


Appropriate Use Criteria and Complex Coronary Interventions: Where Does Hemodynamic Support Fit?
Case presentation
A 65-year-old man (CD) with hypertension and hyperlipidemia was referred to a cardiologist for evaluation of exertional chest pain while performing his activities of daily living. The patient had severe chronic obstructive pulmonary disease requiring oral steroids and occasional ambulatory inhaled oxygen. His blood pressure was relatively well controlled on hydrochlorothiazide, lisinopril and isosorbide mononitrate. Baseline echocardiogram demonstrated an estimated ejection fraction of 25%. After 5 minutes of exercise, there was worsened function of the anterior and inferior walls with a fixed lateral wall defect. Cardiac catheterization demonstrated a complex, long, calcified proximal to mid left anterior descending coronary artery (LAD) lesion and a 90%, focal, right coronary artery (RCA) lesion. The left circumflex (LCX) was occluded at the ostium, but received collateral circulation from the LAD.
Given the nature of his coronary disease, the patient was referred for coronary artery bypass graft surgery. During his pre-operative evaluation, it was felt that given his advanced pulmonary disease, a percutaneous coronary intervention (PCI) may be more suitable. From the interventional cardiologist’s standpoint, the plan included rotational atherectomy of a long segment of the LAD followed by drug-eluting stent (DES) placement. The RCA would be treated with a balloon angioplasty and stent placement as well. A percutaneous hemodynamic support device was chosen to assist with this high-risk PCI, given the low ejection fraction and the long, diseased segment in the LAD.
CD was admitted the morning of the procedure and underwent successful placement of the Impella 2.5 (Abiomed) hemodynamic system through the left femoral artery. After successful rotational atherectomy of the LAD with a 1.75mm burr (Rotablator, Boston Scientific), he received balloon angioplasty with a 2.5mm balloon followed by placement of 3.0 x 38mm and 3.0 x 16mm everolimus-eluting stents. The final result in the LAD demonstrated no residual stenosis, normal flow and no evidence of dissections. For the RCA, the lesion was predilated and then stented with a 3.0 x 16mm everolimus-eluting stent. At the end of the case, the hemodynamic support device was removed without complication and the patient was admitted to the intensive care unit for observation. CD was discharged on hospital day 2 in good condition.
At our next cath lab business meeting, the billing department manager flagged this case in order to review whether it satisfied appropriate use criteria for PCI (AUC-PCI). It became apparent that this issue was unclear to several colleagues at this meeting. It seemed that a more detailed discussion would be useful. Below is a summary of the application of these guidelines for this patient population.
Hemodynamic support systems and appropriate use criteria
Since its initial publication in 2009, few documents or initiatives have created as much controversy and apprehension as the introduction of appropriateness criteria for coronary revascularization. This piece is not an attempt to support or refute the application of these criteria. Rather, it is to clarify the application of these criteria for a specific patient population, specifically, patients undergoing high-risk PCI with the assistance of a hemodynamic support device who may not be suitable candidates for surgical revascularization.
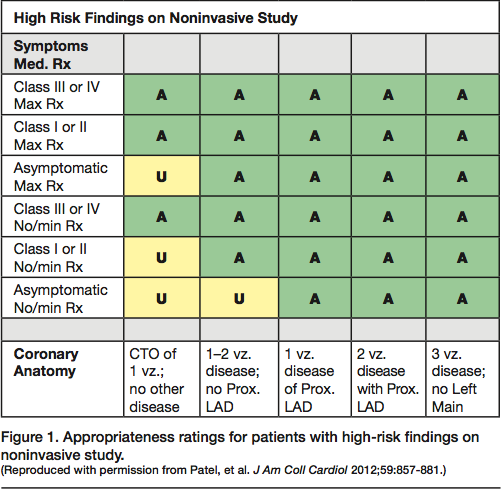
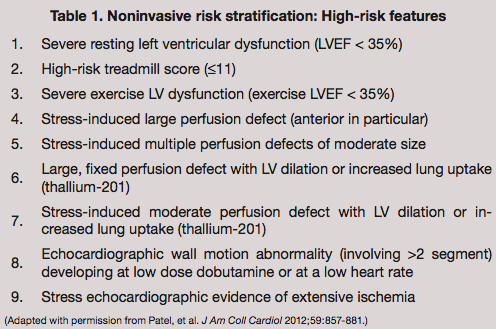 As for most patients requiring hemodynamic support during PCI, CD had symptomatic coronary artery disease, as well as high-risk non-invasive features (Table 1) as described in the Appropriateness Criteria for Coronary Revascularization Guidelines.1,2 In this cohort, revascularization is acceptable for most clinical scenarios and uncertain for a small minority of situations (Figure 1).
