


Acute Myocardial Infarction in a 21-Year-Old Male Due to Essential Thombocytosis
Introduction
The pathophysiology of acute myocardial infarction (MI) often involves acute plaque rupture that results in platelet recruitment, aggregation and thrombosis. Most often this occurs in patients with predisposing risk factors such as hypertension, dyslipidemia, and diabetes mellitus. However, there are rare instances when an acute MI occurs in patients with no obvious risk factors and no predilection to develop coronary artery thrombosis. One such condition that has rarely been documented in literature is essential thrombocytosis. Also known as essential thrombocythemia, this is a rare primary myeloproliferative disorder in which there is clonal thrombocytosis resulting in increased risk of thomboembolic phenomena and hemorrhagic phenomena. Herein, we report a case of a 21-year-old previously healthy male who presented with an acute anterior MI with a large thrombus in the left main coronary artery that was emergently and successfully aspirated manually during primary percutaneous coronary intervention. Studies revealed the presence of essential thrombocytosis with a JAK2 (Janus associated kinase-2) mutation. He is now being treated for essential thrombocytosis to prevent future recurrences. A close review of the literature revealed approximately 30 such cases of acute MI related to essential thrombocytosis, involving
results in platelet recruitment, aggregation and thrombosis. Most often this occurs in patients with predisposing risk factors such as hypertension, dyslipidemia, and diabetes mellitus. However, there are rare instances when an acute MI occurs in patients with no obvious risk factors and no predilection to develop coronary artery thrombosis. One such condition that has rarely been documented in literature is essential thrombocytosis. Also known as essential thrombocythemia, this is a rare primary myeloproliferative disorder in which there is clonal thrombocytosis resulting in increased risk of thomboembolic phenomena and hemorrhagic phenomena. Herein, we report a case of a 21-year-old previously healthy male who presented with an acute anterior MI with a large thrombus in the left main coronary artery that was emergently and successfully aspirated manually during primary percutaneous coronary intervention. Studies revealed the presence of essential thrombocytosis with a JAK2 (Janus associated kinase-2) mutation. He is now being treated for essential thrombocytosis to prevent future recurrences. A close review of the literature revealed approximately 30 such cases of acute MI related to essential thrombocytosis, involving typically elderly patients with multiple risk factors for coronary artery disease. However, this is the first report involving a young individual with confirmed JAK2 mutation to support the diagnosis.
typically elderly patients with multiple risk factors for coronary artery disease. However, this is the first report involving a young individual with confirmed JAK2 mutation to support the diagnosis.
Case report
A 21-year-old male patient presented to the emergency room via ambulance with a 20-minute history of severe retrosternal chest pain. He was playing a game of football and after 30 minutes of play, had developed sudden onset of severe chest pain associated with left upper arm numbness. The patient was taken to a nearby fire station, at which time an electrocardiogram (ECG) was performed, revealing ST segment elevation in leads V1-V6 with reciprocal depressions in the inferior leads (Figure 1), suggestive of an anterolateral MI. Upon initial evaluation, the patient appeared hemodynamically stable, with a blood pressure of 143/88 mmHg and heart rate of 95 beats per minute. He was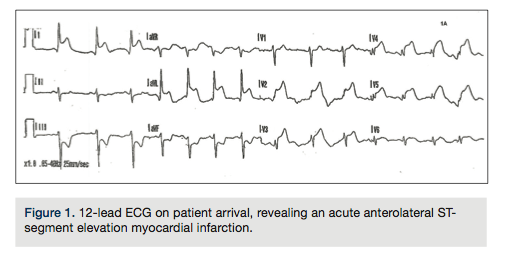 immediately transferred to the nearest emergency room within 10 minutes. Further questioning demonstrated no prior illicit drug abuse, chest trauma, or any risk factors for underlying coronary artery disease, such as smoking, hypertension, dyslipidemia, or family history of early coronary artery disease.
immediately transferred to the nearest emergency room within 10 minutes. Further questioning demonstrated no prior illicit drug abuse, chest trauma, or any risk factors for underlying coronary artery disease, such as smoking, hypertension, dyslipidemia, or family history of early coronary artery disease.
