Utilization of the Jetstream Navitus L for CTO Crossing and Debulking
Disclosure: Orlando Marrero reports no conflicts of interest regarding the content herein. Dr. Van Crisco reports he is on the speakers bureau for St. Jude Medical and AstraZeneca, and is a consultant for Cook Medical. Orlando Marrero can be contacted at  orlm8597@yahoo.com. Dr. Crisco can be contacted at drcrisco@firstcoastheart.com.
orlm8597@yahoo.com. Dr. Crisco can be contacted at drcrisco@firstcoastheart.com.
Case report
A 46-year-old female presented with a non-healing wound on the right foot. Duplex ultrasound suggested an occluded distal right superficial femoral artery (SFA). Single leg right lower extremity arteriogram runoff revealed the 100% occlusion in the distal right SFA before Hunter’s canal (Figure 1), mild atherosclerotic disease in the right profunda femoris, and 3-vessel runoff to the right foot. The occluded segment appeared to be moderately calcified proximally and the plaque heterogeneous in nature.

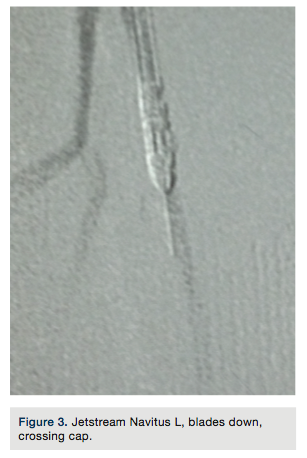
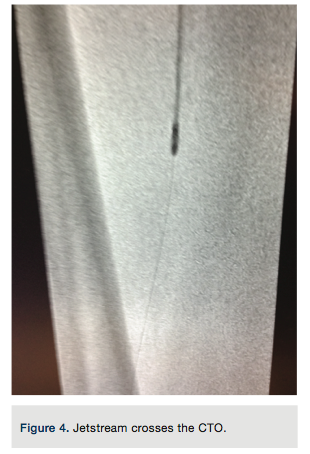
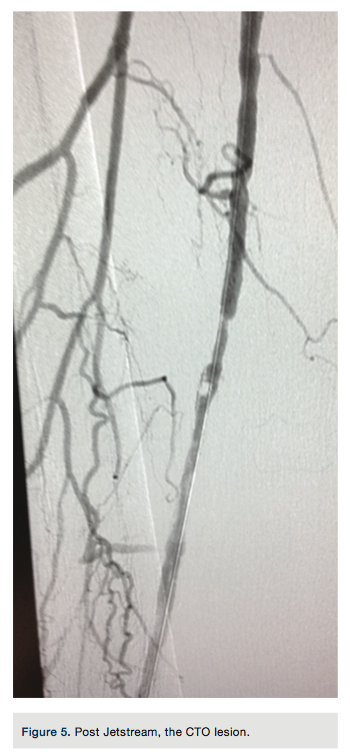
A 7 French x 65 cm Pinnacle Destination sheath (Terumo) was advanced where the tip was placed in the mid right SFA. Systemic anticoagulation with heparin was given and the patient had been pretreated with aspirin and clopidogrel. Standard chronic totalocclusion (CTO) crossing techniques were used to try to gain access across the 100% occluded distal right SFA beginning with a 0.0350-inch Minnie Support Catheter (Vascular Solutions, Inc) and a soft, angled Glidewire (Terumo). Failure to cross prompted advancing to a stiff, angled Glidewire (Terumo), and then a Hi-Torque Supracore 0.035-inch Support Wire (Abbbott Vascular) within the support catheter. Escalation in wire stiffness resulted in inability to pierce the proximal cap. A Frontrunner Catheter (Cordis) was used unsuccessfully in a further attempt to cross (Figure 2). Finally, a 2.4 to 3.4 mm Jetstream Navitus L (Bayer Interventional) debulking atherectomy device was advanced to the proximal cap of the lesion over a Spartacore 0.014-inch long guide wire (Abbott Vascular), with the distal flexible tip of the guide wire excised and its blunt, firm tip protruding out of the tip of the Jetstream catheter. The blunt, sharp wire tip was imbedded into the proximal CTO cap and the Jetstream Navitus was activated with the blades down to enter the lesion. After crossing the proximal cap, the atherectomy device was removed and the Frontrunner catheter crossed the CTO segment, allowing us 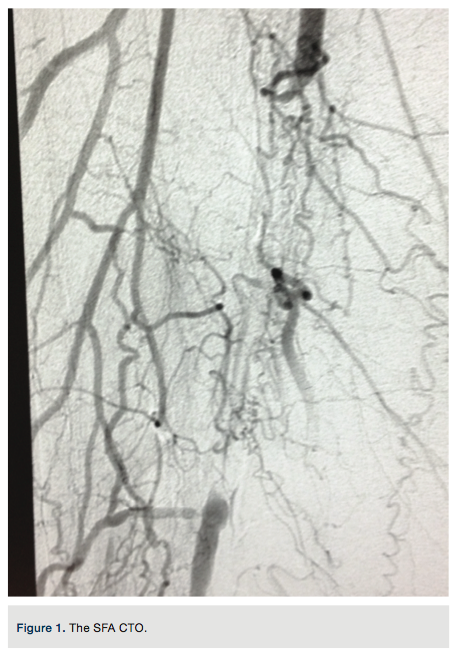 to gain purchase in the distal vessel within the true lumen. Placement was confirmed with a hand injection angiogram into the popliteal artery. There was no evidence of dissection. Routine debulking atherectomy was performed with the Jetstream Navitus 2.4 to 0.4 mm device with blades down (Figure 3) and blades up across the occluded segment (Figures 4-5) over the Spartacore wire. Balloon dilation was then performed with 5.0 x 80 mm and 6.0 x 80 mm Chocolate balloons (Trieme Medical)
to gain purchase in the distal vessel within the true lumen. Placement was confirmed with a hand injection angiogram into the popliteal artery. There was no evidence of dissection. Routine debulking atherectomy was performed with the Jetstream Navitus 2.4 to 0.4 mm device with blades down (Figure 3) and blades up across the occluded segment (Figures 4-5) over the Spartacore wire. Balloon dilation was then performed with 5.0 x 80 mm and 6.0 x 80 mm Chocolate balloons (Trieme Medical)