As for most patients requiring hemodynamic support during PCI, CD had symptomatic coronary artery disease, as well as high-risk non-invasive features (Table 1) as described in the Appropriateness Criteria for Coronary Revascularization Guidelines.1,2 In this cohort, revascularization is acceptable for most clinical scenarios and uncertain for a small minority of situations (Figure 1).
 Use of hemodynamic support is not discussed in these consensus statements1,2; however, one can refer to the most recent clinical guidelines to define the indication for the use of these devices in clinical practice.3 The 2011 PCI Guideline Statement assigns use of a hemodynamic support device a Class I indication for cardiogenic shock. For carefully selected PCI patients, elective insertion is considered a IIb indication.
Use of hemodynamic support is not discussed in these consensus statements1,2; however, one can refer to the most recent clinical guidelines to define the indication for the use of these devices in clinical practice.3 The 2011 PCI Guideline Statement assigns use of a hemodynamic support device a Class I indication for cardiogenic shock. For carefully selected PCI patients, elective insertion is considered a IIb indication.
Choice of revascularization strategy and appropriate use criteria
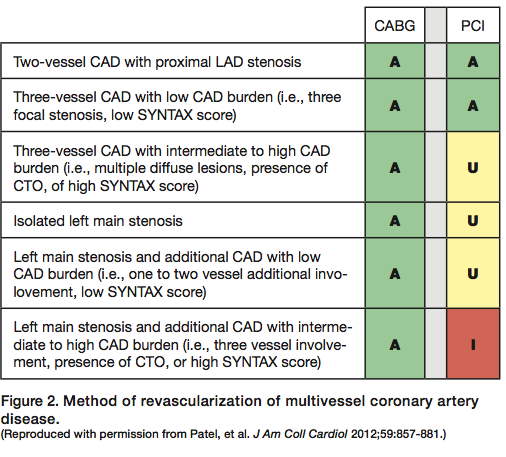 With respect to the method of coronary revascularization for patients with advanced or complex atherosclerosis, the writing group presented various clinical scenarios and independently judged PCI or CABG as a revascularization method (Figure 2). Application of these criteria is limited for patients where such a choice exists. For patients where the method of revascularization is limited to a single strategy, application of the appropriate use classification system is not possible and revascularization should proceed according to the needs of the patient.
With respect to the method of coronary revascularization for patients with advanced or complex atherosclerosis, the writing group presented various clinical scenarios and independently judged PCI or CABG as a revascularization method (Figure 2). Application of these criteria is limited for patients where such a choice exists. For patients where the method of revascularization is limited to a single strategy, application of the appropriate use classification system is not possible and revascularization should proceed according to the needs of the patient.
Urgent/emergent use of hemodynamic support systems is most often in the setting of cardiogenic shock usually due to acute myocardial infarction. Here, the appropriateness guidelines are very clear: revascularization for acute MI is appropriate. Use of hemodynamic support is based upon clinical need and application of clinical practice guidelines.
Conclusion
Appropriateness use criteria represent an important step to improve the overall care of all individuals by reducing variation in practice patterns and aiding clinical decision-making. Clinical context, non-invasive test results, and angiographic findings will determine a patient’s need for revascularization. Use of hemodynamic support systems as an adjunct to PCI can be defined by published clinical practice guidelines. Although not specifically addressed in the AUC classification system, use of a hemodynamic support system occurs primarily in patients with symptomatic coronary artery disease with high-risk features, which satisfies the appropriateness criteria. For patients where only a single revascularization strategy is available, appropriateness criteria are not applicable and revascularization should proceed based on the clinical needs of the patient.
Dr. Shroff can be contacted at arshroff@uic.edu.
References
- Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2009;53:530-553.
- Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2012;59:857-881.
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 2011;124:2574-2609.
