


Ask the Clinical Instructor: Shock and BP
 Todd is the Cardiology Manager for Memorial Hermann Southeast in Houston, Texas. He also teaches an online RCIS Review course for Spokane Community College, in Spokane, Washington, and regularly presents with RCIS Review Courses.
Todd is the Cardiology Manager for Memorial Hermann Southeast in Houston, Texas. He also teaches an online RCIS Review course for Spokane Community College, in Spokane, Washington, and regularly presents with RCIS Review Courses.
We had a case where the patient developed a low BP and became critical. The physician said something about recognizing it too late. We notice the BP immediately. What was he talking about? — Spokane Community College RCIS Review Online Class submission.
The physician was likely talking about the blood pressure (BP) drop being one of the later changes in vital signs when a patient progresses into a shock state. To answer this, we first need to provide some background.
Shock is defined as a medical emergency in which the organs and tissues of the body are not receiving an adequate flow of blood. This deprives the organs and tissues of oxygen (carried in the blood). Shock can result in serious damage to tissues and organs, or even death.
There are a few common types of shock: hypovolemic, cardiogenic, septic, neurogenic (for example, vasovagal responses — see Dr. Kern’s Editor’s Corner in this issue) and anaphylactic. For the purpose of this article, we will refer to hypovolemic and cardiogenic shock in patients that may come to the cath lab. Cardiogenic shock is defined as a shock state (< 80 mmHg systolic) for 30 minutes or more in which the heart/vasculature is suspected as the culprit and other causes have been ruled out.1
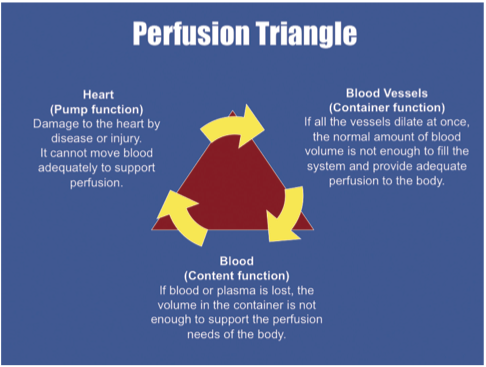 To have a functioning circulatory system, there are three main components required: the fluid (blood), the pipes (vasculature) and the pump (heart) (Figure 1). If any one of these items is malfunctioning, the body can go into a shock state. Think of it as the engine of a car. In order for the car to run properly, it needs a functioning motor (pump), gas (fluids) and gas lines to get the gas to the pump (vessels). If any of these are not functioning properly, our car doesn’t run very well, and will often get worse if we don’t fix it.
To have a functioning circulatory system, there are three main components required: the fluid (blood), the pipes (vasculature) and the pump (heart) (Figure 1). If any one of these items is malfunctioning, the body can go into a shock state. Think of it as the engine of a car. In order for the car to run properly, it needs a functioning motor (pump), gas (fluids) and gas lines to get the gas to the pump (vessels). If any of these are not functioning properly, our car doesn’t run very well, and will often get worse if we don’t fix it.
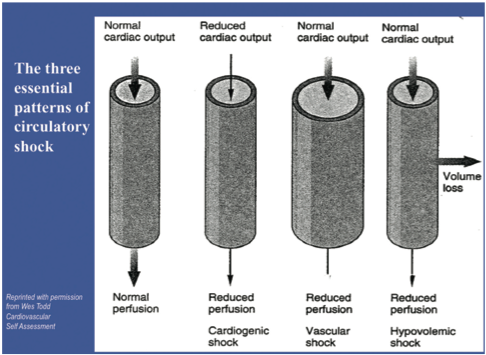 In hypovolemia, the culprit is usually due to a lack of fluid (Figure 2). However, in trauma, that lack of fluid can be caused by holes in the pipes, which is the reason for the lack of fluid. Most of the patients that we will see develop some form either cardiogenic shock due to pump failure, or because of alterations in the pipes.
In hypovolemia, the culprit is usually due to a lack of fluid (Figure 2). However, in trauma, that lack of fluid can be caused by holes in the pipes, which is the reason for the lack of fluid. Most of the patients that we will see develop some form either cardiogenic shock due to pump failure, or because of alterations in the pipes.
When shock develops, there are certain things that happen as the body tries to respond to the crisis and “fix” itself. We will outline a few basic and easy-to-see concepts.
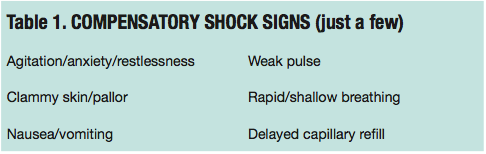 In the beginning of shock (also called COMPENSATORY), a number of systems are activated to counteract the insult on the body (Table 1). During this stage, cells sense the hypoxia because of the lack of blood flow (perfusion) they are receiving. As a result, anaerobic metabolism begins to occur in order to attempt to maintain cellular function. This anaerobic metabolism, however, causes a buildup of lactic acid (a byproduct of of anaerobic metabolism) and results in systemic metabolic acidosis.
