


Use of Excimer Laser to Facilitate CTO Crossing Complicated by Stent Fracture

 Stent fracture secondary to percutaneous coronary intervention (PCI) can be asymptomatic, but studies have shown that it can result in thrombosis or in-stent restenosis (ISR), which can subsequently lead to further angina, myocardial infarction (MI), or possible sudden death.1 Excimer laser coronary atherectomy (ELCA) is indicated for chronic occlusions, stent under-expansion, ISR, and uncrossable lesions. Here, we will discuss the use of ELCA for an uncrossable obstruction due to stent fracture and ISR. While not a formal indication of this modality, ELCA will be explored as a possible treatment option for this type of complication. To the best of our knowledge, this is the first reported case of coronary artery stent fracture and uncrossable ISR successfully treated with ELCA.
Stent fracture secondary to percutaneous coronary intervention (PCI) can be asymptomatic, but studies have shown that it can result in thrombosis or in-stent restenosis (ISR), which can subsequently lead to further angina, myocardial infarction (MI), or possible sudden death.1 Excimer laser coronary atherectomy (ELCA) is indicated for chronic occlusions, stent under-expansion, ISR, and uncrossable lesions. Here, we will discuss the use of ELCA for an uncrossable obstruction due to stent fracture and ISR. While not a formal indication of this modality, ELCA will be explored as a possible treatment option for this type of complication. To the best of our knowledge, this is the first reported case of coronary artery stent fracture and uncrossable ISR successfully treated with ELCA.
Case Report
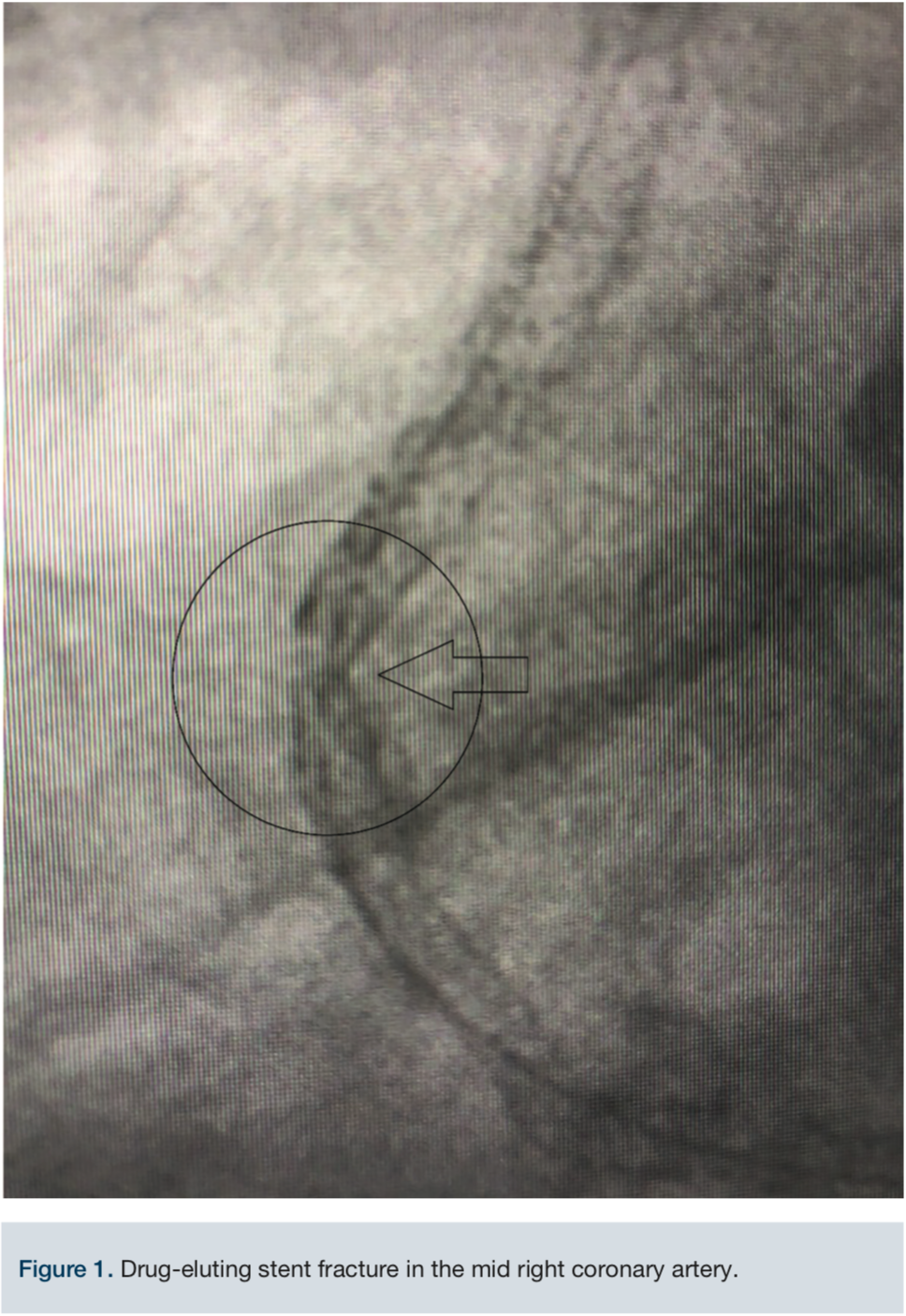 A 68-year-old male was referred to our center for intractable chest pain after a failed intervention to treat ISR of the proximal to mid right coronary artery (RCA) two months prior. The referring cardiologist requested a second opinion and possible Rotoblator (Boston Scientific) rotational atherectomy. After reviewing the case, we determined atherectomy using Rotoblator of the area was contraindicated in view of a stent fracture (Figure 1). It was felt that ELCA (Philips) would give us the safest and best possible outcome, if successful.
A 68-year-old male was referred to our center for intractable chest pain after a failed intervention to treat ISR of the proximal to mid right coronary artery (RCA) two months prior. The referring cardiologist requested a second opinion and possible Rotoblator (Boston Scientific) rotational atherectomy. After reviewing the case, we determined atherectomy using Rotoblator of the area was contraindicated in view of a stent fracture (Figure 1). It was felt that ELCA (Philips) would give us the safest and best possible outcome, if successful.
