


Co-Management of the Cardiovascular Service Line: Using Hospital-Physician Alignment to Achieve Common Goals
 Hospitals and health systems continue to seek ways to align their interests with those of their cardiologists in order to achieve common goals. The challenge lies in finding the correct alignment model or structure. Corazon believes that co-management can be a first step toward true clinical integration between the hospital or health system and physicians.
Hospitals and health systems continue to seek ways to align their interests with those of their cardiologists in order to achieve common goals. The challenge lies in finding the correct alignment model or structure. Corazon believes that co-management can be a first step toward true clinical integration between the hospital or health system and physicians.
The main purpose of a co-management agreement is to improve quality and outcomes, while at the same time recognizing and incentivizing participating  cardiology groups and independent cardiologists for their efforts in developing, managing, and improving the quality, efficiency, and effectiveness of the cardiovascular service line (or any component thereof).
cardiology groups and independent cardiologists for their efforts in developing, managing, and improving the quality, efficiency, and effectiveness of the cardiovascular service line (or any component thereof).
The co-management structure
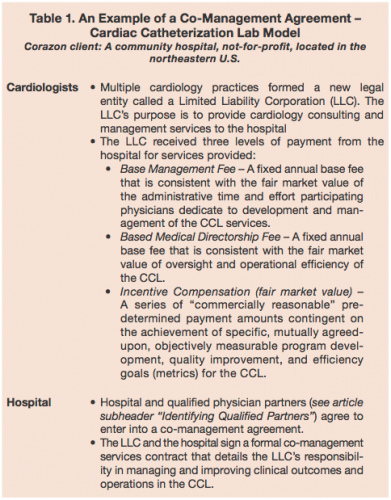
The co-management model (Table 1) has historically helped hospitals and health systems develop collaboration with their physicians. And, when communicated and structured appropriately, this model establishes trust and buy-in from all parties. This more integrated model places physicians and hospital administrators as “partners” in the management and oversight roles for the distinct grouping of services. Often, compensation consists of base fees and bonuses based on achievement of measurable clinical outcomes, patient satisfaction, and operational improvements. Table 1 displays key components of a hospital and cardiology co-management agreement for a cardiac catheterization lab (CCL).
 If hospitals and cardiologists want to compete in the new quality-driven reimbursement environment, a co-management agreement is likely to be a necessary “first step” strategic investment for all parties.
If hospitals and cardiologists want to compete in the new quality-driven reimbursement environment, a co-management agreement is likely to be a necessary “first step” strategic investment for all parties.
Indeed, using the co-management agreement to build a collaborative physician partnership will help hospitals, health systems, and cardiologists prepare for managing the risk associated with pay-for-performance and accountable care initiatives.
Often, expert consultants are used to guide the parties through complexities of drafting the terms of the arrangement, and to assist the hospital and physicians in moving forward with actual model development and formal implementation of the co-management agreement.
Identifying qualified partners
Before entering into a co-management agreement, both the hospital and the physicians need to perform necessary due diligence to validate the potential partnering relationship. In this “partnership exploration phase,” each party compares and clarifies their mission, values, and individual objectives for entering into the agreement; works through any issues or concerns; outlines their individual quality goals; and thoroughly discusses the benefits to each party. In essence, both parties are confirming a “qualified partner” relationship.
Corazon-recommended hospital and physician qualified partner statements
What makes hospitals and physicians “qualified” partners?
- Physicians and the hospital adhere to common values and vision, and avoid conduct that damages one another.
- The hospital and physicians TRUST each other.
- Physicians engage in leadership roles in organization-wide strategic planning and participate in programs to increase hospital efficiency.
- Physicians and the hospital help each other comply with quality and safety standards, and implement best practices.
- Physicians support the venture to the greatest extent possible by being “present” and “active” in all co-management activities.
For the cardiologists, co-management does require them to be present and accountable in order to manage the cath lab and achieve the quality incentive goals. That means: more time spent at the hospital, more time working with the hospital leadership staff, more time working on physician-to-physician relationships, more time engaging in quality improvement activities, and more time sharing and comparing patient outcome data.
To assure the success of the LLC in achieving its goals, co-management physician participation requirements can be developed. These requirements or guidelines provide an additional opportunity to delineate and identify “qualified physician partners.”
Corazon-recommended qualified physician participation requirements in the LLC:
- Physicians are in a position to help the LLC perform its services.
