


Aortic Root Mycotic Pseudoaneurysm
Abstract
Aortic root pseudoaneurysms are rare pathologies that can become more complex by a systemic infection and uncontrolled type II diabetes. The presentation of hemodynamic instability and seizures continues to add to the destabilization of the patient, adding to the enigmatic appearance. In the following case, cardiac catheterization proved to be the most sensitive and reasonable investigative tool in primarily diagnosing this condition in the acute presence of chest pain and positive biomarkers.
Case report
MS is a 47-year-old obese male with a past medical history significant for uncontrolled type 2 diabetes, quintuple coronary artery bypass grafting (2006), hypertension, paroxysmal atrial fibrillation, and seizures. Four years post bypass (6/17/2010), MS was found down by his wife, who called emergency medical systems (EMS). Upon arrival, EMS measured a blood glucose of 800. While on the floor, he developed two generalized tonic-clonic seizures that abated spontaneously. He was transported to a small outside hospital. While en route the patient developed sustained wide complex ventricular tachycardia. He was intubated at the outside hospital, and he was loaded with amiodarone and phenytoin (Dilantin) after suffering two more generalized tonic-clonic seizures. The patient was prepped and transported to Maine Medical Center for further evaluation and management.
At Maine Medical Center, the patient was admitted to the special care unit and started on standard therapy for diabetic ketoacidosis. Upon review of his chart, a family history significant for cardiovascular disease was found. Medications include: metformin, metoprolol, lisinopril, glipizide, hydrochlorothiazide, colchicine, allopurinol, atorvastatin calcium (Lipitor), indomethhacin, and hydralazine. The patient has no known drug allergies. He was somnolent and staff was unable to assess orientation due to his critically ill appearance.
After stabilization and extubation, the patient developed chest pressure and pain. The electrocardiogram (ECG) showed no ST-elevations. Cardiac biomarkers were cycled and positive (CK: 515, CK-MB: 31, troponin: 3.39). Other significant labs to note are WBC: 13.0, BUN: 30, creatinine: 1.70, and glucose: 467. The patient was taken for diagnostic testing in radiology and cardiology.
Diagnostic results
12-Lead ECG: Sinus tachycardia with left atrial enlargement and insignificant Q-waves in the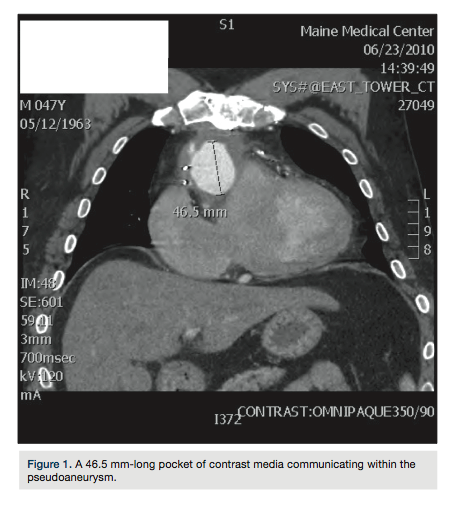 inferior leads.
inferior leads.
Cardiac cath: Severe native coronary artery disease. Left main trunk and left anterior descending artery disease appeared worse than in 2006. Saphenous vein graft to the first diagonal branch was occluded. Saphenous vein graft to the posterior descending artery was widely patent. The posterior descending to posterolateral segments were flush occluded. A large ascending aortic pseudoaneurysm was visualized. Left ventricular systolic function was below normal.
CT-chest: Trace bilateral pleural effusions. Large pseudoaneurysm of the ascending thoracic aorta measuring 7.1 x 8.9 x 6.7 cm (Figures 1-3).
Echocardiogram: Nondilated, concentrically hypertrophied left ventricle with segmental apical,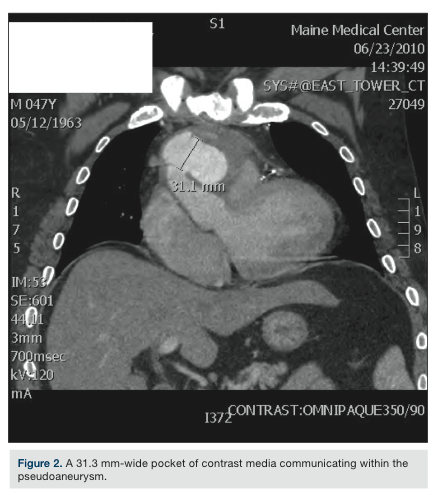 apical lateral, and anteroapical hypokinesis; left ventricular ejection fraction is estimated at 45-50%. Left atrial enlargement. Mild tricuspid regurgitation with estimated pulmonary artery systolic pressure = 47 mmHg. At least moderate pulmonic stenosis with a peak instantaneous gradient of 42 mmHg.
