


Change is Looming on the Horizon for Angioplasty Programs… A Primer to the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention
 As the cardiovascular industry matures, more and more hospitals have entered the arena of therapeutic catheter services, complementing the diagnostic capabilities that many already offer. Corazon frequently supports hospitals with the implementation or advancement of percutaneous coronary intervention (PCI) services. Perhaps the most important guidelines document incorporated to assist our team and clients is the American College of Cardiology Foundation/American Heart Association/Society for Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) Guideline for Percutaneous Coronary Intervention.1
As the cardiovascular industry matures, more and more hospitals have entered the arena of therapeutic catheter services, complementing the diagnostic capabilities that many already offer. Corazon frequently supports hospitals with the implementation or advancement of percutaneous coronary intervention (PCI) services. Perhaps the most important guidelines document incorporated to assist our team and clients is the American College of Cardiology Foundation/American Heart Association/Society for Cardiovascular Angiography and Interventions (ACCF/AHA/SCAI) Guideline for Percutaneous Coronary Intervention.1
Practice guidelines have been developed through the collaboration of a writing committee made up of esteemed cardiologists throughout the United States. Their intent is to produce practice guidelines within the overarching document to assist physicians in selecting the best management strategies for an individual patient. The PCI guidelines are developed in an approach that allows physicians to decide among multitudes of generally acceptable approaches for the clinical management of cardiovascular conditions. In rare cases, an individual clinical situation could warrant deviation from the guidelines. The Corazon team, made up of both physician medical advisors and non-physician clinical consultants, utilizes these guidelines not only as clinical management tools, but for programmatic development of best practice as well. These programmatic considerations may include performance measures, quality improvement processes, and clinical decision support tools.
A Brief History
The ACCF and the AHA have been producing guidelines in the management of cardiovascular disease since 1980. In 1982, the first manuscript was published in Circulation, entitled “Guidelines for the Performance of Percutaneous Transluminal Coronary Angioplasty.” PCI remained in its infancy during this time and the manuscript was only two pages. In 1988, the first ACC/AHA Task Force report on guidelines for coronary angioplasty was published. The expanded content of this report included lesion classification, success rates, indications for and contraindications to balloon angioplasty, and several operational parameters such as on-site surgical back up.
Additional revisions and expansion to the PCI guideline were published in 1993, 2001, and 2005. With each addition, the guideline has become more widely accepted in the field of cardiovascular disease. It encompasses “best practice” treatment protocols through the collation of the most relevant research findings to specify classes of treatment recommendations. Recommendations that are considered Class I have been proven to represent optimal medical therapy. Class I recommendations have a benefit that is much more substantial than the risk and this level of recommendation means the procedure/treatment SHOULD be performed. Class IIa indications still demonstrate a benefit that is greater than the risk, though the evidence is not as strong as a Class I recommendation. Class IIa indications are REASONABLE to perform. Class IIb recommendations produce a benefit that is greater than or equal to the risk. Class IIb recommendations provide treatment options that MAY BE CONSIDERED. Finally, Class III recommendations are reserved for those indications that may produce no benefit or may, in fact, be harmful. These classifications can be extremely useful in evaluating best practice treatment algorithms related to any PCI program.
In 2007 and 2009, more narrowly focused updates to the guidelines were published to address changes in PCI, published quickly due to the expeditious conclusion of several research trials. The 2009 update was the first time that the ST-elevation myocardial infarction (STEMI) guidelines and the PCI guidelines were placed into a single publication through the collaboration of both those writing committees. The latest full revision to the PCI guideline was released in November 2011, and it includes some of the most ‘programmatic’ implications that we have seen to date. Herein, we will detail some of the guideline areas that we believe will have the most impact on cardiovascular programs.
Programmatic Implication #1: Approach to Patient Selection
Individual patient appropriateness for the PCI procedure has been under recent scrutiny. Our team is continually assisting programs that are evaluating the treatment decisions of the cardiologist(s), and often, PCI is the procedure under the most scrutiny. The 2011 PCI guidelines provide a great deal of information related to the “heart team approach” to revascularization decisions. This approach is recommended in patients with unprotected left main or complex coronary artery disease (CAD).1 The guidelines clearly state that it is best if the treatment approach for the complex patient is discussed with both the interventional cardiologist as well as the cardiac surgeon. It is still common, however, to find programs in which the interventional cardiologist is the sole decision-maker for all patients, regardless of risk.