In the beginning of shock (also called COMPENSATORY), a number of systems are activated to counteract the insult on the body (Table 1). During this stage, cells sense the hypoxia because of the lack of blood flow (perfusion) they are receiving. As a result, anaerobic metabolism begins to occur in order to attempt to maintain cellular function. This anaerobic metabolism, however, causes a buildup of lactic acid (a byproduct of of anaerobic metabolism) and results in systemic metabolic acidosis.
Thinking about this for a minute, we can understand what some of the first “signs” of shock might be. When the cells are hypoxic, those cells can also include the brain. In some cases, we can see restlessness or confusion as the first sign of shock, since the brain can be hypoxic from the reduction in system blood flow.
When metabolic acidosis occurs, the body can often increase the respiratory rate to “blow off” the extra carbon dioxide (CO2). An increase in respiratory rate is often seen as the first “sign” of recognizable shock. The baroreceptors in the aorta and the carotid arteries recognize the hypotension, and cause the release of epinephrine and norepinephrine. We use medications, such as norepinephrine, for example, in the cath lab to help vasoconstrict the vasculature (pipes) to make them smaller to accommodate the loss of circulatory fluid. This sympathetic stimulation causes constriction of arteries and veins to decrease the amount of blood held in the vasculature, causing BP and cardiac output (CO) to be maintained. The sympathetic stimulation can also increase the heart rate and contractility to help maintain BP and CO. Constriction of the arteries also leads to increased peripheral vascular resistance (BP is maintained) and decreased capillary flow (cool skin) while blood is maintained to the core of the body (brain, heart, lungs and kidneys). Sympathetic stimulation can also create bronchodilation (improved air exchange).
The epinephrine released by the body causes an increase in heart rate, with a small effect on the vascular tone (alpha and beta properties of epinephrine); the combined effect hopefully results in an increase in blood pressure.
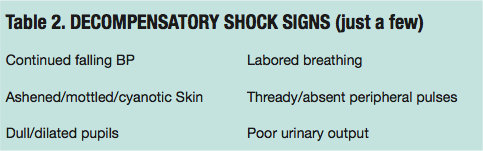 Should the cause of the crisis not be successfully treated, the shock may proceed to the DECOMPENSATORY stage and the compensatory mechanisms begin to fail (Table 2). As anaerobic metabolism continues because of the continued low blood flow, increasing the body’s metabolic acidosis, we can anticipate worsening circulatory status, as blood begins to pool in the microvasculature. This is where we will begin to see the sudden and continued drop in blood pressure, as well as the worsening of the signs and symptoms.
Should the cause of the crisis not be successfully treated, the shock may proceed to the DECOMPENSATORY stage and the compensatory mechanisms begin to fail (Table 2). As anaerobic metabolism continues because of the continued low blood flow, increasing the body’s metabolic acidosis, we can anticipate worsening circulatory status, as blood begins to pool in the microvasculature. This is where we will begin to see the sudden and continued drop in blood pressure, as well as the worsening of the signs and symptoms.
 IRREVERSIBLE shock can develop as the vital organs continue to be starved of oxygen, and the body can no longer provide the rescue mechanisms to prevent it or fix it (Table 3). Brain damage and cell death are happening, and death will occur soon. Because of the continued deterioration of cells due to the hypoxia, we can also see a decrease in heart rate. A decrease in heart rate in addition to a decreased blood pressure is a very ominous sign. (Note: An exception is vasovagal responses, a type of neurogenic shock [again, see Dr. Kern in this issue]).
IRREVERSIBLE shock can develop as the vital organs continue to be starved of oxygen, and the body can no longer provide the rescue mechanisms to prevent it or fix it (Table 3). Brain damage and cell death are happening, and death will occur soon. Because of the continued deterioration of cells due to the hypoxia, we can also see a decrease in heart rate. A decrease in heart rate in addition to a decreased blood pressure is a very ominous sign. (Note: An exception is vasovagal responses, a type of neurogenic shock [again, see Dr. Kern in this issue]).
The point of recognizing these stages is to be able to identify shock EARLIER in the care of the patient. It is true that waiting to identify shock by the drop in blood pressure is a late point in the process. More rapid identification and treatment is needed to keep shock from becoming worse.
Reference
- Libby P, Bonow RO, Mann DL, Zipes DP. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 8th Edition. Philadelphia, Pennsylvania: Elsevier Science; 2007.
Resources
- Berne RM, Levy MN. Cardiovascular Physiology. 8th Edition. St. Louis, Missouri: Mosby; 2001.
- Martini F, Nath J. Fundamentals of Anatomy & Physiology. 8th Edition. San Francisco, California: Pearson Benjamin Cummings; 2009.