Given his initial presentation, despite the absence of significant risk factors for coronary disease, he was emergently taken up for cardiac catheterization. Angiography revealed a large thrombus in the large-caliber distal left main coronary artery (LM) and smaller thrombi were noted in the distal left anterior descending (LAD), mid diagonal branch of the LAD, and distal left circumflex artery (LCx) (Figure 2). The distal thrombi were thought to be embolic fragments from the large thrombus in the LM coronary artery. The right coronary artery was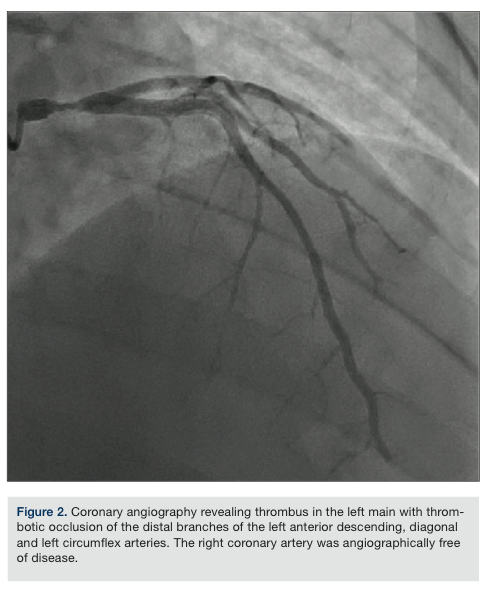 dominant and its branches were angiographically free of disease.
dominant and its branches were angiographically free of disease.
To revascularize the left coronary system, a 7 French (Fr) XB 3.5 guide catheter (Cordis) was used to selectively engage the LM coronary artery. A Pronto V3 catheter system (Vascular Solutions) was used to successfully aspirate the thrombus manually. Anticoagulation was achieved with intravenous bivalirudin and adjuvant intracoronary abciximab. The patient’s chest pain was completely ameliorated once a significant portion of thrombus in the LM coronary artery was aspirated and we achieved excellent angiographic results after repeated passes with the manual aspiration catheter (Figure 3). The thrombus fragments in the distal LCx were successfully aspirated using the Pronto LP system and fragments of thrombus in the diagonal branch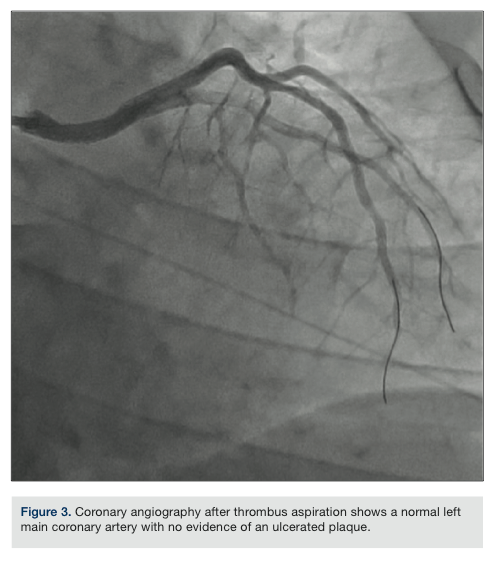 resolved, with adequate flow restored down these vessels. Coronary flow to the distal LAD, however, was not restored, despite balloon angioplasty and attempts to aspirate thrombus manually with the Pronto LP system. No stents were deployed, because there was no evidence of atherosclerotic stenosis after thrombus aspiration. Left ventriculogram showed a low normal left ventricular ejection fraction (LVEF) of 50% with hypokinesis involving the apical segment of the left ventricle.
resolved, with adequate flow restored down these vessels. Coronary flow to the distal LAD, however, was not restored, despite balloon angioplasty and attempts to aspirate thrombus manually with the Pronto LP system. No stents were deployed, because there was no evidence of atherosclerotic stenosis after thrombus aspiration. Left ventriculogram showed a low normal left ventricular ejection fraction (LVEF) of 50% with hypokinesis involving the apical segment of the left ventricle.
