


Building or Renovating an Interventional Suite: Proven Solutions for Common Pitfalls
 Whether the decision at your organization is to upgrade the existing facility or to build from the ground-up, construction or renovation of an interventional suite is no longer about the square footage and equipment selection alone. The endless decisions, directions, conflicts, and attention to minutiae associated with a project of such magnitude can exhaust and overwhelm even the most seasoned of cardiovascular administrators.
Whether the decision at your organization is to upgrade the existing facility or to build from the ground-up, construction or renovation of an interventional suite is no longer about the square footage and equipment selection alone. The endless decisions, directions, conflicts, and attention to minutiae associated with a project of such magnitude can exhaust and overwhelm even the most seasoned of cardiovascular administrators.
It is imperative, however, that full effort and attention to the smallest of details be employed in order to ensure that the completed project will result in a fully functional room for both physicians and staff. The risk of squandering precious capital resources by inadequate planning is never an option — especially during today’s tough economic times!
Corazon’s experience in assisting with interventional suite planning, development, and program implementations at hospitals across the U.S. has given us the benefit of a broad-based, firsthand knowledge of the challenges and common pitfalls of these projects. An understanding of these challenges and a proactive approach in circumventing the roadblocks can be invaluable in ensuring successful and on-time completion. The following are some of the common pitfalls and associated questions that we encourage our client partners to ask when involved in cath lab and interventional suite construction, upgrades, and new equipment installs.
Lack of current knowledge with respect to equipment and technology advances
One of the most frustrating situations a project leader can experience is to spend months identifying the perfect piece of equipment for a new lab, only to find that as soon as the purchase order is issued, a new and improved version of the multi-million dollar item has been released to the market. Perhaps even worse: being informed by an involved physician that the newly-bought equipment will not meet his/her needs, or that a major component was overlooked during the vetting process. We believe that there are several steps that the savvy administrator can take during the equipment selection process in order to be sure that neither financial nor political capital are expended unnecessarily.
Do you have adequate knowledge of the technology and equipment currently available to make a fully informed purchasing decision?
The extraordinary pace of technological advancement in the areas of imaging and intervention make it difficult, if not impossible, for a service line administrator to remain current. Even the tried and true methods of periodical review and the sharing of anecdotal information among colleagues can cause delays in knowing about ‘the latest and greatest.’ We advocate a much more focused approach for information gathering, which can prove essential to success.
If considering a partnership with a particular vendor, we recommend speaking with references that you have identified, and not only those supplied by the vendor partner. During these conversations, seek out specific information that will be useful during the decision-making process. “We love it” or “We hate it” is really not enough information to realistically and adequately help in a decision of this magnitude. Instead, questions about reliability, functionality, customer service, training, and included or excluded software upgrades and the resulting information will be much more useful.
Failure to adequately address patient flow issues
Failing to examine current patient flow practices and then objectively evaluate the current process for inefficiencies and opportunities for improvement can lead to missed opportunities in the development of a truly patient-centric suite. We recommend engagement of all those in the organization who currently work in this environment. Every step of the current patient flow, including movement through the pre and post areas, as well as the lab itself, should be thoroughly examined. By asking the right questions, valuable insights can be gained as to how changes to existing design can lead to improved function.
Are the pre and post areas adequate to ensure safe and timely movement of patients in and out of the suite?
In order to gain maximum efficiency, the pre and post areas must be adequate to handle anticipated growth in volumes, ensure patient confidentiality, and facilitate 360-degree access to the patient by caregivers. Bottlenecks in this area can limit the capacity of the cath lab or interventional suite itself, and result in under-utilization or reluctance on the part of clinicians to schedule to capacity.
Does the size, configuration, and equipment layout within the interventional suite meet current and future needs (with respect to integration of new services, new technology, and expanded staff)?
Space constraints at most organizations compel leaders to plan any new patient care area in the least amount of space possible while ensuring maximum efficiency. The nature of the services to be provided in the room must be examined not only within the framework of the current state, but also with the future state in mind. In order to be thorough in this analysis, the service line leader should again query a broad group of colleagues so as to gain a full understanding of plans for expansion at the organizational level. Such valuable information should form the foundation for decision making.
- Are there plans for physician recruitment that would result in either additional volume or the addition of new services?
- Is there any opportunity to develop a dual-use room to be shared by both cardiology and radiology, for example
- Is the provision of neuro endovascular services a potential area of expansion for your organization?
- Has medical staff leadership expressed interest in future plans that would allow greater utilization of an interventional suite if the necessary technology were integrated into the expansion/development project?
Lack of proper planning with respect to technology integration
The days of installing a stand-alone piece of equipment in a newly-renovated room and ‘calling it a day’ are no longer! Integration of the MacLab (GE Medical, Waukesha, Wisc.), for example, is now the first step in an ever-expanding line of technology needs in any interventional suite. This need is perhaps the most complex in the area of neuro-endovascular capabilities. Integration of record-keeping relative to the administration of general anesthesia, physiologic monitoring, intra-procedural neuro monitoring, nursing documentation systems, electronic medical record requirements, drug administration, and intra-procedural documentation requires an extraordinary effort to achieve maximum functionality and adequate documentation. Many of these systems do not easily communicate with each other; often, the answer to the question “is this possible?” from many vendors may be “no.” We find that by involving available in-house technology experts, collaborating closely with vendor partners, and pushing the boundaries of what has been accomplished previously, a high degree of integration is indeed possible. In order to be successful, a clearly articulated, well-thought-out vision for necessary inter-connectivity must be developed in advance of any meaningful discussion.
