


ADVERTISEMENT
The Cardiosave IABP: An Early Adopter’s Report
 Ivan Feticio shares his experience handling the Cardiosave™ intra-aortic balloon pump (IABP), the newest IABP from MAQUET Cardiovascular. Currently CE marked and having received FDA 510(k) clearance, Cardiosave is expected to be commercially available in the U.S. beginning in January 2012.
Ivan Feticio shares his experience handling the Cardiosave™ intra-aortic balloon pump (IABP), the newest IABP from MAQUET Cardiovascular. Currently CE marked and having received FDA 510(k) clearance, Cardiosave is expected to be commercially available in the U.S. beginning in January 2012.
Tell us about your history in the cath lab.
 All my cardiac catheterization experience and training, including balloon pump exposure, began in the Philippines at the Philippine Heart Center in Quezon City. It was at this hospital that I learned and trained to be an invasive cardiovascular technologist, starting almost eleven years ago. My focus in the Philippines was on adult and pediatric invasive procedures, both diagnostic and therapeutic interventions. I was fortunate to have a great deal of exposure to balloon pump set up and use in the Philippines. During my time at the Philippine Heart Center, we utilized pumps from two IABP manufacturers, Arrow and Datascope (now part of MAQUET). I had exposure to both IABP machines and am familiar with older IABP models.
All my cardiac catheterization experience and training, including balloon pump exposure, began in the Philippines at the Philippine Heart Center in Quezon City. It was at this hospital that I learned and trained to be an invasive cardiovascular technologist, starting almost eleven years ago. My focus in the Philippines was on adult and pediatric invasive procedures, both diagnostic and therapeutic interventions. I was fortunate to have a great deal of exposure to balloon pump set up and use in the Philippines. During my time at the Philippine Heart Center, we utilized pumps from two IABP manufacturers, Arrow and Datascope (now part of MAQUET). I had exposure to both IABP machines and am familiar with older IABP models.
 Six years ago, I moved to the United Kingdom (UK) and began working at Harefield Hospital. The Royal Brompton and Harefield NHS Foundation Trust is a partnership of two specialist hospitals in the UK. I am one of the cardiac physiologists at Harefield Hospital, which focuses on the treatment of heart and lung disease (in the UK, a cardiovascular technologist is called a “cardiac physiologist”). The hospital has more than 900 staff, five operating rooms and four cath labs. I work with approximately 30 physiologists. Our ST-elevation myocardial infarction (STEMI) population is drawn from outer northwest London, and we believe our arrival-to-treatment time of 26 minutes is the fastest in Europe. In four cath labs, we perform over 3,000 diagnostic and 2,400 interventional procedures annually.
Six years ago, I moved to the United Kingdom (UK) and began working at Harefield Hospital. The Royal Brompton and Harefield NHS Foundation Trust is a partnership of two specialist hospitals in the UK. I am one of the cardiac physiologists at Harefield Hospital, which focuses on the treatment of heart and lung disease (in the UK, a cardiovascular technologist is called a “cardiac physiologist”). The hospital has more than 900 staff, five operating rooms and four cath labs. I work with approximately 30 physiologists. Our ST-elevation myocardial infarction (STEMI) population is drawn from outer northwest London, and we believe our arrival-to-treatment time of 26 minutes is the fastest in Europe. In four cath labs, we perform over 3,000 diagnostic and 2,400 interventional procedures annually.
At Harefield, I am involved in all cardiology invasive and non-invasive procedures, except echocardiogram.
What do your current IABP responsibilities involve at Harefield Hospital?
My responsibilities involve setting up the pump, connecting it to the patient, monitoring while inside the cath lab room, transporting the IABP, troubleshooting, cleaning after removal from the patient, and training of junior staff.
Are you using IABPs prophylactically?
 It depends on the patient presentation. Most of the time we use it for acute MI patients in cardiogenic shock, and sometimes prophylactically.
It depends on the patient presentation. Most of the time we use it for acute MI patients in cardiogenic shock, and sometimes prophylactically.