Intravenous abciximab that was started during the procedure was continued for a total of 24 hours, in addition to dual antiplatelet therapy with aspirin and prasugrel. The patient was brought back to the cardiac catheterization lab after 36 hours for a follow-up left heart catheterization that revealed normal coronaries, except for the previously noted occluded distal LAD.
Laboratory work drawn at initial presentation in the emergency room was reported around the time the cardiac catheterization was completed. It demonstrated an elevated white blood cell (WBC) count of 18,600 per µL without obvious shift and significantly elevated platelet count at 723,000 per µL, while other parameters were within normal limits. His basic metabolic profile and urine drug screen showed no significant abnormalities. Initial troponin was elevated at 67, with significantly elevated cardiac isoenzymes.
Given the significantly elevated platelet count and elevated WBC count with no sign of infection, a hematology consult was obtained for further guidance. The patient underwent an extensive hematological evaluation, including laboratory tests for hypercoagulable states (protein C, protein S, antithrombin III, factor V leiden mutation, anticardiolipin antibody, lupus anticoagulant and homocysteine levels), JAK2 mutation analysis, BCR-ABL PCR, and finally, a peripheral smear to help explain the sudden onset of thrombosis in an otherwise healthy individual. All of the above-mentioned laboratory studies were normal, but the patient tested positive for the JAK2 V16F mutated DNA. The peripheral smear demonstrated thrombocytosis with occasional giant platelets, suggestive of a chronic myeloproliferative disorder. Bone marrow aspirate and biopsy confirmed the presence of essential thrombocytosis and ruled out other marrow disorders.
The patient was discharged on day 4 of hospitalization, and placed on dual antiplatelet therapy with aspirin and prasugrel, in addition to carvedilol, rosuvastatin, and hydroxyurea. One month following his presentation, the patient remained compliant on his medication, with routine blood work revealing a stable platelet count of 420,000 per µL and an echocardiogram showing an LVEF of 55 with apical hypokinesis. The patient continues to receive regular follow-up.
Discussion
Thrombocytosis, defined as an increase in the platelet count greater than 600,000 per µl, can have a variety of etiologies, and is usually subdivided into primary and secondary causes, with the latter group being more benign in its course. Essential, or primary thrombocytosis, however, is a chronic myeloproliferative disorder, characterized by the overproduction of platelets by megakaryocytes in the bone marrow, in the absence of an alternative cause. This condition classically affects the middle age to elderly population, with an average age of 50-60 years; however, cases have been reported in the younger population.1 Essential thrombocytosis is very rarely diagnosed, with an incidence rate of 2-3 per 100,000 individuals annually.2 Revised criteria used to diagnose this condition include the presence of a persistently elevated platelet count > 450,000 per µL associated with acquired V617F JAK2 mutation, in the absence of alternative causes such as iron deficiency anemia, chronic myeloid leukemia, polycythemia vera, and other myeloproliferative disorders.3
Essential thrombocytosis usually presents with vasomotor symptoms or with complications related to thrombosis or bleeding, with 25-33% of patients being asymptomatic. Thrombosis can manifest in either the arterial or venous circulation, with the former occurring around 75% of the time.4 One such cohort, examining 100 patients, detailed the overall risk of thrombotic events in essential thrombocytosis, including conditions such as myocardial infarction, stroke, pulmonary embolism, deep vein thrombosis, transient ischemic attack, retinal artery or venous occlusions, hepatic or portal vein thrombosis, and digital ischemia, to be 6.6% per patient per year in comparison to 1.2% per patient per year in the control population.5 The specific incidence of myocardial infarction in this population has been difficult to identify, as it has only been sparingly documented by isolated case reports over the past two decades.