apical lateral, and anteroapical hypokinesis; left ventricular ejection fraction is estimated at 45-50%. Left atrial enlargement. Mild tricuspid regurgitation with estimated pulmonary artery systolic pressure = 47 mmHg. At least moderate pulmonic stenosis with a peak instantaneous gradient of 42 mmHg.
Therapeutic intervention
After the findings, a cardiothoracic surgical consult was obtained. The patient was taken to the operating room three days after first presentation (6/20/2010) and underwent redo sternotomy with circulatory arrest for repair of a complex pseudoaneurysm arising from the ascending aorta. The pseudoaneurysm was dissected and found to contain a purulent infection. A bovine patch was grafted over the surgically corrected area. Cultures demonstrated a copious Aspergillus infection. Aspergillus is a fungus whose spores are found normally in the air. Aspergillus does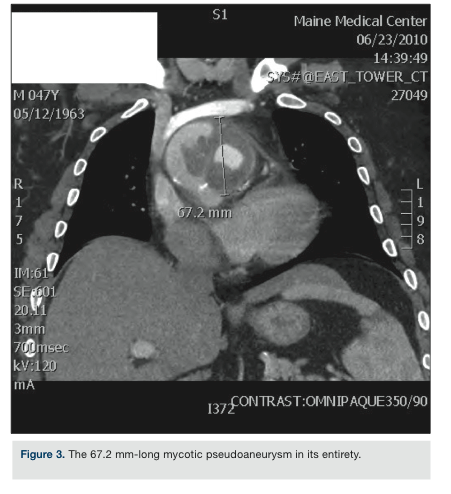 not normally cause infections in healthy individuals.
not normally cause infections in healthy individuals.
The patient had a prolonged and difficult postoperative course requiring mechanical circulatory support for 5 days. Ultimately, the patient was weaned off support, the chest was closed, and the patient was extubated. His recovery was slow, but steady. He had also developed an Aspergillus infection involving his right eye. He was closely followed throughout his hospitalization by critical care medicine, infectious disease, neurology, cardiology, and ophthalmology. By 08/01/2010, the patient was ambulating in the hall independently on room air with stable hemodynamics. He completed a 28-day course of IV amphotericin for his Aspergillus infection, and later he was converted to oral voriconazole. The recommendation from infectious disease is that he continues oral suppression for the remainder of his life.
Discussion
Ascending aortic root pseudoaneurysms are an uncommon complication of coronary artery bypass grafting surgery. The mechanism of formation of such a pseudoaneurysm may be purely idiopathic, but certainly may be initiated by disruption of the natural anatomy of the aorta during cannulation and anastomosis of a vein graft. Moreover, poorly controlled diabetes and the propensity for associated Aspergillus infection went on to complicate our patient’s pseudoaneurysm. In this case, uncontrolled diabetes allowed for an immunocompromised state and the Aspergillus fungal infection spread systemically, infecting his vasculature and right eye. What was possibly a subclinical and asymptomatic out-pouching of the ascending aorta at the site of the vein graft anastomosis rapidly progressed to a mycotic pseudoaneurysm, causing hemodynamic instability.
Disclosures: The authors report no conflicts of interest regarding the content herein.
This article received a double-blind peer review from members of the Cath Lab Digest editorial board.
The authors may be contacted via Matthew Kirk, BSRS, RT(R), RCIS, at gsxeddie@yahoo.com.
References
- Cotran R, Kumar V, Collins T, eds. Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, PA: WB Saunders Co., 1999.
- Prech M, Grajek S, Cieśliński A, Jemielity M. Mycotic aneurysm of the ascending aorta following CABG. Heart. 2000 Jan; 83(1): E3.
- Cooley DA, Burnett CM. Fungal infection in a dissecting aneurysm of the thoracic aorta. Tex Heart Inst J. 1993; 20(1): 51-54.
