


Central Venous Access During Transradial Approach
Question: What do you do when the case calls for venous access as well as arterial access? Are you just going through the groin?
Good question. Every operator is different in what they feel comfortable with. Some will continue to access the femoral vein or the internal jugular. Our default approach is from the ipsilateral antecubital vein as the radial access. Following is a case example using venous access for a transvenous pacer in a patient with an acute inferior wall myocardial infarction (MI).
Case report
An 84-year-old female with a history of hypertension, diabetes, and dyslipidemia presented to the emergency department with approximately one hour of chest pain and dizziness. Initial electrocardiogram (EKG) demonstrated ST elevations with complete heart block (Figure 1). She was brought to the lab for emergent cardiac catheterization. Diagnostic angiography and percutaneous coronary intervention (PCI) were performed via the right radial artery. A transvenous pacemaker was inserted from the right antecubital vein.
the emergency department with approximately one hour of chest pain and dizziness. Initial electrocardiogram (EKG) demonstrated ST elevations with complete heart block (Figure 1). She was brought to the lab for emergent cardiac catheterization. Diagnostic angiography and percutaneous coronary intervention (PCI) were performed via the right radial artery. A transvenous pacemaker was inserted from the right antecubital vein.
The right radial artery was prepped and draped in sterile fashion, then accessed with a 6 French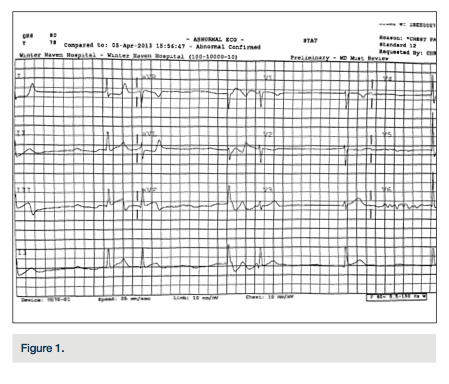 (Fr) Glidesheath (Terumo). The right antecubital vein was accessed by the nurse prior to the patient’s arrival to the lab and changed (after sterile prep followed by betadine solution) to a 5 Fr Glidesheath (Figure 2). The transvenous pacemaker was advanced into the right ventricle (Figure 3). Following placement of the pacemaker and capture, a Judkins right (JR) 4 6 Fr guide was used to engage the right coronary artery. Angiography demonstrated a proximal right coronary artery occlusion with TIMI-0 flow (Figure 4). After administration of bivalirudin (Angiomax, The Medicines Company), a Runthrough wire (Terumo) was passed distally. A 1.0 x 10 mm ClearWay balloon (Atrium Medical) was advanced to the lesion and intracoronary abciximab (ReoPro, Eli Lilly & Co.) was administered. Following drug
(Fr) Glidesheath (Terumo). The right antecubital vein was accessed by the nurse prior to the patient’s arrival to the lab and changed (after sterile prep followed by betadine solution) to a 5 Fr Glidesheath (Figure 2). The transvenous pacemaker was advanced into the right ventricle (Figure 3). Following placement of the pacemaker and capture, a Judkins right (JR) 4 6 Fr guide was used to engage the right coronary artery. Angiography demonstrated a proximal right coronary artery occlusion with TIMI-0 flow (Figure 4). After administration of bivalirudin (Angiomax, The Medicines Company), a Runthrough wire (Terumo) was passed distally. A 1.0 x 10 mm ClearWay balloon (Atrium Medical) was advanced to the lesion and intracoronary abciximab (ReoPro, Eli Lilly & Co.) was administered. Following drug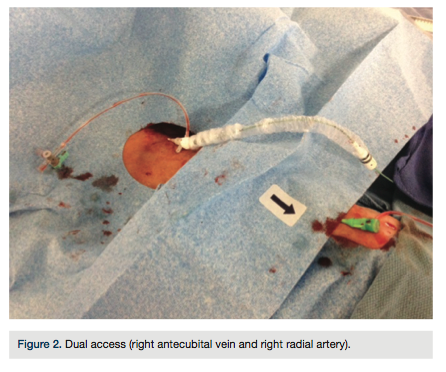 administration, there was improved flow and evidence of a more focal obstruction (Figure 5). A 3.0 x 15 mm Integrity bare metal stent (Medtronic) was deployed at 11 atm with no angiographic residual stenosis and restoration of TIMI-3 flow (Figure 6). Following revascularization of the right coronary artery, the guide was advanced into the left ventricle to calculate the left ventricular end diastolic pressure (LVEDP) and perform ventriculography (estimated ejection fraction was 55% with mild inferobasal hypokinesis noted on hand injection. No significant transvalvular gradient was noted on pull-back). A diagnostic Judkins left (JL) 3.5 catheter was then used to engage the left coronary system. Angiography revealed a 90%
