


An Absent Right Coronary Artery Anomaly
Abstract: The presence of a single coronary artery supplying the entire myocardium is an unusual anomaly. Congenital coronary anomalies are found in 0.2-1.6% of the population undergoing diagnostic coronary angiography.6,8 Most coronary anomalies described in the literature are cases in which the origin of a given coronary artery is anomalous, but very few cases describe the complete agenesis of the ostium of one coronary artery. The presence of a single coronary artery may predispose an afflicted patient to angina, myocardial infarction, congestive heart failure or even sudden cardiac death, especially if this anomaly is compounded by atherosclerotic disease. This case describes a single coronary artery originating from the left sinus of Valsalva with a dominant left circumflex artery continuing distally into the right side of the heart, filling the right coronary artery from the distal end retrograde.
Case report
 A 54-year-old man with a past medical history significant for hypertension, diabetes mellitus and hyperlipidemia was referred to the cardiology clinic for evaluation of unstable angina, fatigue, shortness of breath after climbing one flight of stairs, and swollen ankles. His home medications include lisinopril 5mg once daily, glipizide 2.5mg once daily, amlodipine 5mg once daily, felodipine 25mg once daily and aspirin 81mg daily. The patient has a family history of coronary artery disease and a 75-pack year history of tobacco use. Initial physical
A 54-year-old man with a past medical history significant for hypertension, diabetes mellitus and hyperlipidemia was referred to the cardiology clinic for evaluation of unstable angina, fatigue, shortness of breath after climbing one flight of stairs, and swollen ankles. His home medications include lisinopril 5mg once daily, glipizide 2.5mg once daily, amlodipine 5mg once daily, felodipine 25mg once daily and aspirin 81mg daily. The patient has a family history of coronary artery disease and a 75-pack year history of tobacco use. Initial physical 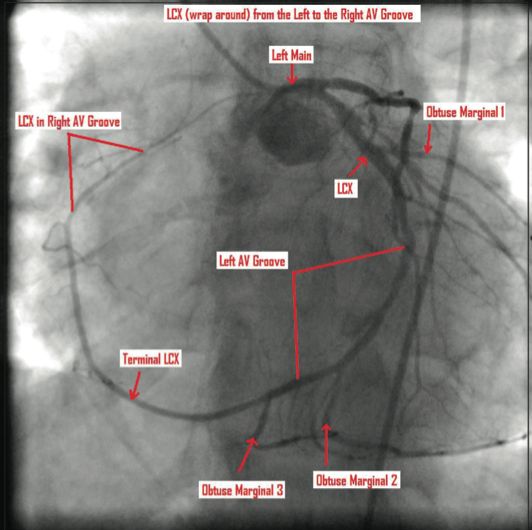 examination revealed a blood pressure of 133/75 mmHg, a heart rate of 62 beats per minute, and was otherwise unremarkable. An ECG revealed a normal sinus rhythm with no evidence of ischemic changes. A persantine stress was also unremarkable for ischemic changes by ECG criteria and electrocardiographic evidence. A two-dimensional echocardiogram revealed a sinus rhythm with extrasystolic beats, an impaired diastolic filling pattern, mild tricuspid regurgitation and an ejection fraction between 60-65%. To further evaluate this
examination revealed a blood pressure of 133/75 mmHg, a heart rate of 62 beats per minute, and was otherwise unremarkable. An ECG revealed a normal sinus rhythm with no evidence of ischemic changes. A persantine stress was also unremarkable for ischemic changes by ECG criteria and electrocardiographic evidence. A two-dimensional echocardiogram revealed a sinus rhythm with extrasystolic beats, an impaired diastolic filling pattern, mild tricuspid regurgitation and an ejection fraction between 60-65%. To further evaluate this  patient’s unstable angina, a cardiac catheterization with selective coronary angiography was performed.
patient’s unstable angina, a cardiac catheterization with selective coronary angiography was performed.