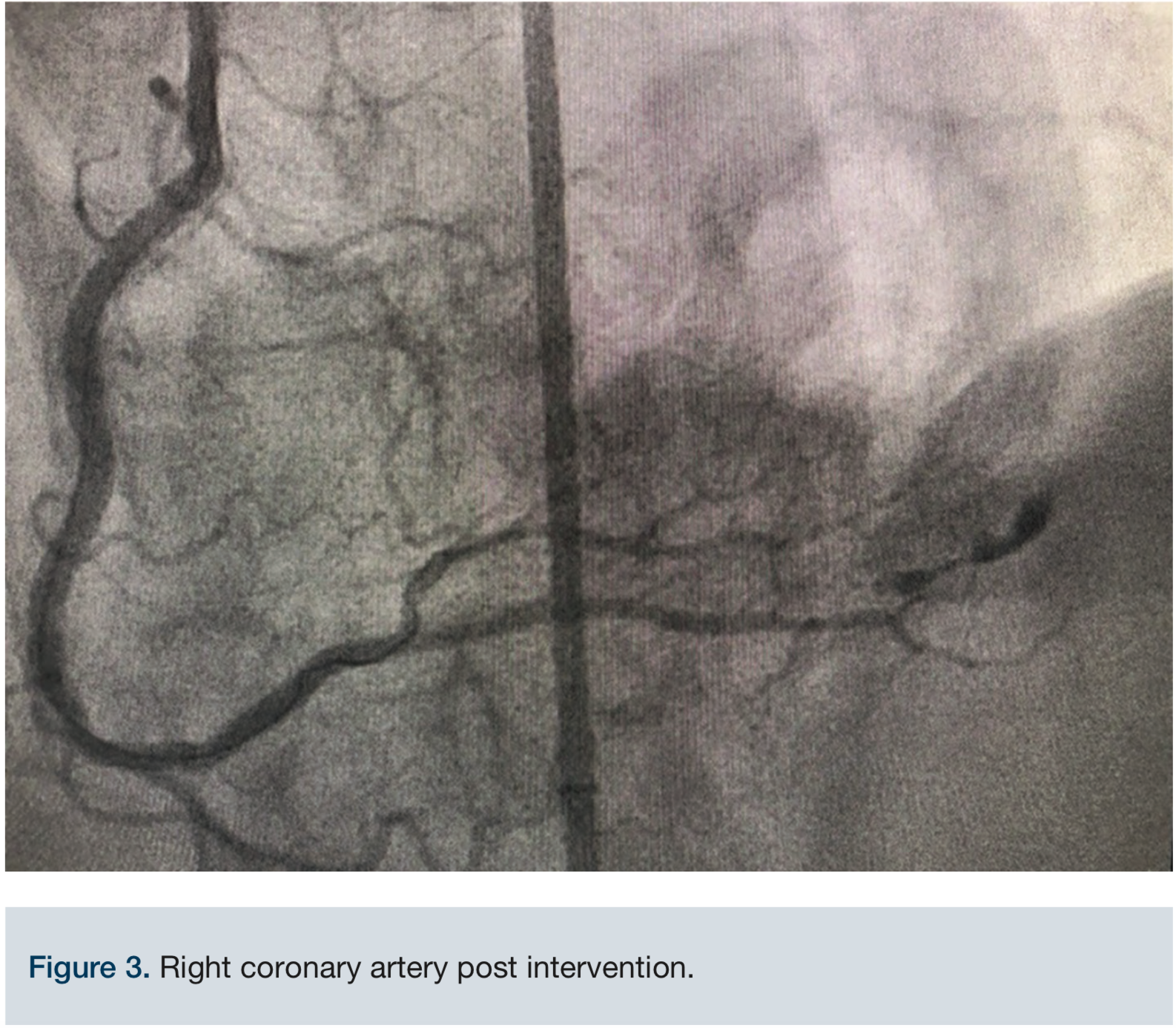
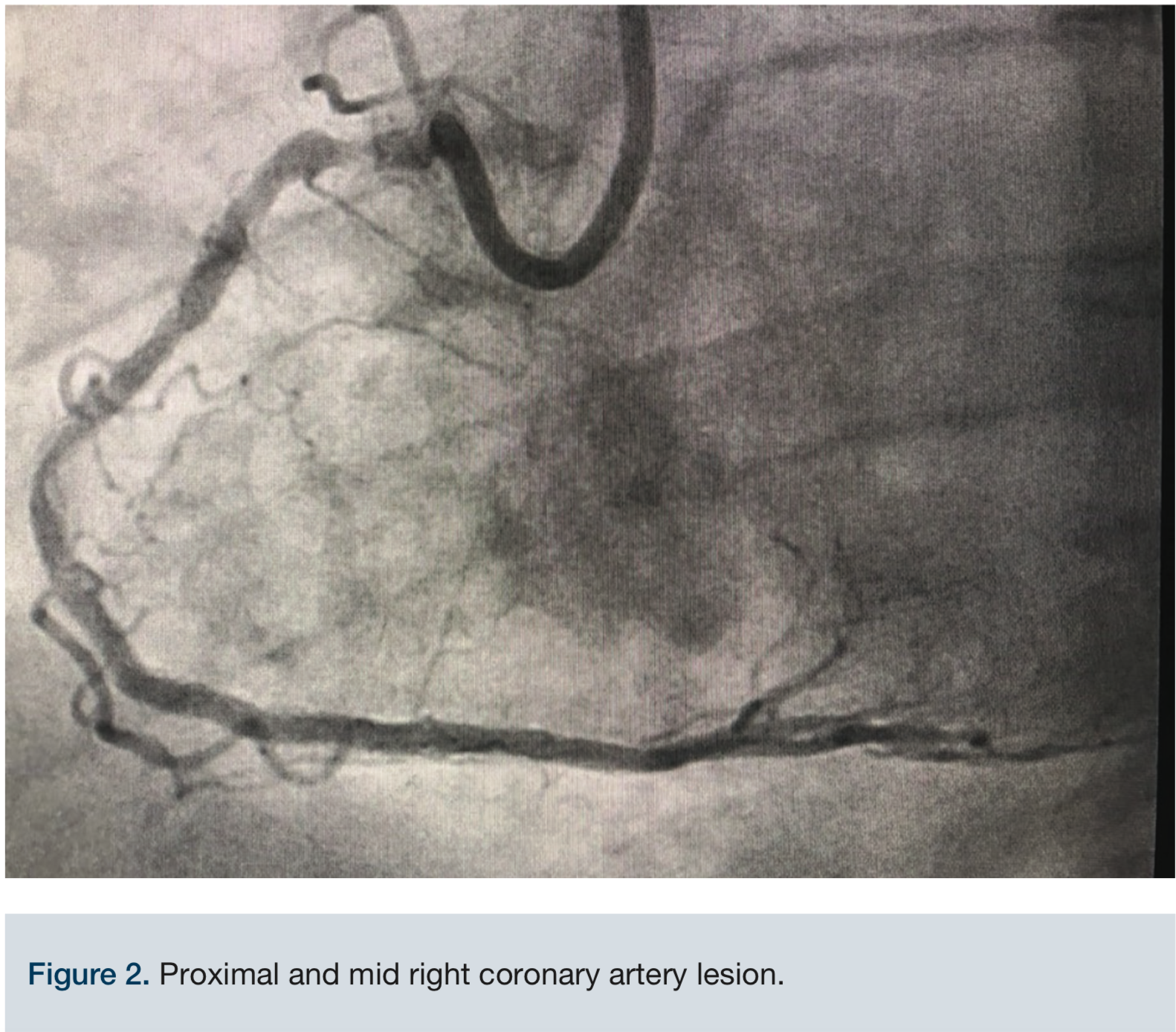 Access was obtained via the right common femoral artery. The initial lesion in the mid proximal RCA can be seen in Figure 2. An 8 French (Fr) long Destination sheath (Terumo) was used for maximum support, and a 0.75 Amplatz left (AL) 2 Guide catheter (Boston Scientific) was used for access support and assistance. A Balance Middleweight (BMW) wire (Abbott Vascular) was initially used to advance the catheter into the target artery. We switched to a 300 cm PT choice wire (Boston Scientific) in an attempt to cross the existing stent lumen, with the use of a 6 Fr Guideliner (Teleflex) for additional support. A 2.5 mm x 12 mm balloon (Medtronic) failed to cross the mid RCA stent fracture and ISR. The two markers on the balloon created a too-large catheter diameter, so a 1.25 mm x 12 mm single marker balloon (Medtronic) was chosen instead and successfully crossed. The balloon was inflated to 20 atmospheres (atm) and removed. A second attempt to pass the original 2.5 mm x 12 mm balloon (Medtronic) once again failed. The ELCA catheter was positioned just proximal to the mid RCA ISR within the fractured stent lumen. We started with an 0.9 laser catheter with the tip terminating just proximal to the ISR. An initial fluence of 45 mJ/mm2 was applied and gradually increased to a