


Ask the Clinical Instructor: A Q&A Column for Those New to the Cath Lab
 also teaches an online RCIS Review course for Spokane Community College, in Spokane, Washington, and regularly presents with RCIS Review Courses.
“I kind of know what LDL and HDL are, and I hear the doctor talk about foam cells and intimal build-up, but sometimes I don’t follow. Can you help?”
— RCIS Online Student
also teaches an online RCIS Review course for Spokane Community College, in Spokane, Washington, and regularly presents with RCIS Review Courses.
“I kind of know what LDL and HDL are, and I hear the doctor talk about foam cells and intimal build-up, but sometimes I don’t follow. Can you help?”
— RCIS Online Student
It can be a difficult concept to understand, particularly when it isn’t something that you talk about every day, and isn’t something that you directly “do” to patients who visit you in the cath lab. However, having an understanding of how things work can sometimes help you when you relate to patients, and more importantly, when you try to take better care of yourself.
This topic has been discussed and presented endlessly, and concepts continue to change as research continues on how the disease process starts in our body. I can relate it to you on a basic level. I must add a disclaimer that I did not do too well in microbiology in school. However, when you apply the concepts towards how we live our everyday life, it can make enough sense to be able to relate to patients who do not have any medical background. A basic review of cholesterol, LDL and HDL is in order.
Cholesterol does have an important body function, including maintaining cell membranes and the permeability of those membranes. When cholesterol deposits in the liver, it is converted to bile. Bile helps to break down fats in the digestive tract, allowing them to help absorb fat-soluble vitamins, such as Vitamins A, D, E, and K. Cholesterol is important in the development and metabolism of hormones.1 Even though low cholesterol is sometimes desired, cholesterol is important for proper metabolism. “Normal” cholesterol levels can vary, depending upon what resource you are using as a guide. While a current recommendation is less than 200 mg/dL,1 the benefits of even lower targets is becoming well known, particularly in patients with cardiovascular disease.
High density lipoprotein (HDL) helps transport certain types of cholesterol to the liver. This is often referred to the “good” type. It is felt that an HDL level of >60 mg/dL can result in an “optimal condition considered protective against heart disease.”2
Low density lipoproteins (LDL) also help transport certain types of cholesterol. This type is often referred as the “bad” type, with a direct correlation to the incidence of cardiovascular disease. In most cases, a “normal” LDL would be less than 100 mg/dL, and in a patient with known cardiovascular disease, less than 70 mg/dL.2 One way to remember the difference is that “low” density is like sludge, and will stick to the vessel walls, and “high” density floats and stays out of the way of the vessel walls.
Now we can review a graphic about the impact of LDL on the vessel walls, and how it 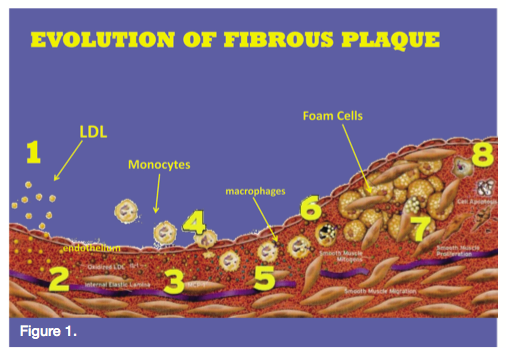 leads to plaque development.
leads to plaque development.
1. As mentioned above, LDL is the “bad” component of cholesterol, and is very sludge-like. When it comes into contact with the vessel wall, it transports the cholesterol it is carrying, and then becomes a deposit in the endothelium that begins the process of plaque.3 2. After these particles are deposited and absorbed, there is an oxidative process that begins a body response to this foreign agent. 3. Monocytes (a type of a white blood cell) respond to this “distress call” to attack a foreign body. 4. In order to reach the ‘invader,’ the monocyte must begin to move through the intimal wall into the deeper components of the vessel. They begin to absorb this oxidized LDL (fat). 5. As macrophages respond to the used-up monocyte, they “engulf and digest” the monocyte containing what was once the LDL. As they become inert, they are considered foam cells. If you have ever seen photos of yellow streaks on the inside of a vessel, these are developed from foam cells. 6. Smooth muscle cells in the intima divide, and other smooth muscle cells migrate into the intima from the media. 7. This results in a buildup of the vessel (smooth muscle proliferation), which begins to impede on the lumen of the cell, starting the blockages that we often treat. This narrowing vessel wall can also be worsened by those fatty streaks on the inside of the vessel wall (as described above). 8. As these cells begin to die, they create a “deposit” within the cell wall and turn into calcium. We can often see these deposits on our angiograms before contrast is even injected. One thing to remember — as this process develops, the “head” of the plaque can often have a very thin layer (or cap) covering it. The thinner the layer, the more likely it is to rupture. That is where the term “vulnerable plaque” arises.
While this isn’t something that we directly manage every day, a basic understanding of what happens can certainly help us when relating to the patient in the management of their disease processes.
References
1. Cholesterol. American Heart Association. Available online at https://www.heart.org/ HEARTORG/Conditions/Cholesterol/Cholesterol_UCM_001089_SubHomePage.jsp. Accessed December 15, 2010. 2. What Do My Cholesterol Levels Mean? (PDF). American Heart Association. September 2007. Available online as a download at https://www.americanheart.org/ presenter.jhtml?identifier=3004817. Accessed December 15, 2010. 3. LDL and HDL Cholesterol: What's Bad and What's Good? American Heart Association. Available online at https://www.americanheart.org/presenter.jhtml?identifier=180. Accessed December 15, 2010.———————————————————— Send us your questions! Todd Ginapp can be contacted at tginapp@rcisreview.com or cathlabdigest@aol.com