As mentioned earlier, diagnosis is often incidental and suspected in patients with persistent yet unexplained increase in the number of platelets in whom other myeloproliferative disorders have been ruled out. Some patients may also present with normal platelet counts where subsequent bone marrow examination and positive clonality markers might be indicative of diagnosis.6 Peripheral blood smear may demonstrate immature precursor cells and large platelets (thrombocytes). Approximately half of patients with essential thrombocytosis also manifest the JAK2 V617F mutation that is associated with increased granulocyte and reticulocyte precursor, in addition to megakaryocytic hyperplasia in the bone marrow.7 Platelet function studies such as PT, PTT and bleeding times are usually within reference ranges; however, platelet aggregation studies are often abnormal.8 A German study chronicling 61 patients with essential thrombocytosis detailed an > 80% incidence of spontaneous platelet aggregation9, which one can consider as the culprit mechanism in acute coronary thrombosis in the otherwise healthy patient. Douste-Blazy et al in 1984 reported that pathophysiologic mechanisms of thrombus formation in different coronary arteries in patients with essential thrombocytosis were possibly due to activation of thrombocytes as a result of endothelial damage, extended arterial spasms, increased procoagulant activity of thrombocytes, changes in glycoproteins on the surface of thrombocytes, and possible deficiency of selective lipoxygenase.10
Usual risk factors for coronary artery disease such as hypertension, diabetes, tobacco abuse, etc., also affect patients with essential thrombocytosis, often increasing their risk for thrombosis. Previous studies have shown a strong correlation between thromboembolic complications of essential thrombocytosis in patients with increased blood pressure and cigarette smoking habits.11 A recent study examining a cohort of patients with essential thrombocytosis at Mayo Clinic before 1992 identified predictors of increased mortality and thrombosis risk as increased age > 60 years, previous thrombotic episodes, leukocytosis, diabetes mellitus, and tobacco abuse. In view of this relationship, studies have shown that with aggressive risk factor control in patients known to have essential thrombocytosis, recurrent thromboembolic risk can be substantially reduced.10
In the acute setting, our patient underwent intracoronary thrombus aspiration and angioplasty in the left main coronary artery and its branches, including the LAD and LCx, with good results. For the longer term, although specific treatment regimens have not been clearly identified in this subset of patients and outcomes are not known, the goal of therapy has remained the same. Multiple studies have documented the need to reduce the overall platelet count, and for dual antiplatelet therapy and risk factor modification.12 A review of the literature sparingly details the use of conventional therapies, such as a combination of platelet anti-aggregating medications including aspirin, glycoprotein IIb/IIIa inhibitors, and clopidogrel with anticoagulants such as heparin and bivalirudin during initial treatment for the acute event, with either percutaneous intervention or emergent coronary artery bypass grafting.13 Newer antiplatelet drugs, including prasugrel and ticagrelor, have yet to be used in such patients. It is not clear if antiplatelet medications can be discontinued if platelet counts are maintained below 450,000 per µL. Long-term treatment modalities to reduce platelet counts include the use of hydroxyurea, anagrelide, and alpha interferon.14 Harrison et al reported in 2005 that patients treated with low-dose aspirin and hydroxyurea experienced decreased rates of arterial thrombosis and hemorrhage compared to those with anagrelide and aspirin.15 A recently introduced JAK 1 and JAK 2 inhibitor, ruxolitinib, (Jakafi, Incyte Corp.) has also been gaining increasing prominence in the literature as another therapeutic modality for treatment of chronic myeloproliferative disorders like essential thrombocytosis, polycythemia vera, and myelofibrosis, but this therapy needs to be closely monitored for potentially serious side effects.16
Conclusion
This case report illustrates the importance of seeking and addressing alternate etiologies to an acute myocardial infarction in the absence of clearly defined risk factors, especially in the younger population. The underlying etiology, in this case, essential thrombocytosis, may warrant indefinite monitoring and appropriate treatment, because complications can potentially be fatal.
Disclosure: The authors report no conflicts of interest regarding the content herein.
This article received a double-blind peer review from members of the Cath Lab Digest Editorial Board.
The authors can be contacted via Venkataramanan Gangadharan, MD, at venkat.gangadharan@gmail.com.