fluence of 80 mJ/mm2 for a total of almost 5 minutes while the tip was still positioned proximally to the ISR. The laser then was able to advance through the obstruction and was removed. Over the wire, a 2.5 mm x 12 mm balloon was inflated up to 20 atm for 25 seconds and then replaced with a 3.0 mm x 20 mm balloon (Medtronic) inflated to nominal pressure. The same 3.0 mm balloon was used at the very proximal aspect of the ISR as a pre-dilation before two drug-eluting stents (DES) were placed: a 3.0 mm x 18 mm Onyx DES (Medtronic) at the mid RCA and a second 3.0 mm x 30 mm Onyx DES at the proximal to mid RCA. The 3.0 mm x 18 mm Onyx DES stent was deployed at 22 atm for 15 seconds and the 3.0 mm x 30 mm Onyx DES was deployed 20 atm for 10 seconds. Post stent deployment, angiography clearly demonstrated reduction of the stenosis from approximately 99% to <10% at the site of the original stenosis in the proximal to mid RCA. At the end of the procedure, Thrombolysis In Myocardial Infarction (TIMI)-III flow was achieved (Figure 3). Inline flow was successfully restored across the entire RCA. The procedure was uncomplicated, but required the use of significant amounts of contrast (500 mL) and fluoroscopy (81.1 minutes). The patient was discharged the following day without incident, and has thus far remained asymptomatic throughout his follow-up with his referring cardiologist.
