


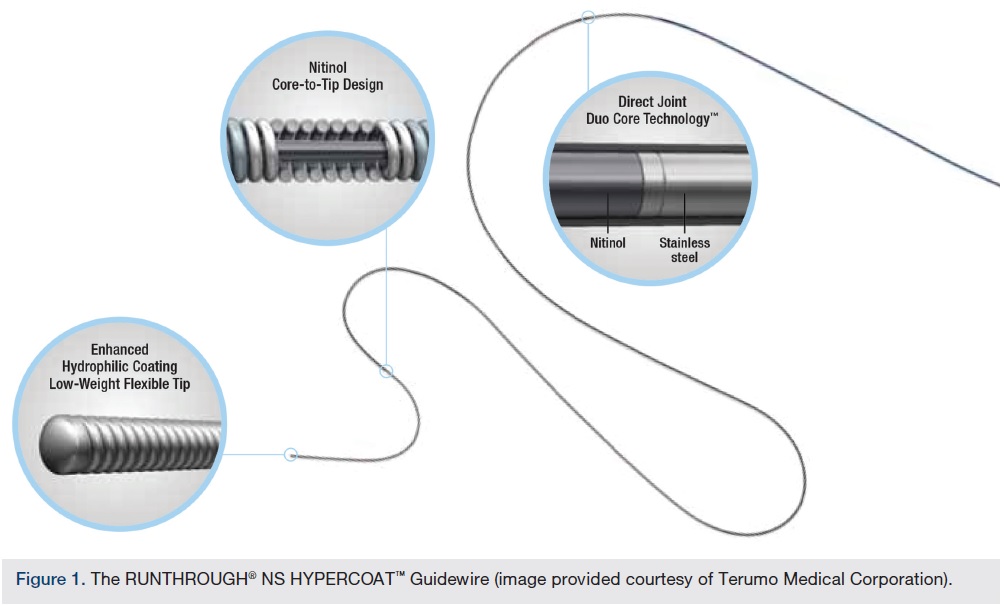
Terumo Coronary Guidewires – RUNTHROUGH® NS EXTRA FLOPPY is Joined by RUNTHROUGH® NS HYPERCOAT™
Can you describe your practice and the types of procedures you do?
 I am an interventional cardiologist and I practice out of St. Petersburg, Florida, primarily at St. Anthony’s Hospital. I do coronary, peripheral, and complex endovascular intervention, and have spearheaded the move to transradial complex coronary interventions as well as transradial use in ST-elevation myocardial infarction (STEMI) intervention here in St. Petersburg.
I am an interventional cardiologist and I practice out of St. Petersburg, Florida, primarily at St. Anthony’s Hospital. I do coronary, peripheral, and complex endovascular intervention, and have spearheaded the move to transradial complex coronary interventions as well as transradial use in ST-elevation myocardial infarction (STEMI) intervention here in St. Petersburg.
Percutaneous transluminal coronary angioplasty (PTCA) wires are very important to an interventional cardiologist. Tell us about your experience with the RUNTHROUGH NS Extra floppy coronary “workhorse” wire.
 The RUNTHROUGH Extra Floppy Guidewire was my workhorse wire before I started using the RUNTHROUGH Hypercoat Guidewire and now I am at about a 50:50 use between the two wires. In fellowship, your attendings introduce you to a lot of different wires, and at University Hospital in Cincinnati, as well as at Banner Good Samaritan Hospital where I trained, the Balance Middle Weight (BMW) (Abbott Vascular), as well as the Asahi Prowater wire (Abbott Vascular), are popular wires. Both are very commonly used workhorse wires and perform well. But with the RUNTHROUGH Extra Floppy Guidewire, I noticed the tip could withstand numerous interventions and did not deform very much. I also experienced a better tactile response with the RUNTHROUGH Extra Floppy Guidewire. I don’t use a torquor (a device that is attached to the wire to help the operator manipulate the wire); I generally use “feel” in my fingers to manipulate the wire, and I get a much better tactile feel with the RUNTHROUGH Extra Floppy Guidewire than I did with the BMW or the Prowater. Among these wires, I feel the RUNTHROUGH Extra Floppy Guidewire has the best blend as far as tensile strength of the wire, ability to cross lesions, and tip durability.
The RUNTHROUGH Extra Floppy Guidewire was my workhorse wire before I started using the RUNTHROUGH Hypercoat Guidewire and now I am at about a 50:50 use between the two wires. In fellowship, your attendings introduce you to a lot of different wires, and at University Hospital in Cincinnati, as well as at Banner Good Samaritan Hospital where I trained, the Balance Middle Weight (BMW) (Abbott Vascular), as well as the Asahi Prowater wire (Abbott Vascular), are popular wires. Both are very commonly used workhorse wires and perform well. But with the RUNTHROUGH Extra Floppy Guidewire, I noticed the tip could withstand numerous interventions and did not deform very much. I also experienced a better tactile response with the RUNTHROUGH Extra Floppy Guidewire. I don’t use a torquor (a device that is attached to the wire to help the operator manipulate the wire); I generally use “feel” in my fingers to manipulate the wire, and I get a much better tactile feel with the RUNTHROUGH Extra Floppy Guidewire than I did with the BMW or the Prowater. Among these wires, I feel the RUNTHROUGH Extra Floppy Guidewire has the best blend as far as tensile strength of the wire, ability to cross lesions, and tip durability.
You recently started using the new RUNTHROUGH Hypercoat coronary specialty wire. Why did you adopt this wire over other specialty wires for complex lesions?
