


Cath Lab Spotlight: Metro Health Hospital Cardiovascular Lab
Dr. Jihad Mustapha can be contacted at Jihad.Mustapha@metrogr.org.
Tell us about your cath lab.
Metro Health Hospital is a 208-bed, community-based teaching hospital located in Wyoming, Michigan. The cardiovascular laboratory consists of two cardiovascular labs (with plans to open a third in the near future) and one interventional radiology lab. We have 26 staff, including 18 registered nurses (RNs) and eight registered radiology technologists (RT[R]s). Staff longevity ranges from one to over 30 years. Additionally, three vascular technologists and eight clinical research nurses rotate through our lab on a regular basis.
Michigan. The cardiovascular laboratory consists of two cardiovascular labs (with plans to open a third in the near future) and one interventional radiology lab. We have 26 staff, including 18 registered nurses (RNs) and eight registered radiology technologists (RT[R]s). Staff longevity ranges from one to over 30 years. Additionally, three vascular technologists and eight clinical research nurses rotate through our lab on a regular basis.
What procedures are performed in your cath lab?
Currently our cath lab performs transesophageal echocardiograms (TEEs), tilt tables, cardioversions, and some loop recorder implants in the holding area. Right and left heart catheterizations, device implants, pericardiocentesis, and emergent percutaneous coronary intervention (PCI) are performed in the cardiovascular labs. Additionally, we perform approximately 100 peripheral vascular angiograms and interventions (PVI) each month.
Who manages your cath lab?
Philip Pascucci, an RN with 12 years of experience in the emergency department and 11 years of cardiovascular experience.
of cardiovascular experience.
What are some of the new equipment, devices and products recently introduced at your lab?
The first retrograde pedal access case utilizing the new 60 cm Diamondback orbital atherectomy device (Cardiovascular Systems, Inc.) was performed in our lab in March of this year and received local media attention.
Indigo System (Penumbra), a percutaneous mechanical thrombectomy device, was historically used for neurovascular cases. It has recently been used in our lab during peripheral vascular interventions.
Do any of your physicians regularly gain access via the radial artery?
Yes, our physicians perform radial access primarily for cardiac catheterizations and interventions (40-45% of cases), as well as for diagnostic aorto-iliac runoff angiograms and iliac revascularizations in selected cases.
revascularizations in selected cases.
Do you have cross-training? Who scrubs, who circulates and who monitors?
Nurses are cross-trained in all areas of the lab. They are trained to scrub in all cases, including cardiovascular and peripheral vascular angiograms and interventions. They also circulate, monitor and record. RTs are trained to scrub and record as well in the circulating role, but are not involved in administering medications to the patients.
How does your cath lab handle radiation protection for the physicians and staff?
Along with lead aprons, zero gravity lead is available for physician use as well as RadPads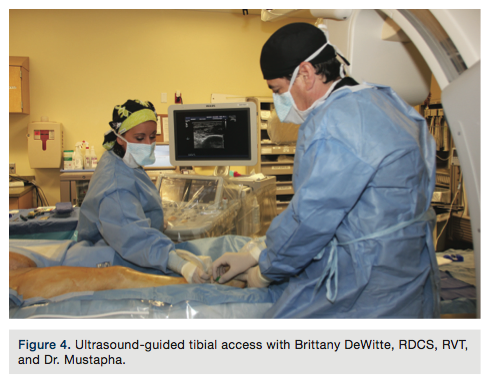 (Worldwide Innovations & Technologies, Inc.), which are utilized during long peripheral vascular interventions. These help protect the vascular technologists and the physician. Lead gloves and a lead skirt on wheels are also available. We also have mobile and repositionable lead barriers with windows. Physicians also utilize radiation glasses. Dosimeter badges are worn in the labs and radiation exposure is monitored on a routine basis. Education is provided to staff during orientation. Lead aprons are checked routinely and replaced when compromised.
(Worldwide Innovations & Technologies, Inc.), which are utilized during long peripheral vascular interventions. These help protect the vascular technologists and the physician. Lead gloves and a lead skirt on wheels are also available. We also have mobile and repositionable lead barriers with windows. Physicians also utilize radiation glasses. Dosimeter badges are worn in the labs and radiation exposure is monitored on a routine basis. Education is provided to staff during orientation. Lead aprons are checked routinely and replaced when compromised.
