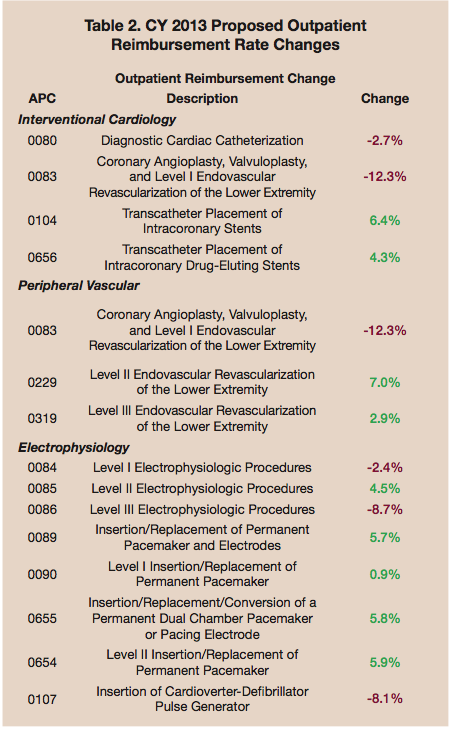 Outpatient ICD replacement, diagnostic cath, ablation, and electrophysiology (EP) studies are also experiencing some decline in payment, though not as dramatic. The APC rates provided in Table 2 do not include the reimbursement of other APC codes that may be billed in the same setting of care. Also, the outpatient rate changes listed are still proposed, and are subject to change in the final ruling, which is still pending release as of publication.
Outpatient ICD replacement, diagnostic cath, ablation, and electrophysiology (EP) studies are also experiencing some decline in payment, though not as dramatic. The APC rates provided in Table 2 do not include the reimbursement of other APC codes that may be billed in the same setting of care. Also, the outpatient rate changes listed are still proposed, and are subject to change in the final ruling, which is still pending release as of publication.
Value-based purchasing…starts now
Beginning this month, October 2012 (the start of FY 2013), the VBP program will begin affecting payments to hospitals for inpatient discharges occurring on or after October 1. Hospitals can expect to receive payment adjustments for their performance in January 2013. In the recent past, hospitals have benefited from a full update of the annual reimbursement payment if they have simply reported quality measures to CMS via the Hospital Inpatient Quality Reporting (IQR) Program. The VBP program augments this payment incentive by not only requiring reporting, but also achieving positive performance on the reported measures. Only hospitals with good or improved quality and patient satisfaction scores will be rewarded with the incentive payment, which will be determined by their performance during specific time periods defined by CMS. Hospitals with mediocre or poor scores will, conversely, break even, or worse, be penalized due to the redistributive nature of the budget-neutral program. In other words, all participating hospitals will be sharing the same pool of payment funding, resulting in competition among hospitals striving to be at top performance compared their competitors, so that additional money is gained.
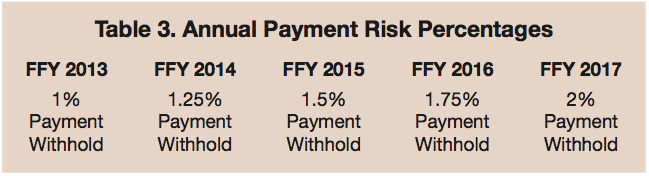 At stake for FY 2013 is a straight 1% reduction in base MS-DRG payments, which represents the dollars used to fund the VBP program. Essentially, the VBP system rewards and punishes hospital providers as a ‘pay-back’ system. For the next five years, the withhold percentage will gradually increase by 0.25% annually until it reaches a total 2% reduction by FY 2017. As previously alluded, hospitals are at risk for not achieving ‘pay-back’ if they do not achieve or exceed total performance scores that beat the majority of participating hospitals. Table 3 outlines the anticipated base payment reductions for each of the first five years of the VBP program.
At stake for FY 2013 is a straight 1% reduction in base MS-DRG payments, which represents the dollars used to fund the VBP program. Essentially, the VBP system rewards and punishes hospital providers as a ‘pay-back’ system. For the next five years, the withhold percentage will gradually increase by 0.25% annually until it reaches a total 2% reduction by FY 2017. As previously alluded, hospitals are at risk for not achieving ‘pay-back’ if they do not achieve or exceed total performance scores that beat the majority of participating hospitals. Table 3 outlines the anticipated base payment reductions for each of the first five years of the VBP program.
Time periods
For FY 2013, payment amounts will be based on clinical process and patient experience performance from July 1, 2011 to March 31, 2012. This is known as the “Performance Period.” A hospital’s scores from the Performance Period will be compared to benchmarks created in the Baseline Period, defined by the date range of July 1, 2009 to March 31, 2010.