The guidelines also detail clinical tools to complement the decision-making of the heart team concept discussed above. Calculation of Society of Thoracic Surgeons (STS) and SYNTAX scores is reasonable in the same high-risk patient population described above. The SYNTAX study (Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery) is the current most comprehensive comparison of PCI with coronary artery bypass graft surgery (CABG).5 It is not within the scope of this article to detail the SYNTAX scoring system; however, cath lab clinicians should recognize that patients with a lower SYNTAX score (≤ 22) have a higher likelihood of a good long-term outcome with a less invasive treatment such as PCI, when coupled with increased risk of adverse surgical outcomes, as per the STS predicted risk of operative mortality score.
One area fraught with controversy, left main CAD revascularization, is also addressed in the most recent guideline. CABG to improve survival is recommended in those patients with a ≥ 50% diameter stenosis (considered significant for left main disease) as a Class I indication. PCI can be used for significant left main stenosis, if the heart team agrees that there is a low risk of percutaneous-related procedure complications. Again, the low risk of complications can be validated through the use of SYNTAX and STS scores. PCI in this setting has been given a Class IIa indication.1
In complex patients such as those with left main disease or for a ≥ 70% stenosis in the non-left main coronaries, the 2011 guideline also endorses an approach where the procedure may be immediately terminated after diagnostic catheterization. The ensuing time interval will allow the cardiologist(s) and cardiac surgeon an opportunity to thoroughly discuss treatment options for the complex patient. (It will be interesting to see whether cardiac programs throughout the U.S. experience more “staging” of complex PCI procedures over time as a result of the guidelines.) If there is an interest in other patient types that are not as complex, such as intermediate lesion morphology (stenosis of 50-70% in the non-left main), a deeper analysis of the guidelines is recommended. There exists a wealth of information and indications for patients with less critical lesion types.
Programmatic Implication #2: Hybrid Coronary Revascularization
The concept of performing both a planned coronary artery bypass procedure in combination with a PCI appears to be on the radar of many clinicians. The 2011 PCI guideline clearly defines hybrid coronary revascularization as the combination of left internal mammary artery (LIMA)-to-left anterior descending (LAD) artery grafting and PCI of ≥ 1 non-LAD coronary atery.1 This combined procedural approach has been designated a class IIa indication for patients that have (1) limitations to traditional CABG, such as a heavily calcified aorta or poor target vessels for CABG; (2) Lack of suitable graft conduits, and (3) unfavorable LAD artery for PCI.
Hybrid coronary revascularization procedures profoundly impact even the most experienced cardiovascular programs. The procedure may be performed in a hybrid suite (if available) in one setting or as a staged procedure. “Staged” indicates that the PCI and CABG were performed separately by hours or perhaps days, although the hybrid approach infers that both procedures are performed within the same hospital stay. If a staged procedure is performed, commonly due to lack of a hybrid suite or patient clinical factors, then it is preferred to perform CABG prior to PCI. The order of this approach will allow the interventional cardiologist to verify the patency of the CABG conduit before attempting PCI of other vessels and minimize the risk of perioperative bleeding that could occur if CABG were performed after PCI.
Programmatic Implication #3: PCI in Hospitals Without On-Site Surgical Backup
Whether your facility already provides PCI or you have a diagnostic catheterization service, there has been a great surge of interest in those programs currently offering or possessing the capability to perform PCI without having cardiac surgery on site. Over the last decade, the need to mechanically open occluded coronary arteries in the presence of STEMI has been well understood. The current PCI guideline provides a dramatic shift in the level of indications for performing PCI procedures at facilities without surgery on site (SOS). Regardless of distance from current PCI centers, our team supports the notion that the initiation of PCI programs without SOS should be focused on those facilities unable to provide timely PCI services in the local marketplace.