Since the inception of extravascular ultrasound (EVUS) to guide arterial access and interventions, our radiation usage has decreased significantly.
Are you recording fluoroscopy times/dosages?
Yes, we record both time and dosage in our procedure log. Both are monitored closely during our PVIs. We cut off at 40 minutes for patients with Rutherford III, 60 minutes for patients with Rutherford IV-V, and 90 minutes for patients with Rutherford VI. Since the introduction of EVUS, these times have consistently decreased.
our PVIs. We cut off at 40 minutes for patients with Rutherford III, 60 minutes for patients with Rutherford IV-V, and 90 minutes for patients with Rutherford VI. Since the introduction of EVUS, these times have consistently decreased.
Who pulls the sheaths post procedure?
Nurses and RTs are trained to pull sheaths of all sizes both post diagnostic and post intervention. The trainee first observes an experienced nurse or RT for several sheath pulls. The trainer describes the hold technique and demonstrates the most effective way to hold the groin in order to ensure proper pressure to obtain hemostasis in patients with both antegrade and retrograde punctures. Once the trainee feels comfortable, he or she is observed for several sheath pulls until it is determined the trainee has mastered the technique. They are also trained in the removal of radial, pedal, and tibial sheaths.
describes the hold technique and demonstrates the most effective way to hold the groin in order to ensure proper pressure to obtain hemostasis in patients with both antegrade and retrograde punctures. Once the trainee feels comfortable, he or she is observed for several sheath pulls until it is determined the trainee has mastered the technique. They are also trained in the removal of radial, pedal, and tibial sheaths.
Where are patients prepped and recovered (post sheath removal)?
Patients are prepped and recovered in the cardiovascular lab holding area. If the doctor does not use a closure device post procedure in the lab, the femoral sheath is pulled in holding by a nurse or RT once the activated clotting time (ACT) is at or below 150. Radial, pedal and tibial sheaths are pulled as soon as possible, regardless of the ACT. The nurse is responsible to monitor the patient, checking the site on a regular basis for bleeding or the presence of a hematoma.
Are your physicians dictating their cath procedure reports, or do they use a structured reporting tool?
Our physicians dictate and are currently working toward a more structured dictation template for peripheral vascular intervention reporting. This will allow for consistency and better compliance with ICD 10.
Has your cath lab recently expanded in size and patient volume?
Yes, patient volume continues to increase. In order to accommodate future growth, plans are being made to open a third cardiovascular lab and increase staffing. Since 2008, when we began performing peripheral vascular procedures, our organization has observed a continuously increasing influx of patients referred for peripheral artery disease (PAD) evaluation and treatment. As the number of referrals and peripheral vascular interventions has increased, the incidence of major amputation at Metro Health has dramatically decreased (Figures 10-11).
being made to open a third cardiovascular lab and increase staffing. Since 2008, when we began performing peripheral vascular procedures, our organization has observed a continuously increasing influx of patients referred for peripheral artery disease (PAD) evaluation and treatment. As the number of referrals and peripheral vascular interventions has increased, the incidence of major amputation at Metro Health has dramatically decreased (Figures 10-11).
Do you use the American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) or any other outside data collection registry?
Data Registry (ACC-NCDR) or any other outside data collection registry?

Currently, we belong to the ACTION Registry, PCI Registry, ICD 10 Registry and BMC2 Registry for Cardiac and PV.
Is your lab involved in clinical research?