References
- Hoffman R, Benz E, Furie B, Sanford S. Essential Thrombocythemia. Hematology: Basic Principles and Practice. 5th ed. London, United Kingdom: Churchill Livingstone (Elsevier); 2008: Chapter 71.
- Mesa R, Silverstein M, Jacobsen S, Wollan P, Tefferi A. Population-based incidence and survival figures in essential thrombocythemia and agnogenic myeloid metaplasia: an Olmsted County Study, 1976-1995. Am J Hematol. 1999; 61(1): 10-15.
- Murphy S, Peterson P, Iland H, Laszlo J. Experience of the Polycythemia Vera Study Group with essential thrombocythemia: a final report on diagnostic criteria, survival and leukemic transition by treatment. Semin Hematol. 1997; 34: 29-39.
- Blann A, Caine G, Bareford D. Abnormal vascular, platelet and coagulation markers in primary thrombocythaemia are not reversed by treatments that reduce the platelet count. Platelets. 2004; 15: 447-449.
- Cortelazzo S, Viero P, Finazzi G, D’Emilio A, Rodeghiero F, Barbui T. Incidence and risk factors for thrombotic complications in a historical cohort of 100 patients with essential thrombocythemia. J Clin Oncol. 1990; 8: 556-562.
- Mercier E, Cochery-Nouvellon E, Lavigne G, Bertinchant J-P, Gris J-C. In support of the revised World Health Organization diagnostic criteria for essential thrombocythemia: JAK2V617F and premature myocardial infarction. J Thromb Haemost. 2008; 6: 206-207.
- Spanoudakis E, Margaritis D, Kotsianidis I, Georgiou G, Tripsianis G, Anastasiadis A, Karakolios A, Pantelidou D, Panayiotidis P, Bourikas G, Tsatalas C. Long-term bone marrow cultures (LTBMC) from essential thrombocythemia (ET) patients with or without JAK2617V>F mutation. Leuk Res. 2008; 32(10): 1593-1596.
- Gugliotta L, Marchioli R, Fiacchini M, et al. Epidemiological, diagnostic, therapeutic and prognostic aspects of essential thrombocythemia in a retrospective study of the GIMMC group in two thousand patients [abstract]. Blood. 1997; 90(Suppl 1): 348a.
- Hehlmann R, Jahn M, Baumann B, Köpcke W. Essential thrombocythemia: clinical characteristics and course of 61 cases. Cancer. 1988; 61(12): 2487-2496.
- Douste-Blazy P, Taudou MJ, Delay M, Pris J, Sie P, Ribaut L, Ribaut L, Galinier F, Bernadet P. Essential thrombocythaemia and recurrent myocardial infarction. Lancet. 1984; 2: 992.
- Rossi C, Randi ML, Zervinati P, Rinaldi V, Girolami A. Acute coronary disease in essential thrombocythemia and polycythemia vera. J Intern Med. 1998; 244: 49-53.
- Young-Hyo Lim, Young Yiu Lee, Jae Hoon Kim et al. Development of acute myocardial infarction in a young female patient with essential thrombocythemia treated with anagrelide: a case report. Korean J of Hematol 2010; 45: 136-138.
- Watanabe T, Fujinaga H, Ikeda Y, Higashi T, Murakami M, et al. Acute myocardial infarction in a patient with essential thrombocythemia who underwent successful stenting: A case report. Angiology. 2005; 56(6): 771-774.
- Gisslinger H, Chott A, Scheithauer W, Gilly B, Linkesch W, Ludwig H. Interferon in essential thrombocythaemia. Br J Haematol. 1991; 79(Suppl 1): 42-7.
- Harrison CN, Campbell PJ, Buck G, Wheatley K, East CL, Bareford D, Wilkins BS, van der Walt JD, Reilly JT, Grigg AP, Revell P, Woodcock BE, Green AR. Hydroxyurea compared with anagrelide in high-risk essential thrombocythemia. N Engl J Med. 2005; 353(1): 33-45.
- Tefferi A, Litzow M, Pardanani A. Long-term outcome of treatment with ruxolitinib in myelofibrosis. N Engl J Med. 2011; 365: 1455-1457.