Perhaps the greatest impact of the current 2011 guideline revisions relates to the shifting of PCI without SOS to higher classifications that appear to further support the practice. Primary PCI (PCI in the presence of a STEMI) was considered a class IIb indication prior to the most recent guidelines. The current PCI guideline has elevated primary PCI to a class IIa indication. Primary PCI is considered reasonable in hospitals without cardiac surgery, provided that the appropriate planning for program development has been accomplished. It was also significant that the current guideline has elevated the status of elective PCI, as this has been one of the greatest sources of controversy for programs without on-site surgical backup. Elective PCI may be considered in hospitals without on-site cardiac surgery, provided that appropriate planning has been accomplished and rigorous clinical and angiographic selection criteria are used for patient selection. Elective PCI has been moved from a class III status (harmful) to a class IIa in the current guideline. There are very prescriptive measures for elective PCI without SOS related to patient risk, lesion risk, and a strategy for surgical backup, all detailed in the latest practice guideline.
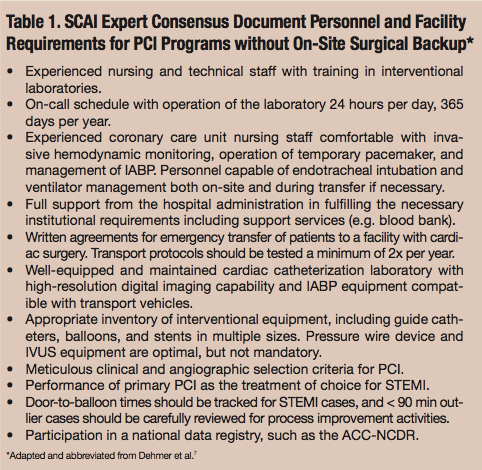 Programs considering the offering of PCI without on-site surgical back up must employ rigorous implementation parameters. It is still considered a class III indication to offer PCI without SOS without having a proven plan for rapid transport to a cardiac surgery operating room in a nearby hospital or without appropriate hemodynamic support capability for transfer.1 An abbreviated list of facility requirements for programs wishing to perform PCI without on-site surgical backup from the SCAI Expert Consensus Document is detailed in Table 1. It should also be noted that often the largest barrier for programs attempting to gain entry into PCI services is individual state regulations. Corazon is anticipating that with the release of the new 2011 PCI guideline, states that have practices prohibitive to the offering of PCI will begin to relax their requirements.
Programs considering the offering of PCI without on-site surgical back up must employ rigorous implementation parameters. It is still considered a class III indication to offer PCI without SOS without having a proven plan for rapid transport to a cardiac surgery operating room in a nearby hospital or without appropriate hemodynamic support capability for transfer.1 An abbreviated list of facility requirements for programs wishing to perform PCI without on-site surgical backup from the SCAI Expert Consensus Document is detailed in Table 1. It should also be noted that often the largest barrier for programs attempting to gain entry into PCI services is individual state regulations. Corazon is anticipating that with the release of the new 2011 PCI guideline, states that have practices prohibitive to the offering of PCI will begin to relax their requirements.
Programmatic Implication #4: Adjunctive Diagnostic Devices
Facilities are attempting to utilize scientifically proven techniques to ensure appropriate intervention. The level of scrutiny related to the performance of PCI in appropriate patients has reached a high magnitude. All facilities performing PCI would be wise to invest in devices that assist in the determination of lesions that are appropriate for and amenable to treatment. The new 2011 PCI guideline has greatly expanded the language related to adjunctive devices for this purpose.
Fractional flow reserve (FFR) is a physiologic measurement that can be made with flow-wire technology to assist with the assessment related to level of obstruction for a lesion. FFR has been granted a status IIa indication in the current revision. FFR is reasonable to assess angiographic intermediate coronary lesions (50% to 70% diameter stenosis) and can be useful in patient appropriateness decisions for those with stable ischemic disease.1 The correlation of ischemia on stress testing with FFR values of <0.75 has been established in numerous comparative studies with high sensitivity and specificity. FFR appears to be gaining traction at our client sites in comparison to intravascular ultrasound (IVUS). It is noted that both FFR and IVUS have shown favorable outcomes related to intermediate angiographic (as defined above) lesion assessment, though FFR may reduce the need for revascularization. IVUS utilization is a class IIa indication for the assessment of angiographically indeterminant left main CAD and a class IIb indication for the assessment of non-left main coronary arteries with angiographically intermediate coronary stenoses.1
Of note, optical coherence tomography (OCT) has not received any clinical indication within the 2011 guideline, because the appropriate role of OCT within routine clinical decision-making has not yet been established. However, the guideline does specify that OCT provides excellent resolution for 2-dimensional imaging of plaque morphology and evaluation of response to stent implantation. Further research related to the role of OCT within the PCI treatment is needed.