Yes, our lab is heavily involved in both industry-sponsored and investigator-initiated clinical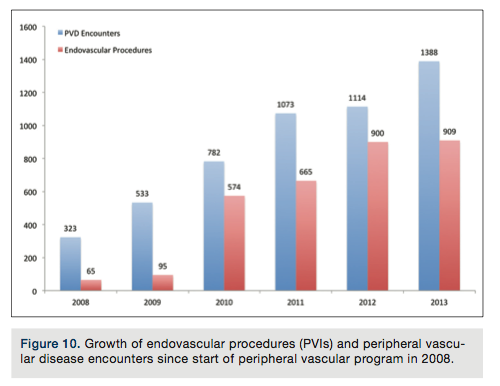 trials. These include studies on pacemaker/defibrillators, pharmacological agents used in patients post myocardial infarctions, and a large variety of studies on PAD and critical limb ischemia (CLI). Currently, eight clinical research nurses support the peripheral vascular studies at Metro Health. The Peripheral RegIstry of Endovascular Clinical OutcoMEs (PRIME) Research Database is a multi-center registry that was initiated at Metro Health in January of 2013 with the intention of studying patients with CLI. The main objective is to look for answers to common and frequent clinical questions that arise in the management of these complex patients with multiple comorbidities who are unlikely to be eligible for enrollment in randomized clinical trials due to the nature and gravity of their disease process.
trials. These include studies on pacemaker/defibrillators, pharmacological agents used in patients post myocardial infarctions, and a large variety of studies on PAD and critical limb ischemia (CLI). Currently, eight clinical research nurses support the peripheral vascular studies at Metro Health. The Peripheral RegIstry of Endovascular Clinical OutcoMEs (PRIME) Research Database is a multi-center registry that was initiated at Metro Health in January of 2013 with the intention of studying patients with CLI. The main objective is to look for answers to common and frequent clinical questions that arise in the management of these complex patients with multiple comorbidities who are unlikely to be eligible for enrollment in randomized clinical trials due to the nature and gravity of their disease process.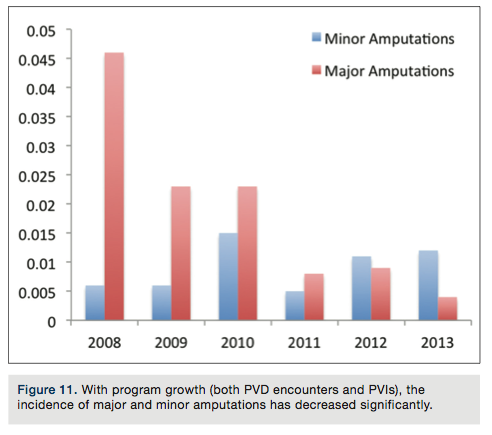
How are new employees oriented and trained at your facility?
Currently, new hires go through three months of intense on-the-job training in the labs for cardiovascular procedures. Included in this training are right and left heart catheterizations, pacemaker/implantable cardioverter defibrillator (ICD) implants, and patient prep and recovery skills utilized in the holding area. Nurses are trained to scrub, record, monitor and circulate. RTs go through the same training, with the exception of conscious sedation training. After six months and if competency has been demonstrated in previously taught areas, the new hire is trained in the peripheral vascular arena. This training is also intense and continues until the employee is proficient. It can and usually does take six months to a year for the employee to feel comfortable in this role.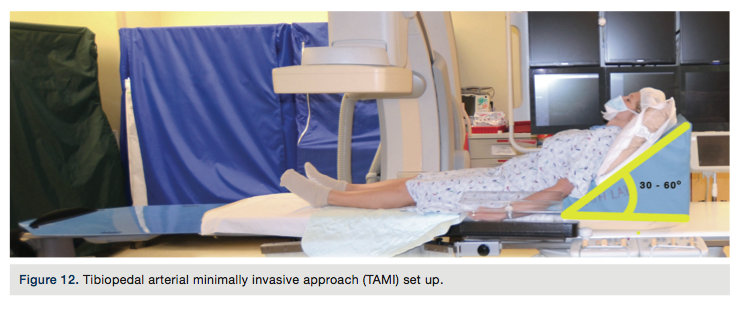
What continuing education opportunities are provided to staff members?
Staff members are provided with multiple opportunities to contribute to and attend educational in-services and conferences. Our cath lab hosts multiple physician training courses throughout the year. These courses provide ample opportunity for staff to remain current with rapidly evolving technology and new low-profile devices utilized in complex peripheral vascular interventions.