- Possession of active/provisional medical staff membership at the hospital — this should be in good standing.
- Practice in a relevant specialty.
- High-quality standards are demonstrated (i.e., no adverse professional review actions within five years).
- Willingness to participate in meetings/committees as assigned.
Cost to implement
 For the hospital or health system, the cost to implement a co-management agreement is highly variable based on the size and type of the organization, the scope and complexity of the proposed co-management agreement, and the number of estimated qualified physician partners. However, when compared to the costs of other alignment models and/or direct employment, the co-management agreement serves as an excellent “first step” to maximize quality and efficiency.
For the hospital or health system, the cost to implement a co-management agreement is highly variable based on the size and type of the organization, the scope and complexity of the proposed co-management agreement, and the number of estimated qualified physician partners. However, when compared to the costs of other alignment models and/or direct employment, the co-management agreement serves as an excellent “first step” to maximize quality and efficiency.
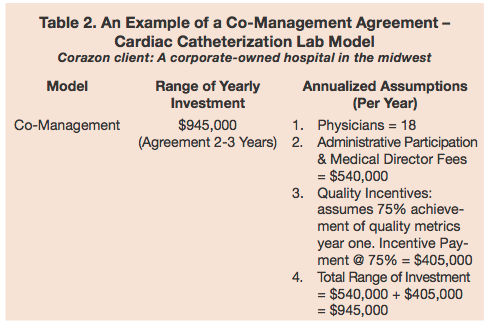
The typical pre-determined payments included in a co-management agreement (Table 2) are:
- Administrative Duties & Medical Director(s): Based on an estimated number of hours necessary to achieve proper management and direction of the service line.
- Quality Bonus Incentive: Based on defined metrics, typically ranging from 8-10 indicators.
Organizations must separately determine the number of hours it takes to manage the service line or a specific department such as the cath lab, for administrative duties and medical directorship(s). The job descriptions and activities must not overlap; therefore, multiple brainstorming sessions with physicians should occur in order to identify specific duties for each and how long it takes to complete such activities. To estimate the cost of administrative duties and medical directorship(s), a fair market hourly rate by physician specialty must be applied to the number of hours agreed upon.
To determine the amount of quality bonus incentive, a rule of thumb for the not-for-profit organization is a capped amount that is no more than the combined amount for administrative duties and medical directors. Organizations must follow IRS Revenue Procedure Code 97-13, which is a safe harbor for management contracts that allows hospitals to pay the LLC a maximum quality bonus payment equal to the administrative and medical directorship duties without having issues related to tax-exempt bond financing space.
Administrative Duties + Medical Directorship(s) = Maximum Quality Bonus Incentive
Quantifiable ROI
Although specific to every organization, improvements in the operations of a co-managed service like the CCL will have a positive impact on both patient care and the hospital’s bottom line that can be realized through the following:
- Improved quality performance
- Standardization of delivery processes
- Supply cost improvements
- Increased market share
For example, improvements in “on-time starts” for cath lab procedures can result in more expedient patient turnover and throughput, as well as improvements in the use of staff time and equipment. In this same example, add-on cases can be more easily accommodated and the process improvements are likely to spread to other units in the hospital.
By reviewing costs and modeling “best practice” in the cardiac cath lab, physician co-managers are able to identify and act on improving other “opportunity costs” (i.e., cost savings), such as pharmaceuticals and supplies.
In addition to cost savings, hospitals and health systems can expect to realize market growth associated with the co-management agreement. As the impetus for quality and efficiency builds, and physician satisfaction grows, more patients are directed to co-managed services, especially from primary care physicians, as they to realize the co-management is having a positive impact on their own clinical outcomes. Likewise, with the advancement of quality and streamlining of services, patient satisfaction and patient self-direction will also contribute to increased market share.
It is also important to remember that insurers will be looking to reward hospital and physician providers who are equally invested in improving patient care, and meeting quality and efficiency goals and objectives.
To co-manage or not to co-manage — “go or no-go” decision points
Industry experts predict that in 2012 physicians will continue to look to hospital employment as a stable option in an unstable environment.1 Trends further suggest that co-management agreements will increase across the country.
However, the co-management model, especially as it relates to cath lab services, must be the right fit for all parties. Throughout all phases of the co-management development, pre-established “go or no-go” decision points must be clearly identified. This is where third-party unbiased advice and/or legal counsel can be of great value, helping both the hospital and physicians identify those decision points while providing support for unanswered clinical, business, and legal questions. A facilitator for this process can also actively assist both parties in overcoming critical roadblocks — something that can be worthwhile in order to maintain momentum. Once all “go, no-go” decision points have been reached and both parties agree to continue, the implementation phase of the co-management agreement can begin.