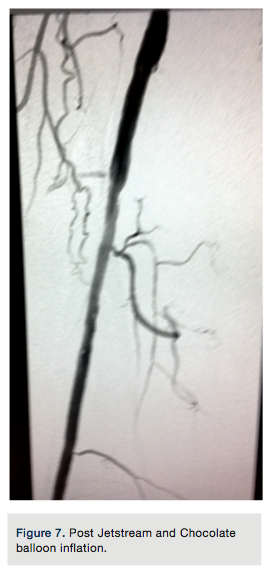
(Figure6). There was an excellent angiographic result (Figure 7). The final angiographic image showed a -10% residual stenosis and brisk flow distally, with no dissection or extravasation of contrast. A pullback gradient assessment of femoral and popliteal artery to the proximal right SFA was performed and no gradient found. The Pinnacle Destination sheath was removed and a Perclose (Abbott Vascular) technique was used for left common femoral artery vascular access closure.
Discussion
Antegrade wire escalation inside a crossing catheter is a common CTO crossing technique used in peripheral intervention. The above case represents a common series of crossing wires with accelerating stiffness to cross a CTO, with ultimate advancement to a dedicated crossing catheter, the (Cordis) Frontrunner, which was also used without success.
Having performed direct SFA CTO crossings using the Jetstream Navitus L device (Bayer Interventional), both within stents and native vessels, we felt it was a reasonable option in this case for several reasons. Our goal when crossing a CTO is to always try to
remain luminal, which keeps safe debulking atherectomy an acceptable lesion-modifying strategy. We feel luminal crossing also decreases the likelihood that an endovascular scaffold, such as a stent, is needed to maintain vessel patency. Ultimately, we feel a luminal approach reduces the risk of stent-related, long-term events such as in-stent restenosis, further atherectomy or covered stents, and the need for vascular bypass surgery. It also provides a relatively quick way to address safe CTO crossing, with little downside.
We used a blunt Spartacore 0.014-inch guidewire with the flexible tip removed (with wire cutters) to stabilize the Jetstream atherectomy device by advancing the wire tip into the proximal cap of the CTO. Device activation modifies the proximal cap to facilitate wire crossing or advancement of the atherectomy device itself. A blunt-tipped wire in front of the atherectomy tip can reduce the likelihood of the device veering into a sub-intimal space. The Jetstream’s differential blade design pushes elastic
tissue away from the advancing edge and has a distinct rpm change if a sub-intimal track is taken. If a perforation should occur in an already occluded area, there is little eminent risk to the patient in the distal SFA, although this risk is high in other vascular segments where compartment syndromes can occur. If successful, using the Jetstream as a crossing device also allows for immediate atherectomy with no additional cost. Many vessels approached in this manner ultimately reveal both a proximal and distal cap structure amenable to atherectomy, and often a somewhat healthier vessel in-between. This can be appreciated by the free-swinging vibratory imaging of the Jetstream atherectomy tip between caps, which becomes stabilized whena more complex lesion is engaged. Although off-label, use of the Jetstream Navitus as a crossing device for proximal cap access seems a safe and reasonable strategy when typical crossing strategies fail to engage the proximal cap of an SFA CTO.
]