How long have you been using the Cardiosave?
We have used it on 18 patients (10 for pacer detection evaluation) during a limited commercial trial at Harefield Hospital. It has been almost a month now. We used 2 Cardiosave pumps during that period, every time a patient needed a balloon. We like it and if feasible, would like to change all our balloon pumps to Cardiosave.
How would you compare it against previous IABP systems?
 The first model I used was the Datascope System 95, which was a very big machine and then the succeeding models, the System 97, System 98, CS100, CS300, and now, Cardiosave. From a bigger machine, the IABP has become smaller and lighter. Performance has improved, and the interface has changed. The old one was a monochrome orange. The Cardiosave interface is very lively. Everything is color-coded, from the ECG tracing to the point of inflation on the dicrotic notch, pressure waveform and balloon pressure waveform. The older
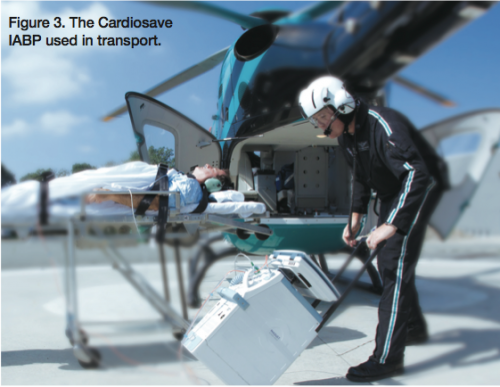
The first model I used was the Datascope System 95, which was a very big machine and then the succeeding models, the System 97, System 98, CS100, CS300, and now, Cardiosave. From a bigger machine, the IABP has become smaller and lighter. Performance has improved, and the interface has changed. The old one was a monochrome orange. The Cardiosave interface is very lively. Everything is color-coded, from the ECG tracing to the point of inflation on the dicrotic notch, pressure waveform and balloon pressure waveform. The older  models were heavy and difficult to maneuver. It is not easy to transport a patient with a balloon pump. Battery life has been a concern, particularly if you are going to transport a patient. You worry about whether the battery is sufficient for the journey, especially if it is a long journey to another hospital. As a tech, this is one of my primary concerns. So I would say that problems with IABPs have included the fact that they are big, heavy, difficult to maneuver, loud when working, have potentially inadequate battery power for long transports, and a simplistic, monochrome interface. In addition, getting the console off the cart is difficult, especially if the patient is being transported via ambulance or helicopter.
models were heavy and difficult to maneuver. It is not easy to transport a patient with a balloon pump. Battery life has been a concern, particularly if you are going to transport a patient. You worry about whether the battery is sufficient for the journey, especially if it is a long journey to another hospital. As a tech, this is one of my primary concerns. So I would say that problems with IABPs have included the fact that they are big, heavy, difficult to maneuver, loud when working, have potentially inadequate battery power for long transports, and a simplistic, monochrome interface. In addition, getting the console off the cart is difficult, especially if the patient is being transported via ambulance or helicopter.
Does the Cardiosave address any of these problems?
 Yes, when compared with older models, even the CS300, all of the challenges for use I listed are addressed with Cardiosave. When I used it during transport of a patient going to an intensive care unit, I found that I was able to “drive” it with one hand. It is very light. Cardiosave is smaller compared with older models, and quieter compared to the CS300. The user interface has improved and new features have been added, but it retains its familiar appearance, something I love about Cardiosave. If you are very familiar with the older models, you can immediately use it. The screen, especially the upper display is larger, with improved help screen navigation and Touchscreen controls.
Yes, when compared with older models, even the CS300, all of the challenges for use I listed are addressed with Cardiosave. When I used it during transport of a patient going to an intensive care unit, I found that I was able to “drive” it with one hand. It is very light. Cardiosave is smaller compared with older models, and quieter compared to the CS300. The user interface has improved and new features have been added, but it retains its familiar appearance, something I love about Cardiosave. If you are very familiar with the older models, you can immediately use it. The screen, especially the upper display is larger, with improved help screen navigation and Touchscreen controls.
