


Catheter-Directed Intracoronary Fibrinolysis for Subacute Stent Thrombosis After Failure of Conventional Treatment Strategies
Abstract
Primary percutaneous coronary intervention (PCI) is the preferred strategy for reperfusion in the treatment of acute myocardial infarction due to superior outcomes compared to fibrinolytic therapy. However, various adjunctive strategies, referred to as facilitated PCI, have been explored to further improve outcomes. We present a case of acute myocardial infarction with stent thrombosis that failed conventional treatment strategies, but managed successfully with catheter-directed intracoronary fibrinolysis.
Case
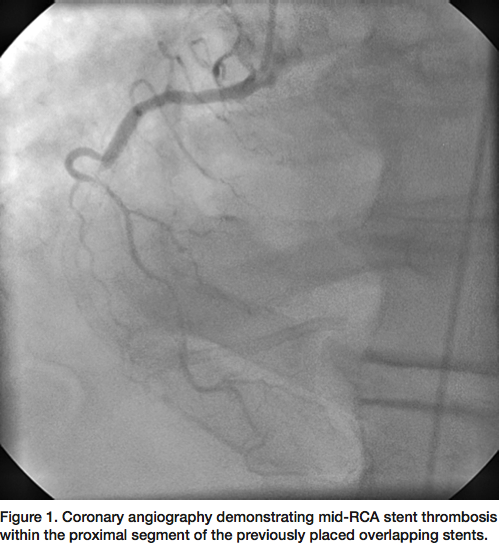 A 58-year-old male with known coronary artery disease and prior PCI of the right coronary artery (RCA) with multiple overlapping drug-eluting stents, presented with acute ST-segment elevation myocardial infarction (STEMI). Physical examination was unremarkable and laboratory analysis confirmed recent MI with troponin of 1.14. Electrocardiogram revealed acute ST-segment elevations in the inferior leads and reciprocal changes in the anterior leads. Coronary angiography revealed mid RCA stent thrombosis within the proximal segment of the previously placed stents (Figure 1).
A 58-year-old male with known coronary artery disease and prior PCI of the right coronary artery (RCA) with multiple overlapping drug-eluting stents, presented with acute ST-segment elevation myocardial infarction (STEMI). Physical examination was unremarkable and laboratory analysis confirmed recent MI with troponin of 1.14. Electrocardiogram revealed acute ST-segment elevations in the inferior leads and reciprocal changes in the anterior leads. Coronary angiography revealed mid RCA stent thrombosis within the proximal segment of the previously placed stents (Figure 1).
 A 6 French JR4 guide was used to engage the RCA. A Prowater wire (Asahi Intecc) was initially advanced but unable to cross the lesion. A PT Graphix wire (Boston Scientific) was then advanced with the use of an Apex 1.5 mm over-the-wire balloon (Boston Scientific) for support to cross the occluded segment into the distal RCA. Due to the degree of thrombus burden, laser atherectomy was performed (Figure 2) using a 0.9 mm ELCA catheter (Spectranetics) with no improvement in flow. Intravascular ultrasound (IVUS) of the entire stented
A 6 French JR4 guide was used to engage the RCA. A Prowater wire (Asahi Intecc) was initially advanced but unable to cross the lesion. A PT Graphix wire (Boston Scientific) was then advanced with the use of an Apex 1.5 mm over-the-wire balloon (Boston Scientific) for support to cross the occluded segment into the distal RCA. Due to the degree of thrombus burden, laser atherectomy was performed (Figure 2) using a 0.9 mm ELCA catheter (Spectranetics) with no improvement in flow. Intravascular ultrasound (IVUS) of the entire stented 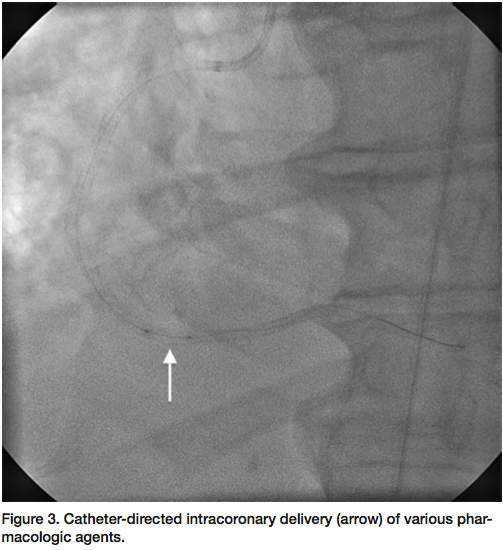 segment revealed an under-expanded stent with a reference vessel size of 4 mm. An NC Sprinter 4.0 mm balloon (Medtronic) was used to further dilate the stented segment, but with no improvement in flow. A ClearWay 1.0 x 10 mm perfusion balloon (Atrium) was then used to deliver intracoronary nitroglycerin, adenosine, and eptifibatide (Figure 3), with still no distal flow. Finally, the ClearWay balloon was used to deliver intracoronary tPA (2 mg bolus) with significant improvement in flow after 5 minutes of dwell time. Final angiogram revealed brisk TIMI-3 flow through the stented segment with excellent angiographic result (Figure 4).
