


Coronary Perfusion via Single Patent Conus Artery in the Presence of Severe Native Artery and Coronary Bypass Graft Disease
Case
 A 65-year-old male with advanced atherosclerotic coronary artery disease (CAD) status post third re-do coronary artery bypass grafting (CABG) with initial five-vessel bypass in 1984 followed by subsequent three-vessel bypass in 1998, systolic heart failure with left ventricular ejection fraction of 45%, peripheral arterial disease status post endovascular repair of abdominal aortic aneurysm, hypertension, dyslipidemia, and active tobacco use presented with recurrent Canadian Class III angina symptoms. On admission, physical examination was
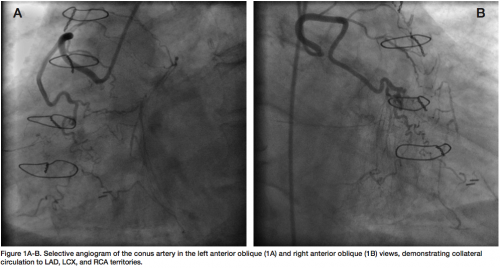
A 65-year-old male with advanced atherosclerotic coronary artery disease (CAD) status post third re-do coronary artery bypass grafting (CABG) with initial five-vessel bypass in 1984 followed by subsequent three-vessel bypass in 1998, systolic heart failure with left ventricular ejection fraction of 45%, peripheral arterial disease status post endovascular repair of abdominal aortic aneurysm, hypertension, dyslipidemia, and active tobacco use presented with recurrent Canadian Class III angina symptoms. On admission, physical examination was 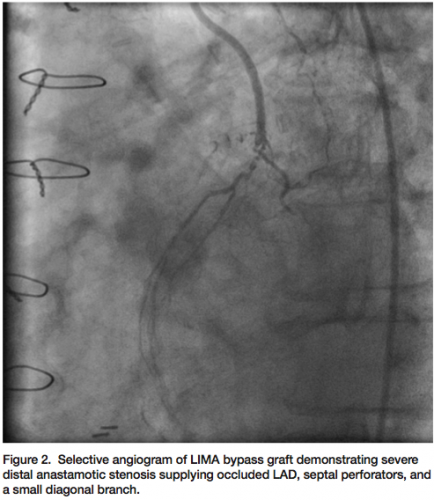 significant for heart failure with jugular venous distension and lower extremity edema; laboratory analysis was unremarkable for myocardial infarction with negative cardiac biomarkers; and diagnostic testing that was non-contributory with an unchanged baseline electrocardiogram. Subsequent coronary and graft angiography revealed a large conus artery via a separate ostium from the right coronary artery supplying a rich network of collaterals to the distal right posterior descending, distal left obtuse marginal, and mid to distal left anterior descending (LAD) arteries (Figure 1). Although the left internal mammary artery (LIMA) bypass graft to the LAD was patent, the native LAD was noted to be occluded distal to the anastamosis supplying only two septal perforators, as well as a small diagonal branch jeopardized by a severe 90% distal bypass graft anastamotic lesion (Figure 2). A decision was made to perform percutaneous coronary intervention on the anastamotic lesion between the LIMA graft and the LAD to revascularize the ischemic myocardial territory in this patient with unstable angina and depressed LV function.
significant for heart failure with jugular venous distension and lower extremity edema; laboratory analysis was unremarkable for myocardial infarction with negative cardiac biomarkers; and diagnostic testing that was non-contributory with an unchanged baseline electrocardiogram. Subsequent coronary and graft angiography revealed a large conus artery via a separate ostium from the right coronary artery supplying a rich network of collaterals to the distal right posterior descending, distal left obtuse marginal, and mid to distal left anterior descending (LAD) arteries (Figure 1). Although the left internal mammary artery (LIMA) bypass graft to the LAD was patent, the native LAD was noted to be occluded distal to the anastamosis supplying only two septal perforators, as well as a small diagonal branch jeopardized by a severe 90% distal bypass graft anastamotic lesion (Figure 2). A decision was made to perform percutaneous coronary intervention on the anastamotic lesion between the LIMA graft and the LAD to revascularize the ischemic myocardial territory in this patient with unstable angina and depressed LV function.