Programmatic Implication #5: Adjunctive Therapeutic Devices
The 2011 guideline has expanded upon its prior recommendations related to devices that many programs have been debating for purchase or further use. For simplicity, the technological device and the clinical indication per the guideline have been summarized in the list below:
- Rotational atherectomy – Class IIa, for fibrotic or heavily calcified lesions that cannot be crossed or dilated with conventional balloon angioplasty. Class III, for de novo lesions or in-stent restenosis.
- Aspiration thrombectomy – Class IIa, for patients undergoing primary PCI.
- Laser angioplasty – Class IIb, considered for fibrotic or moderately calcified lesions that cannot be crossed or dilated with conventional balloon angioplasty. Class III, for routine PCI.
- Cutting balloon angioplasty – Class IIb, to avoid slippage-induced coronary artery trauma during PCI for in-stent restenosis or ostial lesions in side branches. Class III, for routine PCI.
- Embolic protection devices – Class I, for saphenous vein graft PCI when feasible.
- Percutaneous hemodynamic support (inclusive of IABP counterpulsation, Impella Recover LP 2.5 System [Abiomed], and TandemHeart [CardiacAssist, Inc.]) – Class IIb: elective insertion of an appropriate hemodynamic support device as an adjunct to PCI may be reasonable in carefully selected high-risk patients.1 High-risk patients include those undergoing unprotected left main or last remaining conduit PCI, those with severely depressed ejection fraction (EF) undergoing PCI of a vessel supplying a large territory, and those patients in pronounced cardiogenic shock.
Concluding Remarks
The 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention has been the most comprehensive revision to the PCI guidelines to date. There are several very important aspects to the guideline that have not been covered in this manuscript. For example, pharmaceutical treatment options are very detailed in this last revision and likely require their own summation. The guideline also covers quality and performance considerations such as operator and institutional volumes, though these do not appear to be significantly different from the prior revisions and the focused updates. Herein, we have attempted to capture the most global items added or expanded within the guideline that will likely have an overall program impact. Consider how your program’s clinical decision-making or employed technologies will change as a result of the recommendations of the 2011 PCI guideline. A proactive look ahead may help your program avoid surprises and continue to deliver excellence in cardiac care.
Ross Swanson is a Vice President at Corazon, Inc., offering consulting, recruitment, and interim management services for the heart, vascular, neuro, and ortho specialties. To learn more, call (412) 364-8200 or visit www.corazoninc.com. To reach Ross, email rswanson@corazoninc.com.
References
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation /American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011 Dec 6;58(24):e44-e122.
- Williams DO, Gruntziz A, Kent KM, et al. Guidelines for the performance of transluminal coronary angioplasty. Circulation 1982; 66:693-694.
- Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therepeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). J Am Coll Cardiol 1988:12:529-545.
- Kushner FG, Hand M, Smith SC Jr, et al. 2009 Focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update). J Am Coll Cardiol 2009; 54:2205-2241.
- Chakravarty T, Buch MH, Naik H, et al. Predictive accuracy of SYNTAX score for predicting long-term outcomes of unprotected left main coronary artery revascularization. Am J Cardiol 2011; 107:360-366.
- Gilard M, Bezon E, Cornily JC, et al. Same-day combined percutaneous coronary intervention and coronary artery surgery. Cardiology 2007;108:363-367.
- Dehmer GJ, Blankenship J, Wharton TP Jr., et al. The current status and future direction of percutaneous coronary intervention without on-site surgical back-up: an expert consensus document from the Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv 2007; 69:471-478.
- Sing PP, Sing M, Bedi US, et al. Outcomes of nonemergent percutaneous coronary intervention with and without on-site surgical backup: a meta-analysis. Am J Ther 2011:18:e22-e28.
- Kern MJ, Samady H. Current concepts of integrated coronary physiology in the catheterization laboratory. J Am Coll Cardiol 2010; 55:173-185.
- Nam CW, Yoon HF, Cho YK, et al. Outcomes of percutaneous coronary intervention in intermediate coronary disease: fractional flow reserve-guided versus intravascular ultrasound-guided. J Am Coll Cardiol Intv 2010;3:812-817.