segment revealed an under-expanded stent with a reference vessel size of 4 mm. An NC Sprinter 4.0 mm balloon (Medtronic) was used to further dilate the stented segment, but with no improvement in flow. A ClearWay 1.0 x 10 mm perfusion balloon (Atrium) was then used to deliver intracoronary nitroglycerin, adenosine, and eptifibatide (Figure 3), with still no distal flow. Finally, the ClearWay balloon was used to deliver intracoronary tPA (2 mg bolus) with significant improvement in flow after 5 minutes of dwell time. Final angiogram revealed brisk TIMI-3 flow through the stented segment with excellent angiographic result (Figure 4).
 The remainder of the hospital stay was uncomplicated and the patient was discharged home the following day with dual antiplatelet therapy including aspirin and prasugrel indefinitely.
The remainder of the hospital stay was uncomplicated and the patient was discharged home the following day with dual antiplatelet therapy including aspirin and prasugrel indefinitely.
Discussion
Early and complete reperfusion is the most important goal in treatment of patients with acute STEMI.1 Primary PCI is the preferred strategy for reperfusion in the treatment of STEMI, due to superior outcomes compared to fibrinolytic therapy.2
The optimal pharmacologic therapy for reperfusion before and in conjunction with primary PCI has evolved over time. Facilitated percutaneous coronary intervention (FPCI), utilizing PCI preceded by early treatment with glycoprotein IIb/IIIa inhibitors or fibrinolytics, has been previously evaluated as a potential strategy to improve outcomes in patients with acute STEMI.3 However, results of FPCI have been variable, based on pharmacologic agent and timing of use, and therefore, inconclusive. While significantly more patients had early ST-segment resolution with FPCI using fibrinolytics and glycoprotein IIb/IIIa inhibitors, the primary endpoint composite of all-cause mortality, ventricular fibrillation, cardiogenic shock, and congestive heart failure was similar in all groups.3 More recently, FPCI with intracoronary catheter-directed delivery of glycoprotein IIb/IIIa inhibitor has been shown to reduce infarct-size in patients with large anterior STEMI4, suggesting a benefit of localized high-dose delivery of the adjunctive pharmacologic agent. FPCI with catheter-directed fibrinolysis in the setting of acute MI may be a viable strategy that demands further evaluation.
Herein, we present a patient with acute stent thrombosis refractory to conventional treatment strategies that was successfully revascularized after catheter-directed intracoronary delivery of fibrinolytics.
References
- Simes RJ, Topol EJ, Holmes DR Jr, et al. Link between the angiographic substudy and mortality outcomes in a large randomized trial of myocardial reperfusion: importance of early and complete infarct artery reperfusion. Circulation 1995; 91: 1923-1928.
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003; 361: 13-20.
Ellis SG, Tendera M, deBelder MA, et al. Facilitated PCI in patients with ST-elevation myocardial infarction. N Engl J Med 2008; 358: 2205-2217. - Stone GW, Maehara A, Witzenbichler B, et al. Intracoronary abciximab and aspiration thrombectomy in patients with large anterior myocardial infarction: the INFUSE-AMI randomized trial. JAMA 2012; 307(17): 1817-1826.
________________________________
Dr. Jon George may be contacted at georgej@deborah.org. Disclosure: Dr. George reports he is a consultant for Boston Scientific and Spectranetics, and receives research support from Atrium Medical.