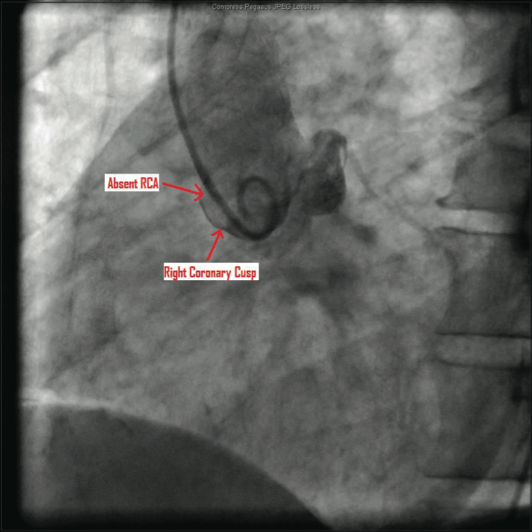
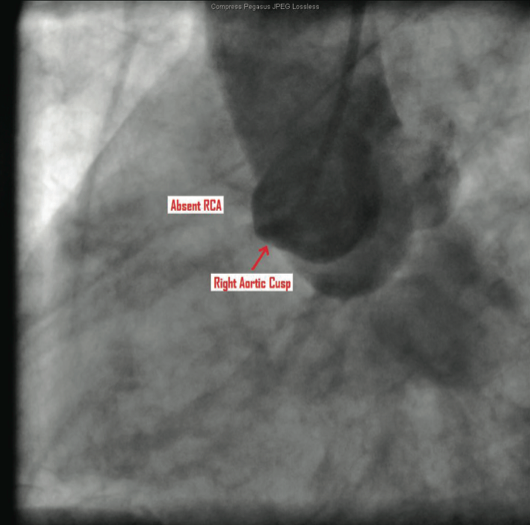
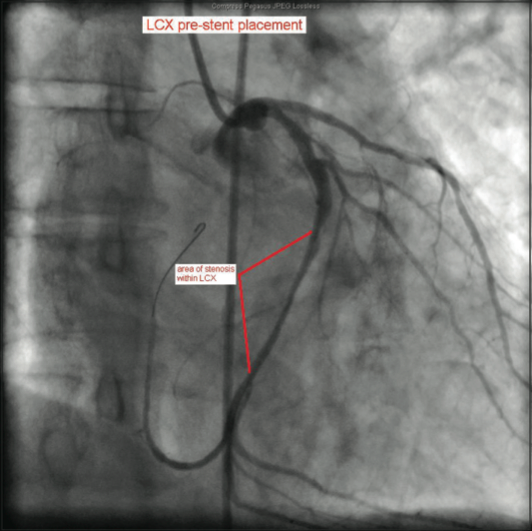
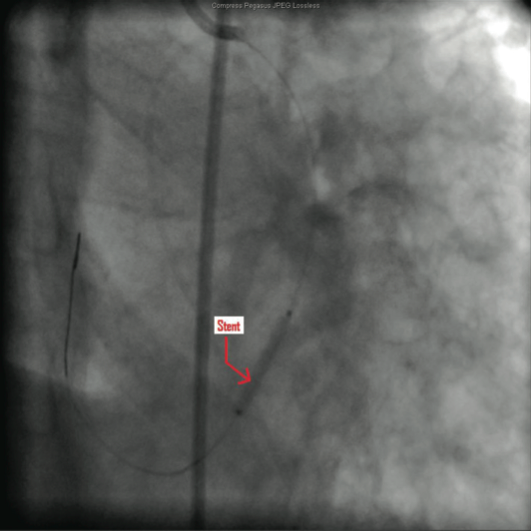
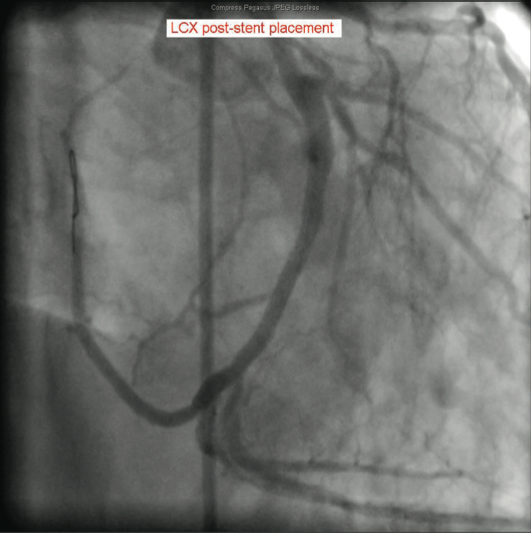
The catheterization and angiogram showed a patent left main coronary artery that bifurcated into the left anterior descending (LAD) and the left circumflex (LCX). The LAD had a mid 50% stenosis and the LCX was a large-sized vessel that gave off three obtuse marginal (OM) branches and continued distally into the right 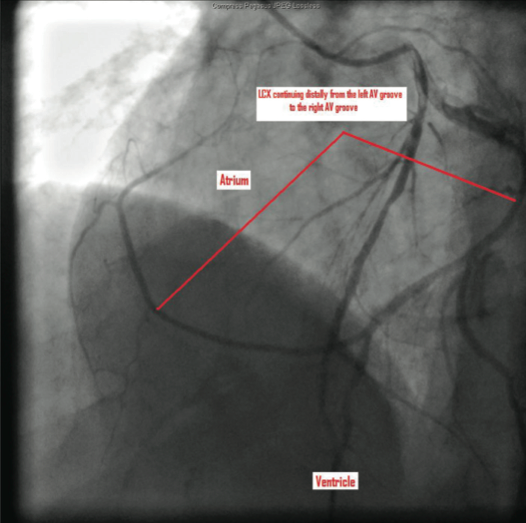 side of the heart, filling the right coronary artery (RCA) from the distal end retrograde. The LCX had a mid 70-80% lesion that was confirmed by intravascular ultrasound (IVUS). The right coronary artery had no ostium and received retrograde filling via the LCX, continuing distally into the right myocardium. The LCX 80% mid stenosis was successfully revascularized with deployment of two drug-eluting stents. The patient was placed on post-procedure clopidogrel, simvastatin, beta blockers, and nitroglycerin.
side of the heart, filling the right coronary artery (RCA) from the distal end retrograde. The LCX had a mid 70-80% lesion that was confirmed by intravascular ultrasound (IVUS). The right coronary artery had no ostium and received retrograde filling via the LCX, continuing distally into the right myocardium. The LCX 80% mid stenosis was successfully revascularized with deployment of two drug-eluting stents. The patient was placed on post-procedure clopidogrel, simvastatin, beta blockers, and nitroglycerin.
Discussion
 The congenital absence of a single coronary ostium is a rare finding in patients undergoing cardiac catheterization, with an incidence of 0.024%-0.066%.1,2 The anomalous origin of the right coronary artery from sites such as the left main stem and the pulmonary trunk has been previously described in the literature.3-5 However, a search of the literature for the agenesis of the right coronary ostium with continuation of the left circumflex artery into the right region of the heart yielded very few case reports.
The congenital absence of a single coronary ostium is a rare finding in patients undergoing cardiac catheterization, with an incidence of 0.024%-0.066%.1,2 The anomalous origin of the right coronary artery from sites such as the left main stem and the pulmonary trunk has been previously described in the literature.3-5 However, a search of the literature for the agenesis of the right coronary ostium with continuation of the left circumflex artery into the right region of the heart yielded very few case reports.