administration, there was improved flow and evidence of a more focal obstruction (Figure 5). A 3.0 x 15 mm Integrity bare metal stent (Medtronic) was deployed at 11 atm with no angiographic residual stenosis and restoration of TIMI-3 flow (Figure 6). Following revascularization of the right coronary artery, the guide was advanced into the left ventricle to calculate the left ventricular end diastolic pressure (LVEDP) and perform ventriculography (estimated ejection fraction was 55% with mild inferobasal hypokinesis noted on hand injection. No significant transvalvular gradient was noted on pull-back). A diagnostic Judkins left (JL) 3.5 catheter was then used to engage the left coronary system. Angiography revealed a 90%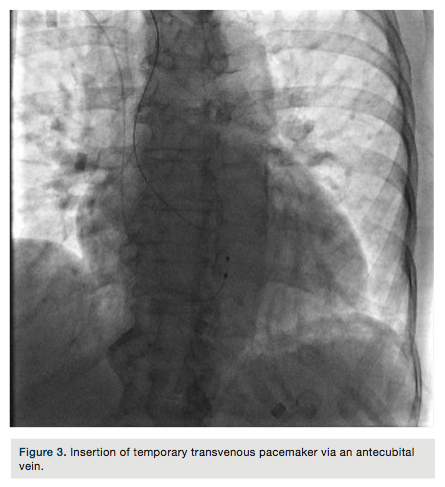 proximal left anterior descending coronary artery (LAD) stenosis and intermediate disease of the circumflex (Figure 7). The patient was started on ticagrelor (Brilinta, AstraZeneca) and aspirin, and transferred to the unit. The pacemaker was removed after the patient regained sinus rhythm. She was discharged home after 48 hours with plans for staged intervention of the LAD.
proximal left anterior descending coronary artery (LAD) stenosis and intermediate disease of the circumflex (Figure 7). The patient was started on ticagrelor (Brilinta, AstraZeneca) and aspirin, and transferred to the unit. The pacemaker was removed after the patient regained sinus rhythm. She was discharged home after 48 hours with plans for staged intervention of the LAD.
Discussion
This case demonstrates the ability to access the right heart from the forearm, thereby extending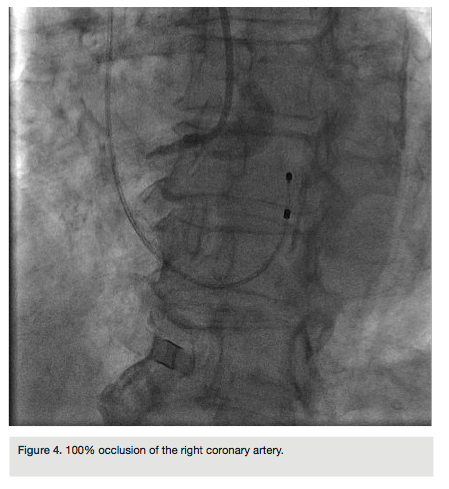 benefits of the transradial approach. Such an approach may be particularily beneficial in certain subsets of patients such as those that have received thrombolytics, are on anticoagulation, are morbidly obese, or have inferior vena cava (IVC) hardware or interruption. Utilization of this approach is conditional upon obtaining venous access. For elective procedures, the nursing staff will routinely obtain access prior to the procedure, and then the site is prepped in a sterile manner and the IV is exchanged for a Glidesheath. Ultrasound can also be used to obtain access; however, this could prove time consuming.Alternative approaches include using levophase contrast venography1 to visualize the vein, followed by direct puncture
benefits of the transradial approach. Such an approach may be particularily beneficial in certain subsets of patients such as those that have received thrombolytics, are on anticoagulation, are morbidly obese, or have inferior vena cava (IVC) hardware or interruption. Utilization of this approach is conditional upon obtaining venous access. For elective procedures, the nursing staff will routinely obtain access prior to the procedure, and then the site is prepped in a sterile manner and the IV is exchanged for a Glidesheath. Ultrasound can also be used to obtain access; however, this could prove time consuming.Alternative approaches include using levophase contrast venography1 to visualize the vein, followed by direct puncture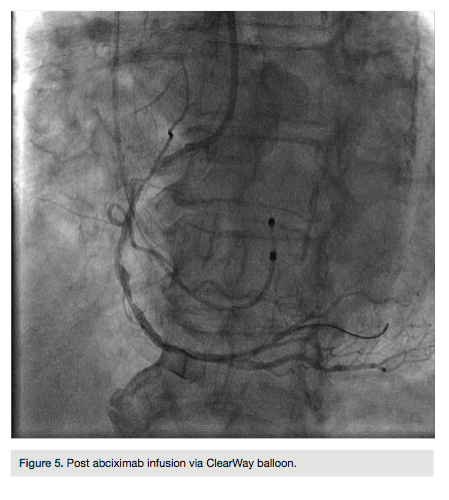 or injection of contrast via a small distal peripheral vein, followed by access.
or injection of contrast via a small distal peripheral vein, followed by access.