Most noteworthy is our institution’s engagement in the AMPutation Prevention Symposium. Many of our staff members are faculty and others are able to attend this educational meeting. AMP is the first meeting of its kind, totally devoted to critical limb ischemia. The 4th annual AMPutation Prevention Symposium will be held August 14-16, 2014 at the Palmer House Hilton in Chicago, Illinois. In addition to a hands-on Atherectomy Summit, including ultrasound mapping with live models and tibial access training on cadaveric models, a Vascular Technology Ultrasound Workshop has been added this year. Check out the agenda at www.AMPtheCLImeeting.com.
What trends have you seen in your procedures and/or patient population?
As PAD is becoming more prevalent, we have witnessed significant increases in complex CLI cases.
Is there a problem or challenge your lab has faced?
The rapid growth of our program, despite being a good problem to have, presented a shortage of experienced staff. The training period for a new cath lab employee is steep, especially with the performance of complex peripheral vascular limb salvage cases. With institutional and leadership support of growth and education, patience and a cohesive team, we have successfully maintained this growth.
What is unique about your cath lab and staff?
Our staff consists of a tight-knit group of nurses, RTs and doctors. Our physicians and cath lab staff pioneer the use of existing devices in the peripheral vascular arena. An example of this is the use of EVUS, utilizing the 15-MHz i7 hockey stick probe (Philips Healthcare), for diagnosis, access and intervention. A vascular ultrasound technician is scheduled for each case. This addition has increased our ability to gain arterial access in patients with complex anatomy, as well as our crossing success while decreasing complications, procedure time, contrast usage and radiation exposure.
The Tibiopedal Arterial Minimally Invasive (TAMI) Retrograde Revascularization approach was born in our lab out of a need for access for patients unable to undergo or tolerate common femoral artery access and intervention due to body habitus or comorbidities. Using this approach, operators are able to access and revascularize the lower extremity completely via tibial-pedal arterial access. A decrease in groin access complications, in this complex patient population, has been experienced with this approach. The patients are able to recline on the table at a 30-45 degree angle during the procedure. They are also able to ambulate one hour after their procedure. Hemostasis is easily obtained using a tibial compression device for one hour post sheath removal. The device is loosened, access site evaluated, and distal pulses checked every 15 minutes. The TAMI approach required an innovative approach to patient preparation. The entire target limb and bilateral groins are prepped in the event additional urgent access is required. Additionally, an extended table set up is required for these cases (Figure 12).
What is the first necessary step in building a successful CLI program?
The first step in building a successful CLI program is to obtain the support of your institution’s leadership and support of primary stakeholders. Our institution is fortunate to have the vision and leadership of Michael Faas, President and CEO. Also, identification of a passionate and engaged program champion to lead the program is key. Five hospital-based interventional cardiologists, Drs. Walchak, Mustapha, Karenko, Diaz, and Saab, fulfill this capacity with their passion for peripheral vascular disease and interventions. Additionally, Drs. Kovack, Sevensma, and Key are also involved in screening, non-invasive diagnostic testing, and long-term follow up of the CLI patients.
Current knowledge of economics of amputation versus treatment must be researched, including the financial impact of amputation. Due to the multiple comorbidities present in CLI patients, the development of a CLI program provides opportunity for an institution to expand other service lines and the downstream revenue that can come from additional cardiac evaluations, carotid evaluations, abdominal aortic aneurysm (AAA) screening, venous evaluation and interdisciplinary referrals such as podiatry, wound care, infectious disease, primary care, and physical therapy.
One hurdle in gaining support for development of a CLI program to hospital administration is providing justification for lengthy complex revascularization procedures. Success requires an investment in the program and in talent development. It requires patience and an institutional commitment to patient-centered care. It takes time to build a sustainable program. Institutions and practices need to be prepared for the future. Peripheral arterial disease (PAD) and CLI is on the rise and expensive to treat. Being shortsighted and not preparing to treat this ever-increasing patient population could be more costly to the organization and to society in the long run.
It is difficult to place monetary cost on the psychosocial impact of amputation to a patient. However, as stated by Einstein, “not everything that counts can be counted, and not everything that can be counted counts.”
The 4th annual AMPutation Prevention Symposium will be held August 14-16, 2014 at the Palmer House Hilton
in Chicago, Illinois.
Visit www.AMPtheCLImeeting.com