 According to Lipton et al, classification of coronary anomalies depends on the origin and anatomical course of the coronary arteries relative to the ascending aorta and pulmonary trunk. Type L represents a RCA originating from the left main stem and type R represents a coronary artery originating from the RCA ostium. These types are then classified as I to III. Class I follows either the anatomical course of either the LCA or RCA. Class II represents one coronary artery arising from the proximal part of the opposite coronary artery. In class III, the left anterior
According to Lipton et al, classification of coronary anomalies depends on the origin and anatomical course of the coronary arteries relative to the ascending aorta and pulmonary trunk. Type L represents a RCA originating from the left main stem and type R represents a coronary artery originating from the RCA ostium. These types are then classified as I to III. Class I follows either the anatomical course of either the LCA or RCA. Class II represents one coronary artery arising from the proximal part of the opposite coronary artery. In class III, the left anterior 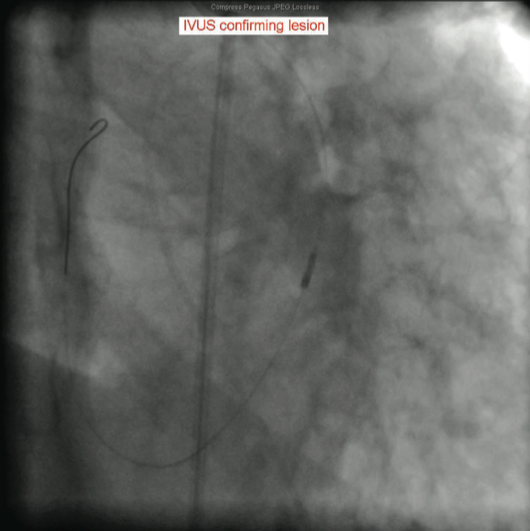 descending and left circumflex arteries arise separately from the proximal part of a normal RCA. Classes II and III are then designated as anterior (type A) or posterior (type P) according to their route in relation to the pulmonary artery, or inter-arterial (type B) if it courses between the ascending aorta and pulmonary trunk.9,10 The patient we describe does not fit into any of these categories, as his single coronary artery originated from the left sinus of Valsalva and subsequently gave off the LAD, LCX and the LCX merely continued distally to supply the right region of the myocardium.
descending and left circumflex arteries arise separately from the proximal part of a normal RCA. Classes II and III are then designated as anterior (type A) or posterior (type P) according to their route in relation to the pulmonary artery, or inter-arterial (type B) if it courses between the ascending aorta and pulmonary trunk.9,10 The patient we describe does not fit into any of these categories, as his single coronary artery originated from the left sinus of Valsalva and subsequently gave off the LAD, LCX and the LCX merely continued distally to supply the right region of the myocardium.
 Identification of coronary anomalies usually occurs during coronary angiography. Depending on the origin, course, termination and the presence atherosclerosis, coronary anomalies may result in syncope, myocardial infarction, cardiomyopathy, sudden cardiac death, or may be asymptomatic. In our particular case, the patient had a rare congenital anomaly of the RCA that was not evident on ECG, two-dimensional echocardiogram, or persantine stress test. Given the atherosclerotic changes described in the patient’s coronary arteries above, the results of these diagnostic tests can be attributed to false negatives.
Identification of coronary anomalies usually occurs during coronary angiography. Depending on the origin, course, termination and the presence atherosclerosis, coronary anomalies may result in syncope, myocardial infarction, cardiomyopathy, sudden cardiac death, or may be asymptomatic. In our particular case, the patient had a rare congenital anomaly of the RCA that was not evident on ECG, two-dimensional echocardiogram, or persantine stress test. Given the atherosclerotic changes described in the patient’s coronary arteries above, the results of these diagnostic tests can be attributed to false negatives.