Accepting the status quo — possibly the largest pitfall of all
Perhaps the best advice we can give is to not acquiesce and accept a solution that falls short of meeting your needs. With clinical and/or operational knowledge and a strong commitment to quality patient care, the savvy leader must trust instincts and advocate for future patients by not “settling” for a less-than-optimal solution. To do so only leads to “work-around” solutions that breed frustration and disappointment for all involved.
Construction or renovation of an interventional suite is perhaps one of the largest and most visible projects that a service line administrator may undertake. The rewards of diligent planning, total organizational commitment, and the involvement of leading experts in both leadership and at the operational level can yield truly remarkable results.
Stacey Lang can be contacted at slang@corazoninc.com.
_________________________________________________________________
Case Study: Bon Secours Virginia Health System
 We at Corazon have had the privilege of partnering with the Bon Secours Virginia Health System over the past two years in the development of a world-class neuroscience center at DePaul Medical Center in Norfolk, Virginia. Under the leadership of Dr. Timothy Shephard, Vice President of Neurosciences, Bon Secours Virginia and Jennifer Smith, Administrative Director Neurosciences, Hampton Roads, DePaul has evolved from a small community hospital into a tertiary neuroscience center offering a full range of neuroscience services. In July 2011, a state of the art neuro-endovascular lab was opened after a nine-month planning and construction process.
We at Corazon have had the privilege of partnering with the Bon Secours Virginia Health System over the past two years in the development of a world-class neuroscience center at DePaul Medical Center in Norfolk, Virginia. Under the leadership of Dr. Timothy Shephard, Vice President of Neurosciences, Bon Secours Virginia and Jennifer Smith, Administrative Director Neurosciences, Hampton Roads, DePaul has evolved from a small community hospital into a tertiary neuroscience center offering a full range of neuroscience services. In July 2011, a state of the art neuro-endovascular lab was opened after a nine-month planning and construction process.
 The leadership at Bon Secours fully embraced a work group development model recommended by Corazon. Together we identified resources, both internal and external, to participate in the various work groups. Dr. John R. Baker, Medical Director, DePaul Neurovascular Center, served as medical lead for the project and provided invaluable direction gleaned from similar projects. All involved committed to weekly, and at times, twice-weekly meetings in order to remain on time and on track. Design and construction, equipment and supplies, information systems, and staff education committees were developed at project inception and continue through today.
The leadership at Bon Secours fully embraced a work group development model recommended by Corazon. Together we identified resources, both internal and external, to participate in the various work groups. Dr. John R. Baker, Medical Director, DePaul Neurovascular Center, served as medical lead for the project and provided invaluable direction gleaned from similar projects. All involved committed to weekly, and at times, twice-weekly meetings in order to remain on time and on track. Design and construction, equipment and supplies, information systems, and staff education committees were developed at project inception and continue through today.
 The extraordinary commitment of all involved and the excruciating attention to detail that each embraced resulted in a completely functional, exceptionally efficient, patient-centric room that will serve the organization well into the future.
The extraordinary commitment of all involved and the excruciating attention to detail that each embraced resulted in a completely functional, exceptionally efficient, patient-centric room that will serve the organization well into the future.
The experience at Bon Secours perfectly illustrates the benefit of an organized, thoughtful, and comprehensive approach to the planning and development of an interventional suite.
Some of the benefits of that attention to detail during the planning phase are evident:
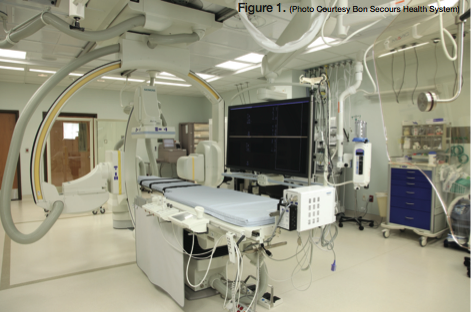
- The patient enters the room from the foot of the table on the right side. As a result, table controls were placed on the left side of the table in order to avoid wear and tear associated with moving patients back and forth over these delicate controls (Figure 1).
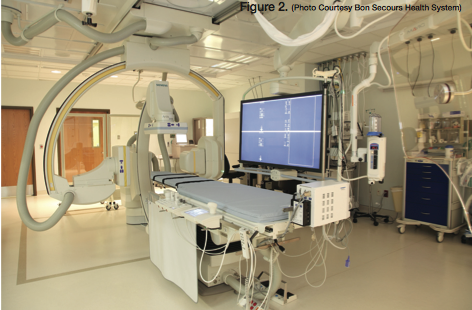
- All necessary cables, wires, etc., are either suspended from the ceiling or hidden beneath the floor, exiting just under the table. This allows for the unimpeded movement of equipment and staff through the room without fear of obstruction (Figure 2).
- Note the demarcated area on the floor at the head of the table surrounding the gantry (Figure 3). This visual reminder of the “Zone of Destruction,” as described by Dr. Baker, was installed to discourage employees from moving through this area and eliminate the tendency of mobile equipment being placed unsafely within the room.