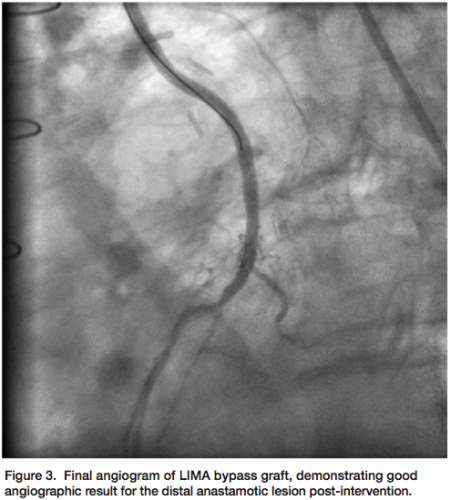 A 6 Fr IM guide was used to selectively engage the LIMA graft and a Miracle Bros 12 gram-tip wire (Asahi Intecc) advanced into the largest septal perforator. An NC Quantum Apex 2 x 15 mm balloon (Boston Scientific) was used to predilate the distal anastomotic lesion, a Promus 2.25 x 18 mm stent (Boston Scientific) was deployed, and an NC Quantum Apex 2.5 x 8 mm balloon was used to post-dilate the stent. Final angiogram demonstrated excellent stent result and TIMI-3 flow (Figure 3). The patient was discharged the following day on dual antiplatelet therapy and has been seen in follow up without recurrence of angina on optimized medical therapy.
A 6 Fr IM guide was used to selectively engage the LIMA graft and a Miracle Bros 12 gram-tip wire (Asahi Intecc) advanced into the largest septal perforator. An NC Quantum Apex 2 x 15 mm balloon (Boston Scientific) was used to predilate the distal anastomotic lesion, a Promus 2.25 x 18 mm stent (Boston Scientific) was deployed, and an NC Quantum Apex 2.5 x 8 mm balloon was used to post-dilate the stent. Final angiogram demonstrated excellent stent result and TIMI-3 flow (Figure 3). The patient was discharged the following day on dual antiplatelet therapy and has been seen in follow up without recurrence of angina on optimized medical therapy.
Discussion
The first branch that typically arises from the right coronary artery (RCA) is the pulmonary conus artery, or conus artery (CA). In a variable proportion of the population (between 30% and 50%), this artery originates with an independent ostium in the right sinus of Valsalva, anterior and superior to the ostium of the RCA1, and has been described as “the third coronary artery.”2 The anterior and superior course of the CA is usually short, and irrigates the pulmonary infundibulum and the supraventricular crest. It usually forms an anastamosis with the corresponding branch from the left coronary artery. This anastomosis lies on the distal part of the bulbous cordis (truncus arteriosus) and is known as the Vieussen’s arterial ring.3
Collateral circulation is a key factor in the pathophysiology of CAD. Symptoms and prognosis among patients with advanced CAD depend largely on the degree of collateral circulation.4 The CA branch of the RCA has a special anatomic and functional significance in the development of collaterals between the right and left coronary arterial systems. The CA may also arise as a separate branch from the aorta, and may not even be visualized by selective angiography due to its small size in patients with mild disease, only manifesting itself in advanced CAD when it is recruited to provide collateral circulation to under-perfused myocardial territories.5
Herein we describe a case of a large conus artery with a separate ostium supplying extensive collaterals to the left and right coronary territories in the setting of advanced CAD, thereby allowing critical percutaneous coronary intervention of a severe anastamotic lesion of the LIMA bypass graft supplying further collaterals to additional underperfused myocardial segments.
Dr. George can be contacted at jcgeorgemd@hotmail.com.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
References
- Levin DC, Beckmann CF, Garnic JD, Carey P, Bettmann MA. Frequency and clinical significance of failure to visualize the conus artery during coronary arteriography. Circulation 1981;63:833-837.
- Vilallonga R. Anatomical variations of the coronary arteries: I. The most frequent variations. Eur J Anat 2003;7:29-41.
- Yamagishi M, Haze K, Tamai J, Fukami K, et al. Visualization of isolated conus artery as a major collateral pathway in patients with total left anterior descending artery occlusion. Cathet Cardiovasc Diagn 1988;15(2):95-98.
- de Agustín JA, Marcos-Alberca P, Hernandez-Antolin R, et al. Collateral circulation from the conus coronary artery to the anterior descending coronary artery: assessment using multislice coronary computed tomography. Rev Esp Cardiol 2010;63(3):347-351.
- Rathor AL, Gooch AS, Maranhao V. Survival through conus artery collateralization in severe coronary artery heart disease. Chest 1973; 63; 840-843.
Disclosure: Dr. George reports he is a consultant for Boston Scientific. Dr. Desai and Dr. Kovach report no conflicts of interest regarding the content herein.