In FY 2014, the time periods will change, and new aspects will be added to payment calculations. The Performance Period for clinical process of care (mainly CORE measures) and patient experience of care Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) is April 1, 2012 to December 31, 2012. These measures compare to a Baseline Period of April 1, 2010 to December 31, 2010. The FY 2014 newly-introduced mortality outcome measure Performance Period spans a twelve-month period from July 1, 2011 to June 30, 2012, and the Baseline Period for this measure domain is July 1, 2009 to June 30, 2010.
What is being measured?
Hospitals will still report data on the measures in the Inpatient Quality Reporting (IQR) measure set to receive full payment updates. There are certain measures under the Hospital VBP Program that are selected from the IQR measure set. Interestingly, many of these measures are specific to the patient population that is serviced within the cath lab. The Hospital IQR Program is intertwined with the Hospital VBP Program since the measures and reporting infrastructure for both programs overlap.
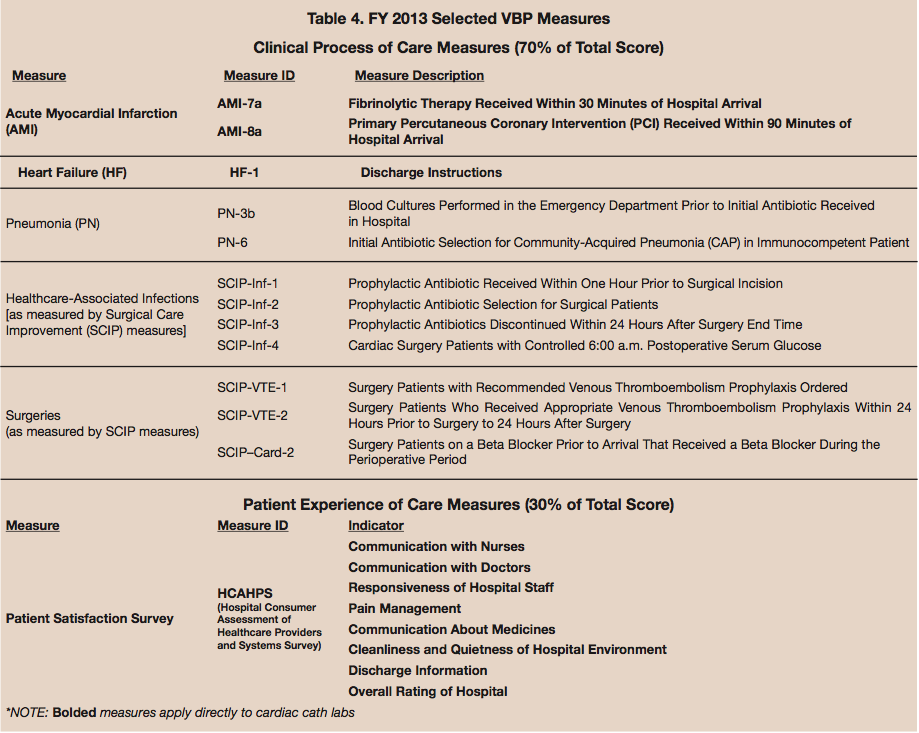 Of the quality measures reported and collected in the Hospital IQR Program, 13 will be evaluated and scored in FY 2013 for hospitals providing applicable services related to these measures. These measures are allocated into two care domains: 1) the Clinical Process of Care Domain and 2) the Patient Experience of Care Domain. The clinical process domain consists of select core measures, four of which apply directly to the cardiac cath lab (see bolded measures in Table 4), and an additional six of which that relate to cardiovascular and open heart surgery services. Eight HCAHPS survey categories make up the patient experience domain. Table 4 displays the selected core measures [including cath lab measures] and HCAHPS indicators included in the FY 2013 VBP program.
Of the quality measures reported and collected in the Hospital IQR Program, 13 will be evaluated and scored in FY 2013 for hospitals providing applicable services related to these measures. These measures are allocated into two care domains: 1) the Clinical Process of Care Domain and 2) the Patient Experience of Care Domain. The clinical process domain consists of select core measures, four of which apply directly to the cardiac cath lab (see bolded measures in Table 4), and an additional six of which that relate to cardiovascular and open heart surgery services. Eight HCAHPS survey categories make up the patient experience domain. Table 4 displays the selected core measures [including cath lab measures] and HCAHPS indicators included in the FY 2013 VBP program.