Implementation of the agreement
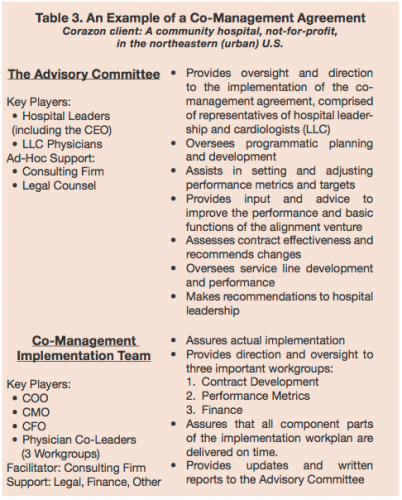 Once plans to move forward have been finalized, the hospital and physicians will need to develop an implementation work plan, set timelines associated with that work plan, and formalize committee and governance structures for the cath lab co-management agreement (Table 3).
Once plans to move forward have been finalized, the hospital and physicians will need to develop an implementation work plan, set timelines associated with that work plan, and formalize committee and governance structures for the cath lab co-management agreement (Table 3).
Performance metrics
No doubt the cardiologists will face a certain degree of financial risk through the use of incentives tied to the clinical performance and the measurement of performance metrics. However, this does translate into an inherent sense of ownership over the service line, which is currently not present in other existing partnering models or with direct employment.
Typically, the performance metrics focus on quality measures, operational efficiency, patient/staff satisfaction, and new program development. Such metrics are then benchmarked against industry standards and incentive payments are applied to each metric. Each metric, benchmark, and payment will need to be deliberated and agreed upon by all parties in the co-management LLC.
It is advisable to engage expert consultants to help model the metrics, structure the incentive fees, and provide recommendations for achieving the specified benchmarks. The consultants can also monitor the operations of the physician LLC to verify and validate that the goals related to the metrics have been achieved, which entitles the LLC to incentive payments.
Secure ongoing legal oversight and valuation firm
Because the co-management agreement involves payments between the hospital and cardiologists, the co-management agreement must be regularly evaluated for potential abuse under applicable healthcare statutes and regulations, and will be subject to external legal scrutiny.
Finally, an independent third-party valuation firm experienced in providing healthcare services should review all compensation for estimated duties and hours, as well as quality indictors, to confirm that the proposed agreement reflects fair market value and commercial reasonableness.
Conclusion — reaching the ultimate customer
The co-management agreement allows a hospital and/or health system to provide financial incentives for cardiologists on the allied medical staff in assisting the hospital with quality improvement and cost of care reductions.
In general, a co-management agreement can be a viable alternative to the direct employment of cardiologists for those hospitals and health systems that do not want to assume the administrative or financial responsibility of owning and operating cardiology practices, and for cardiologists who wish to remain independent rather than become direct employees.
Because a cath lab co-management agreement involves the payment of compensation to physicians who refer patients to the hospital or health system, the agreement must be properly structured in order to avoid any violation of healthcare statute and/or regulation.
Hospitals and health systems interested in developing and implementing a co-management agreement with their cardiologists should act now to initiate discussions — this is a ‘hot’ issue for hospitals AND physicians as both try to improve their quality of care, positive community reputation, overall market performance, and financial viability.
Through Corazon experience across the country, the co-management agreement has proven itself to be a highly viable partnering and alignment model for hospitals and cardiologists. And, perhaps most importantly, the benefits inherent in the co-management agreement extend to the patient, the ultimate healthcare customer, who will receive higher quality, more efficient and effective care and treatment.
Bruce is a director and Kristin is a lead business consultant with Corazon, offering program solutions for the heart, vascular, neuro, and ortho specialties. The team provides consulting, recruitment, interim management, and physician practice and alignment services (PP&A) across the country and in Canada. To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach the authors, email bpayton@corazoninc.com or ktruesdell@corazoninc.com.
Reference
- The Camden Group. 2012 healthcare industry outlook: capital and cost pressures persist, triggering more consolidation. January 5, 2012. Available online at https://www.thecamdengroup.com/press/Camden_2012_Trends_Release.pdf. Accessed March 19, 2012.