Access was obtained via the right common femoral artery. The initial lesion in the mid proximal RCA can be seen in Figure 2. An 8 French (Fr) long Destination sheath (Terumo) was used for maximum support, and a 0.75 Amplatz left (AL) 2 Guide catheter (Boston Scientific) was used for access support and assistance. A Balance Middleweight (BMW) wire (Abbott Vascular) was initially used to advance the catheter into the target artery. We switched to a 300 cm PT choice wire (Boston Scientific) in an attempt to cross the existing stent lumen, with the use of a 6 Fr Guideliner (Teleflex) for additional support. A 2.5 mm x 12 mm balloon (Medtronic) failed to cross the mid RCA stent fracture and ISR. The two markers on the balloon created a too-large catheter diameter, so a 1.25 mm x 12 mm single marker balloon (Medtronic) was chosen instead and successfully crossed. The balloon was inflated to 20 atmospheres (atm) and removed. A second attempt to pass the original 2.5 mm x 12 mm balloon (Medtronic) once again failed. The ELCA catheter was positioned just proximal to the mid RCA ISR within the fractured stent lumen. We started with an 0.9 laser catheter with the tip terminating just proximal to the ISR. An initial fluence of 45 mJ/mm2 was applied and gradually increased to a fluence of 80 mJ/mm2 for a total of almost 5 minutes while the tip was still positioned proximally to the ISR. The laser then was able to advance through the obstruction and was removed. Over the wire, a 2.5 mm x 12 mm balloon was inflated up to 20 atm for 25 seconds and then replaced with a 3.0 mm x 20 mm balloon (Medtronic) inflated to nominal pressure. The same 3.0 mm balloon was used at the very proximal aspect of the ISR as a pre-dilation before two drug-eluting stents (DES) were placed: a 3.0 mm x 18 mm Onyx DES (Medtronic) at the mid RCA and a second 3.0 mm x 30 mm Onyx DES at the proximal to mid RCA. The 3.0 mm x 18 mm Onyx DES stent was deployed at 22 atm for 15 seconds and the 3.0 mm x 30 mm Onyx DES was deployed 20 atm for 10 seconds. Post stent deployment, angiography clearly demonstrated reduction of the stenosis from approximately 99% to <10% at the site of the original stenosis in the proximal to mid RCA. At the end of the procedure, Thrombolysis In Myocardial Infarction (TIMI)-III flow was achieved (Figure 3). Inline flow was successfully restored across the entire RCA. The procedure was uncomplicated, but required the use of significant amounts of contrast (500 mL) and fluoroscopy (81.1 minutes). The patient was discharged the following day without incident, and has thus far remained asymptomatic throughout his follow-up with his referring cardiologist.
Discussion
 Excimer laser coronary atherectomy was first approved for coronary intervention in the United States in 1983, with its use becoming increasingly prevalent over the past 10-15 years. The excimer laser is comprised of pulsed gases, acting as a medium to create short wavelength, high energy pulses of ultraviolet (UV) light. The depth of laser penetration is directly correlated to its wavelength.2 Advancements have occurred over the years to help improve the safety and efficacy of ELCA. Risks do exist, including perforation, clotting, and possible myocardial infarction, however the occurrence of such is relatively rare.4 An interventionalist at our institution (Jost) has performed over 500 cardiac laser atherectomy procedures with only a single perforation, due to the pre-dilation balloon prior to placing the stent. The patient outcome was excellent. There are several indications for the use of ELCA, including:
Excimer laser coronary atherectomy was first approved for coronary intervention in the United States in 1983, with its use becoming increasingly prevalent over the past 10-15 years. The excimer laser is comprised of pulsed gases, acting as a medium to create short wavelength, high energy pulses of ultraviolet (UV) light. The depth of laser penetration is directly correlated to its wavelength.2 Advancements have occurred over the years to help improve the safety and efficacy of ELCA. Risks do exist, including perforation, clotting, and possible myocardial infarction, however the occurrence of such is relatively rare.4 An interventionalist at our institution (Jost) has performed over 500 cardiac laser atherectomy procedures with only a single perforation, due to the pre-dilation balloon prior to placing the stent. The patient outcome was excellent. There are several indications for the use of ELCA, including:
- Occluded saphenous vein bypass grafts;
- Ostial lesions;
- Long lesions (>20 mm in length);
- Moderately calcified stenosis;
- Total occlusions traversable by a guidewire;
- Lesions which previously failed balloon angioplasty;
- Restenosis in 316L stainless steel stents, prior to the administration of intravascular brachytherapy.3
Risks are low, but include perforation, clotting, and myocardial infarction.4
Relative contraindications include:
- Lesion in an unprotected left main artery;
- Lesion beyond acute bends or in a location within the coronary anatomy where the catheter cannot traverse;
- Guidewire cannot be passed through the lesion;
- Lesion is located within a bifurcation;
- Patient is not an acceptable candidate for bypass graft surgery.3
The first case report of coronary stent fracture was described in 2004.5 The conventional treatment for stent fracture and ISR varies between solitary medical treatment, balloon angioplasty, and re-stenting using DES.6 High-energy excimer laser has been used to treat coronary ISR in an underexpanded stent not amenable to high-pressure balloon angioplasty.2 Latib and Colombo describe the use of ELCA to modify the plaque by using contrast injection to further improve stent underexpansion in undilatable stented lesions.7 This laser “explosion” technique was previously described by Nicola Viceconte.8 While rotational atherectomy is a relative contraindication for ISR and underexpanded stents, this modality of treatment has been used at times with success.7 In our case, the stent fracture led to symptomatic and severe ISR, and as an uncrossable/undilatable obstruction, was a contraindication for rotational or orbital atherectomy. The prolonged use of focal and proximal ELCA treatment, leading to the maximum fluence of 80 mJ/mm2, was instrumental in plaque modification that permitted the passing of a larger balloon at high pressure and finally, a DES. This collective procedural approach significantly reduced the ISR, satisfactorily treated and resolved the coronary stent obstruction, and restored adequate blood flow through the coronary vessels, with the expectation of excellent long-term patency.
References and Further Reading
- Mohsen MK, Alqahtani A, Al suwaidi J. Stent fracture: how frequently is it recognized? Heart Views. 2013 Apr-Jun; 14(2): 72-81. doi: [10.4103/1995-705X.115501]
- Noble S, Bilodeau, L. High energy excimer laser to treat coronary in-stent restenosis in an underexpanded stent. Catheter Cardiovasc Interv. 2008 May 1; 71(6): 803-807. doi: 10.1002/ccd.21490.
- Rawlins J, Din JN, Talwar S, O’Kane P. Coronary intervention with the excimer laser: review of the technology and outcome data. Interv Cardiol. 2016 May; 11(1): 27-32. doi: 10.15420/icr.2016:2:2.
- Nishino M, Mori N, Takiuchi S, et al. Indications and outcomes of excimer laser coronary atherectomy: Efficacy and safety for thrombotic lesions-The ULTRAMAN registry. J Cardiol. 2017 Jan; 69(1): 314-319. doi: 10.1016/j.jjcc.2016.05.018.
- Sianos G, Hofma S, Ligthart JM, et al. Stent fracture and restenosis in the drug-eluting stent era. Catheter Cardiovasc Interv. 2004; 61(1): 111-116.
- Lee SE, Jeong MH, Kim IS, et al. Clinical outcomes and optimal treatment for stent fracture after drug-eluting stent implantation. J Cardiol. 2009; 53(3):422-428.
- Ferri LA, Jabbour RJ, Giannini F, et al. Safety and efficacy of rotational atherectomy for the treatment of undilatable underexpanded stents implanted in calcific lesions. Catheter Cardiovasc Interv. 2017; 90: E19-E24.
- Viceconte N, Biscione C, Tarsia G, et al. Laser “explosion” technique for treatment of unexpanded coronary stent. Int J Cardiol. 2011 Jun 16; 149(3): 395-387. doi: 10.1016/j.ijcard.2011.03.021.
- Stone GW, Reifart NJ, Moussa I, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part II. Circulation. 2005; 112: 2530-2537.
- Dash D. Interventional management of “balloon-uncrossable” coronary chronic total occlusion: is there any way out? Korean Circ J. 2018 Apr; 48(4): 277-286. doi: 10.4070/kcj.2017.0345.
- Ino Y, Toyoda Y, Tanaka A , et al. Predictors and prognosis of stent fracture after sirolimus-eluting stent implantation. Circ J. 2009; 73(11): 2036-2041.
- Chinikar M, Sadeghipour P. Coronary stent fracture: a recently appreciated phenomenon with clinical relevance. Curr Cardiol Rev. 2014 Nov; 10(4): 349-354.
Disclosure: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Kyle Macdonald, BS, at kmacdonald@swcva.com.