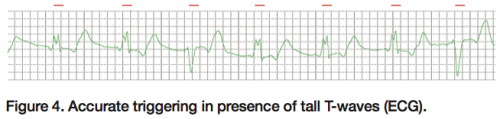
 Pacer detection has been enhanced. The pump has the ability to detect and analyze pacer spikes simultaneously in multiple leads. We have tried the pacing enhancement on our pacing-dependent patients. It works well. Another feature that I like is ECG Lead Fault Detection. When the ECG lead is disconnected or the electrode is off, normally you have to figure out which lead is disconnected. Cardiosave pinpoints the disconnected lead or electrode immediately. It helps me reconnect the ECG lead quickly and saves time. Regarding enhanced triggering performance, Cardiosave will abort triggering on the T-wave, a very nice feature, especially for ischemic patients. T-waves that are 120% of the R-wave amplitude will be rejected, as opposed to 70% with the CS300. It offers greater immunity to electrosurgical interference, minimizing the need to switch from ECG Trigger to Pressure Trigger in the O.R. There is a lower voltage threshold requirement for triggering in ECG Trigger, eliminating the need for manual ECG gain adjustment. In terms of design, if you are using an older model, the power button is in the front, and the helium tank is in the back of the balloon pump along with a power cord that does not retract. This has changed with Cardiosave. Everything is nicely designed and organized, as reflected by the user-friendly patient interface connections, easier access to the connection panel, and color-coded and keyed connections. I like the lock button of the Touchscreen. In the older models, anyone can change the setting accidentally or intentionally. Now, if you set your balloon pump and use the lock button, no one can accidentally change it. The power cord is retractable. After unplugging it from the mains, it will retract itself and is hidden. In the older models, the ECG cable, transducer cable and Doppler had a tailored bag attached to the side. Now they have their own compartment. Cardiosave has 2 hot-swappable lithium ion batteries, a great help if you are going to be transporting a patient for a long journey.
Pacer detection has been enhanced. The pump has the ability to detect and analyze pacer spikes simultaneously in multiple leads. We have tried the pacing enhancement on our pacing-dependent patients. It works well. Another feature that I like is ECG Lead Fault Detection. When the ECG lead is disconnected or the electrode is off, normally you have to figure out which lead is disconnected. Cardiosave pinpoints the disconnected lead or electrode immediately. It helps me reconnect the ECG lead quickly and saves time. Regarding enhanced triggering performance, Cardiosave will abort triggering on the T-wave, a very nice feature, especially for ischemic patients. T-waves that are 120% of the R-wave amplitude will be rejected, as opposed to 70% with the CS300. It offers greater immunity to electrosurgical interference, minimizing the need to switch from ECG Trigger to Pressure Trigger in the O.R. There is a lower voltage threshold requirement for triggering in ECG Trigger, eliminating the need for manual ECG gain adjustment. In terms of design, if you are using an older model, the power button is in the front, and the helium tank is in the back of the balloon pump along with a power cord that does not retract. This has changed with Cardiosave. Everything is nicely designed and organized, as reflected by the user-friendly patient interface connections, easier access to the connection panel, and color-coded and keyed connections. I like the lock button of the Touchscreen. In the older models, anyone can change the setting accidentally or intentionally. Now, if you set your balloon pump and use the lock button, no one can accidentally change it. The power cord is retractable. After unplugging it from the mains, it will retract itself and is hidden. In the older models, the ECG cable, transducer cable and Doppler had a tailored bag attached to the side. Now they have their own compartment. Cardiosave has 2 hot-swappable lithium ion batteries, a great help if you are going to be transporting a patient for a long journey.
Although we are not currently using the Sensation® fiber-optic IAB catheter, Cardiosave has a fiber-optic port option where you can plug in this type of IAB, press the start button, and the system will start pumping accordingly.
I highly recommend Cardiosave. This is the best balloon pump I have seen. You won’t regret buying it. It’s the iPhone 4 of balloon pumps.
Ivan Feticio can be contacted at heartmaker_ivan@yahoo.com.