One should familiarize themselves with venous anatomy of the upper extremity and its variations to help navigate the catheter. When obtaining central venous access from the forearm, use a long Swan-Ganz catheter (110 cm, DeRoyal Industries). Advance the catheter with either flush going through the distal port (“open” the vein ahead of the catheter) or advance the catheter over a coronary wire. Once in the subclavian, the balloon can usually be inflated and catheter advancement can continue.
This procedure has been previously described in the literature2,3 and has demonstrated to have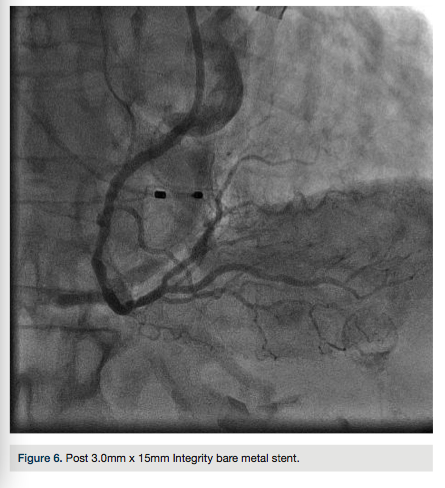 fewer access site complications and earlier ambulation when compared to the traditional femoral approach.4 If antecubital access is not easily obtained, then consider using levophase contrast venography to visualize the deep forearm veins. This approach may not be obtainable in all patients, but should be considered. Hemostasis can be effectively achieved despite anticoagulation5 and the patient will receive the extended benefits of a transradial approach.
fewer access site complications and earlier ambulation when compared to the traditional femoral approach.4 If antecubital access is not easily obtained, then consider using levophase contrast venography to visualize the deep forearm veins. This approach may not be obtainable in all patients, but should be considered. Hemostasis can be effectively achieved despite anticoagulation5 and the patient will receive the extended benefits of a transradial approach.
Disclosure: Orlando Marrero reports no conflicts of interest regarding the content herein. Dr. Zaheed Tai reports the following: Terumo (proctor for transradial course), Spectranetics (proctor for laser course, speaker, advisory board), Medicines Company (speakers bureau).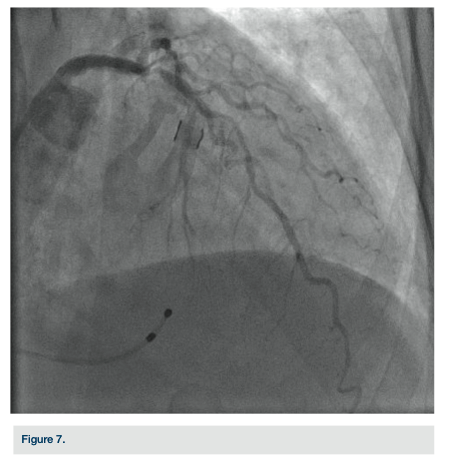
Orlando Marrero can be contacted at orlm8597@yahoo.com. Dr. Zaheed Tai can be contacted at zaheedtai@gmail.com.
References
- Pancholy S, Sweeney J. A technique to access difficult to find upper extremity veins for right heart catheterization: the levogram technique. Catheter Cardiovasc Interv. 2011; 78: 809-812.
- Gilchrist IC, Kharabsheh S, Nickolaus MJ, Reddy R. Radial approach to right heart catheterization: Early experience with a promising technique. Catheter Cardiovasc Interv 2002; 55: 20–22.
- Yang CH, Guo GB, Yip HK, Hsieh K, Fang CY, Chen SM, Cheng CI, Hang CL, Chen MC, Wu CJ. Bilateral cardiac catheterizations: The safety and feasibility of a superficial forearm venous and transradial arterial approach. Int Heart J. 2006; 47: 21-27.
- Gilchrist IC, Moyer CD, Gascho JA. Transradial right and left heart catheterizations: a comparison to traditional femoral approach. Catheter Cardiovasc Interv 2006; 67: 585–588.
- Lo TS, Buch AN, Hall IR, Hildick-Smith DJ, Nolan J. Percutaneous left and right heart catheterization in fully anticoagulated patients utilizing the radial artery and forearm vein: a two-center experience. J Interv Cardiol. 2006; 19: 258-263.