How scores are calculated
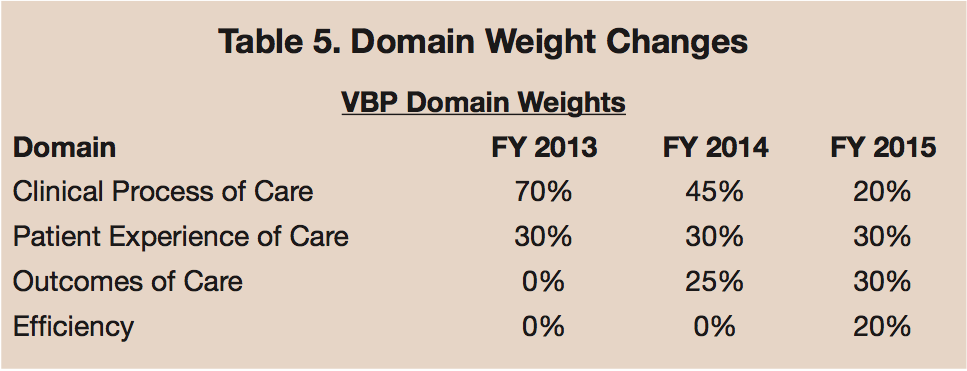 A hospital’s performance assessment domain scores culminate into a Total Performance Score that determines the level of payment the hospital will receive. For FY 2013, the domain totals are weighted with 70% of the total score allocated to the clinical process of care domain and 30% allocated to the patient experience of care domain. CMS VBP payment incentives and penalties aim to encourage achievement of high-quality care and improvement in quality of care for both domains.
A hospital’s performance assessment domain scores culminate into a Total Performance Score that determines the level of payment the hospital will receive. For FY 2013, the domain totals are weighted with 70% of the total score allocated to the clinical process of care domain and 30% allocated to the patient experience of care domain. CMS VBP payment incentives and penalties aim to encourage achievement of high-quality care and improvement in quality of care for both domains.
Looking ahead to FY 2014, an outcome domain measuring 30-day mortality indicators will be added to the Total Performance Score calculation. The specific mortality measures include 30-day mortality rates for Acute Myocardial Infarction, Heart Failure, and Pneumonia (MORT-30-AMI, MORT-30-HF, MORT-30 PN). The inclusion of the outcomes domain to the total score alters the weights to a mix of 45% process, 30% experience, and 25% outcomes. CMS will incorporate new measures and an efficiency domain for FY 2015, which will be accompanied by another shift in domain weights.
What can the cardiac cath lab team do?
Based on Corazon experience, the staff in the cardiac cath lab can play a major role in achieving — or hindering the ability to achieve — the highest possible reimbursement for their hospital. Four of 13 measures evaluated in the VBP program are directly associated with performance in the cath lab setting (AMI-7a, AMI-8a, HF-1, and HCAHPS). This means that 31% of the total performance score can be affected by those who see patients in the cath lab. Therefore, to assist in contributing to a positive reimbursement reward, members of the cath lab team will need to heavily focus on improving quality, patient satisfaction, and outcomes.
Corazon recommends the following to cath lab staff, and hospitals in general, for maximum attainment of reward potential:
- Develop a Continuous Quality Improvement (CQI) Program for the cath lab, which reviews structure, process, and outcomes and employs appropriate corrective action.
- Consistently collect and track quality and patient satisfaction data and results via internal dashboards to monitor and chart progress against internal and national benchmarks, especially for VBP measures pertaining to your hospital. Submission to the American College of Cardiology-NCDR CathPCI Registry, for example, is one way to ensure this process occurs.
- Implement an improvement action plan for correcting deficiencies causing lower quality and patient satisfaction scores as identified by the benchmarking process mentioned above.
- Report measures as required through the Hospital IQR and administer the HCAHPS survey to patients.
- Host VBP programs and meetings with all cath lab physicians, cath lab staff, and representatives from the financial and medical records departments to ensure understanding of the implications of the VBP program.
- Empower cath lab staff to be patient care ambassadors for quality care delivery and the creation of positive patient experiences. Staff must be responsive to patient satisfaction issues.
- Provide customer satisfaction workshops to train all staff members in techniques that will enhance the cath lab environment for patients.
The combination of cost control and achievement of positive care and patient satisfaction measures can have a lasting impact on the financial performance of your hospital. Although the VBP program produces the emergence of hospital “winners and losers,” it also provides the opportunity for hospitals to gain incentive rewards both now and in the future. Participation in VBP with a greater focus on the finances associated with individual clinical services, such as the cath lab, is a great stepping stone towards bundled payments (to be discussed in greater detail in a later publication). Constant, concentrated effort on patient-centered care by way of quality and satisfaction enhancement can have downstream effects that will put your hospital in great position to be a provider of choice, and can help prepare for any other future programs. The cath lab can be the leading agent for hospital change by providing significant contributions to reimbursement.
Catherine is a Decision Support Specialist and Kristi is a Consultant with Corazon, offering strategic program development in the heart, vascular, neuro and orthopedics specialties, offering a continuum of consulting, recruitment, interim management, and physician practice & alignment services across the country and in Canada. For more information, visit www.corazoninc.com, or call (412) 364-8200.
To reach the authors, email:
cdinardo@corazoninc.com or
kpowers@corazoninc.com.