I use the RUNTHROUGH Hypercoat Guidewire in situations when I would typically reach for a hydrophilic, polymer-jacketed wire. Hydrophilic wires, primarily wires like the Choice PT Extra Support (Boston Scientific) or Whisper wire family (Abbott Vascular), have a reputation for finding any and all channels, which leads to worry about distal wire perforations or wire trauma. When treating a distal lesion, if you are taking the wire out very far, or if there is any degree of difficulty advancing a wire or stent through the lesion, the back and forth of the wire can cause a wire trauma or wire perforation. With the RUNTHROUGH Hypercoat Guidewire, the wire works in a manner similar to a hydrophilic wire, yet prolapses very easily and then is able to go into very distal parts of vessels without causing worry that you are going to create a wire perforation or wire trauma. It is a very good wire to cross a very tight lesion, because once you have crossed, you have the ability to prolapse it and extend the wire distally. It is an ideal wire for that situation.
When are you using the RUNTHROUGH Hypercoat Guidewire?
Highly stenosed lesions, so very tight, 95-99% lesions with reduced TIMI grade flow, situations where I typically reach for a PT2, Choice PT Extra Support, or a Whisper wire, are situations where I now go first to the RUNTHROUGH Hypercoat Guidewire. When the lesion is in the middle portion of the vessel, I prefer to take my wire out very far to get wire support, so I will also use a RUNTHROUGH Hypercoat Guidewire in that scenario, with the intention of prolapsing the wire and placing it very far out into the vessel.
You discussed some of the concerns with hydrophilic wires. Is there a tradeoff between performance and safety with specialty wires?
You do often exchange safety for performance with some hydrophilic wires, because crossing a heavily calcified or highly stenosed lesion requires a highly lubricious wire. These types of lesions might not be navigable by a non-hydrophilic wire. Once you have crossed, a very hydrophilic wire is apt to take very small channels and can potentially cause wire trauma or perforations further down in the distal vascular bed, which makes using it as a workhorse wire a little more dangerous. If you are having trouble crossing a lesion and you know that the tip of the wire is going to be going back and forth as you are advancing and exchanging equipment, then a hydrophilic wire becoming the workhorse is a worry, because of issues with wire perforation and distal vascular injury. With the RUNTHROUGH Hypercoat Guidewire, you can cross the lesion, so it gives you the performance, and in terms of safety, you are able to advance the wire out distally with less worry about wire trauma or vascular perforation. It is a nice, unique feature of the wire. In my opinion, you don’t sacrifice safety for performance.
After crossing a lesion with the RUNTHROUGH Hypercoat Guidewire, do you then utilize that wire to deliver balloons and stents?
Yes, I do use it once I have crossed. Most operators, once they have crossed a lesion, will use the same wire to do the intervention, because no one really wants to go through the hassle of changing a wire, mistakenly pulling a wire out, or creating added levels of complexity. The difference is when I am using a non-RUNTHROUGH Hypercoat Guidewire further distally, like a PT Extra Support or a Whisper, or a Choice PT 2, I am extremely conscious of not permitting the wire tip to go out too far. In that situation, I am sometimes sacrificing wire support in order to minimize vascular trauma distally. With the RUNTHROUGH Hypercoat Guidewire, I don’t worry about it. I intentionally prolapse the wire and push it out further, and typically get a very good result.
How do you evaluate whether vessel trauma or injury has occurred?
Post intervention, you have to be meticulous with your shots. Stay on cine fluoroscopy longer, and make sure you don’t have what looks to be a wire perforation, wire dissection, or wire issues distal to the area that you worked on. It does take some degree of focused attention and due diligence to make sure that you haven’t created a wire injury distally; otherwise you will finish your intervention and there will often be a complication down the road that you missed.
Do you have any tips or tricks for new users of the RUNTHROUGH Hypercoat Guidewire?
My recommendation would be to try using it in situations where you would reach for your hydrophilic wire. Evaluate its ability to cross lesions and its ability to travel distally with minimal wire trauma. If it fits your requirements for crossing lesions and maintaining safety, then the RUNTHROUGH Hypercoat Guidewire can be the wire you reach for more often than not. Between the RUNTHROUGH Extra Floppy Guidewire and the RUNTHROUGH Hypercoat Guidewire, I rarely reach for another wire. I am successful 98% of the time with those two wires alone.
As a user of both RUNTHROUGH NS Extra Floppy and Hypercoat Guidewires, what criteria do you use when selecting the appropriate wire?
If the lesion is calcified and very highly stenosed, then 95-99% of the time I won’t even try the RUNTHROUGH Extra Floppy Guidewire, I will just go straight to the RUNTHROUGH Hypercoat Guidewire. Or, in a situation where the lesion is further down in the vessel and I want to get as much wire support as possible so I don’t have to take my wire out uncomfortably far into a blood vessel, then in that case, I will reach for a RUNTHROUGH Hypercoat Guidewire first, with the intention to prolapse it and advance it distally.
Any final thoughts?
The RUNTHROUGH Hypercoat Guidewire is a great wire. Ever since its introduction in our lab, I have been utilizing this wire often in my practice, and it has been an asset. We do very complex transradial coronary interventions and have found the RUNTHROUGH Hypercoat Guidewire to be a valuable tool in the coronaries. We are using transradial access to be as safe as possible for the patient and minimize bleeding complications. If you already have that mentality when you are doing coronary interventions, then choosing a wire that is atraumatic makes your procedure that much safer.
Dr. Amit Srivastava can be contacted at asrivastava@bahc.com.
Disclosure: Dr. Srivastava reports he is a consultant and proctor for Abbott Vascular, Endologix, Terumo, Volcano Corporation, and W.L. Gore and Associates.