 This case demonstrates the importance of evaluating recurrent episodes of unstable angina in patients with multiple risk factors for coronary artery disease despite non-specific diagnostic test results. Based on this case, one can make an argument in favor of the aggressive management of patients with risk factors for coronary artery disease that are referred to outpatient cardiology clinics for the evaluation of unstable angina, despite unremarkable test results. This patient’s initial cardiac work-up showed no specific evidence of ischemic heart
This case demonstrates the importance of evaluating recurrent episodes of unstable angina in patients with multiple risk factors for coronary artery disease despite non-specific diagnostic test results. Based on this case, one can make an argument in favor of the aggressive management of patients with risk factors for coronary artery disease that are referred to outpatient cardiology clinics for the evaluation of unstable angina, despite unremarkable test results. This patient’s initial cardiac work-up showed no specific evidence of ischemic heart 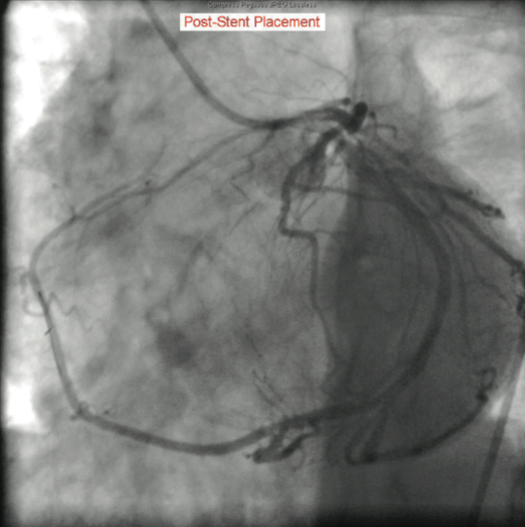 disease, yet the choice to proceed with cardiac catheterization proved wise, as this patient had significant atherosclerosis of his coronary arteries. The cardiac catheterization and subsequent deployment of drug-eluting stents may potentially save this clinically symptomatic, yet diagnostically unremarkable, patient from a future myocardial infarction or even sudden cardiac death.
disease, yet the choice to proceed with cardiac catheterization proved wise, as this patient had significant atherosclerosis of his coronary arteries. The cardiac catheterization and subsequent deployment of drug-eluting stents may potentially save this clinically symptomatic, yet diagnostically unremarkable, patient from a future myocardial infarction or even sudden cardiac death.
The authors can be contacted via Roba Alhasan at ralhasan@med.wayne.edu.
This article received a double-blind peer review from members of the Cath Lab Digest Editorial Board.
References
- Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J, de Geest H. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992;13(12):1637-1640.
- Harindhanavudhi T, Tanawuttiwat T, Trivedi D. Anomalous single coronary artery with absent right coronary artery diagnosed with the aid of 64-slice multidetector computed tomographic angiography. Tex Heart Inst J. 2009; 36(4): 362–363.
- W C Kang, S H Han, T H Ahn, E K Shin. Unusual dominant course of left circumflex coronary artery with absent right coronary artery. Heart. 2006 May; 92(5): 657.
- Sanyal K, Satija B, Katyayni K. Malignant anomalous right coronary artery detected by multidetector row computed tomography coronary angiography. J Cardiovasc Dis Res. 2012 Jan; 3(1): 40-42.
- Jo Y, Uranaka Y, Iwaki H, Matsumoto J, Koura T, Negishi K. Sudden cardiac arrest: associated with anomalous origin of the right coronary artery from the left main coronary artery. Tex Heart Inst J. 2011; 38(5): 539-543.
- Babb J, Miller M, Shammas R. Single left coronary artery with origin of the right coronary artery from distal circumflex. Clin Cardiol. 2001; 24: 90-92.
- Dixit DP, Gohil DV, Pandya AM, Patel MP. A study of incidence of single coronary artery. Int J Biol Med Res. 2012; 3(1): 1348-1350.
- Ugalde H, Ramírez A, Ugalde D, Farías E, Silva AM. Coronary artery origin anomalies. Analysis of 10.000 coronary angiographies. Rev Med Chil. 2010 Jan;138(1):7-14.
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979; 130: 39-47.
- Gleeson T, Thiessen R, Wood D, Mayo JR. Single coronary artery from the right aortic sinus of Valsalva with anomalous prepulmonic course of the left coronary artery. Can J Cardiol. 2009 April; 25(4): e136-e138.
