


Case Report
TAVR: Valve-in-Valve Challenges and a Unique Approach with an EN Snare Device
 Aortic stenosis (AS) affects 5% of people older than 75 and 8% of those older than 80. Once symptoms of AS have presented, life expectancy is between two and three years.1 Unfortunately, medical management does not extend life expectancy. Traditional approaches for mitigating symptomatic AS include surgical aortic valve replacement (SAVR). However, due to high surgical risk, about a third of patients are rejected.2,3 Patients deemed “non-surgical” have a EuroSCORE >20% or Society of Thoracic Surgeons (STS) score >10%. These high risk patients have extenuating characteristics, i.e., a porcelain aorta, advanced liver disease, chronic renal disease, frailty, and patent left internal mammary artery grafts (LIMA).4,5 Due to these factors limiting SAVR, transcatheter aortic valve replacement (TAVR) has been utilized to treat these high risk patients.
Aortic stenosis (AS) affects 5% of people older than 75 and 8% of those older than 80. Once symptoms of AS have presented, life expectancy is between two and three years.1 Unfortunately, medical management does not extend life expectancy. Traditional approaches for mitigating symptomatic AS include surgical aortic valve replacement (SAVR). However, due to high surgical risk, about a third of patients are rejected.2,3 Patients deemed “non-surgical” have a EuroSCORE >20% or Society of Thoracic Surgeons (STS) score >10%. These high risk patients have extenuating characteristics, i.e., a porcelain aorta, advanced liver disease, chronic renal disease, frailty, and patent left internal mammary artery grafts (LIMA).4,5 Due to these factors limiting SAVR, transcatheter aortic valve replacement (TAVR) has been utilized to treat these high risk patients.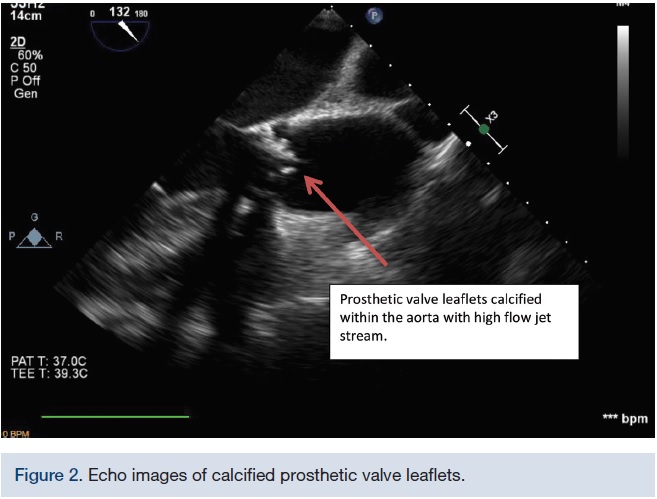 The first TAVR procedure was performed in 2002 by Dr. Alain Cribier and his colleagues.6 Compared to the traditional surgical approach, TAVR is less invasive and is performed without placing the patient on cardiopulmonary bypass or in cardiac arrest.7 As technology developed along with superior valve device morphologies and delivery systems, adverse outcomes were reduced. In the CoreValve US Pivotal Trial, adverse outcomes were reduced by 40.7% in the CoreValve (Medtronic) group versus standard therapies.8
The first TAVR procedure was performed in 2002 by Dr. Alain Cribier and his colleagues.6 Compared to the traditional surgical approach, TAVR is less invasive and is performed without placing the patient on cardiopulmonary bypass or in cardiac arrest.7 As technology developed along with superior valve device morphologies and delivery systems, adverse outcomes were reduced. In the CoreValve US Pivotal Trial, adverse outcomes were reduced by 40.7% in the CoreValve (Medtronic) group versus standard therapies.8There are three major delivery techniques for TAVR: retrograde percutaneous access, direct transapical puncture, and direct aortic access. Retrograde femoral artery assess is most commonly employed. However, due to severe peripheral artery disease or an extremely calcified ascending aorta or arch (porcelain aorta), the retrograde femoral approach may not be feasible.
 There is a specialized group of clients who present an increased challenge to TAVR teams: valve-in-valve cases. Valve-in-valve procedures are best suited for patient who present with regurgitation and/or stenosis of the aortic bioprosthetic valve. However, those patients who are deemed to be a too high of a risk for SAVR (STS risk score of ≥8% or at a ≥15% risk of mortality at 30 days)9 are candidates for a TAVR valve-in-valve technique. The CoreValve Evolut R and the Sapien XT valve (Edwards Lifesciences) are approved for valve-in-valve TAVR.
There is a specialized group of clients who present an increased challenge to TAVR teams: valve-in-valve cases. Valve-in-valve procedures are best suited for patient who present with regurgitation and/or stenosis of the aortic bioprosthetic valve. However, those patients who are deemed to be a too high of a risk for SAVR (STS risk score of ≥8% or at a ≥15% risk of mortality at 30 days)9 are candidates for a TAVR valve-in-valve technique. The CoreValve Evolut R and the Sapien XT valve (Edwards Lifesciences) are approved for valve-in-valve TAVR.One challenge of the CoreValve is that it cannot be placed transapically, thereby limiting options for placement. In addition to this access restriction, there is also a barrier in crossing a wire from the aorta through the bioprosthetic valve in a retrograde fashion. This limitation has been discussed in the literature, but there have been no case studies offering techniques to overcome this barrier. We believe this case study is the first of its kind to be reported in the literature.
Case Report
 This is a 62-year-old male with a history of aortic stenosis status post bioprosthetic aortic valve replacement in December 2009 followed by a pericardial window in January 2010. He has a past medical history of left partial nephrectomy, diabetes, hypertension, hyperlipidemia, polysubstance abuse (methamphetamines, marijuana), gastric reflux, alcohol abuse, osteoarthritis, bipolar II disorder, depression, smoking history of 25 years and hepatitis C. His initial transaortic valve replacement procedure date was delayed due to a low platelet count of 74,000. The liver ultrasound did not reveal cirrhosis and it was believed the low platelet count was due to longstanding hepatitis C. He also presented with a high HCV viral load RT of 2,228,458 Iu/ml. The rest of his labs were unremarkable. His medication regimen consisted of ledipasvir 90 mg/sofosbuvir 400 mg, aspirin 81 mg, glipizide 10 mg, metformin 1000 mg, omeprazole 20 mg, metoprolol tartrate 25 mg, simvastatin 40 mg. He was allergic to Vicodin.
This is a 62-year-old male with a history of aortic stenosis status post bioprosthetic aortic valve replacement in December 2009 followed by a pericardial window in January 2010. He has a past medical history of left partial nephrectomy, diabetes, hypertension, hyperlipidemia, polysubstance abuse (methamphetamines, marijuana), gastric reflux, alcohol abuse, osteoarthritis, bipolar II disorder, depression, smoking history of 25 years and hepatitis C. His initial transaortic valve replacement procedure date was delayed due to a low platelet count of 74,000. The liver ultrasound did not reveal cirrhosis and it was believed the low platelet count was due to longstanding hepatitis C. He also presented with a high HCV viral load RT of 2,228,458 Iu/ml. The rest of his labs were unremarkable. His medication regimen consisted of ledipasvir 90 mg/sofosbuvir 400 mg, aspirin 81 mg, glipizide 10 mg, metformin 1000 mg, omeprazole 20 mg, metoprolol tartrate 25 mg, simvastatin 40 mg. He was allergic to Vicodin.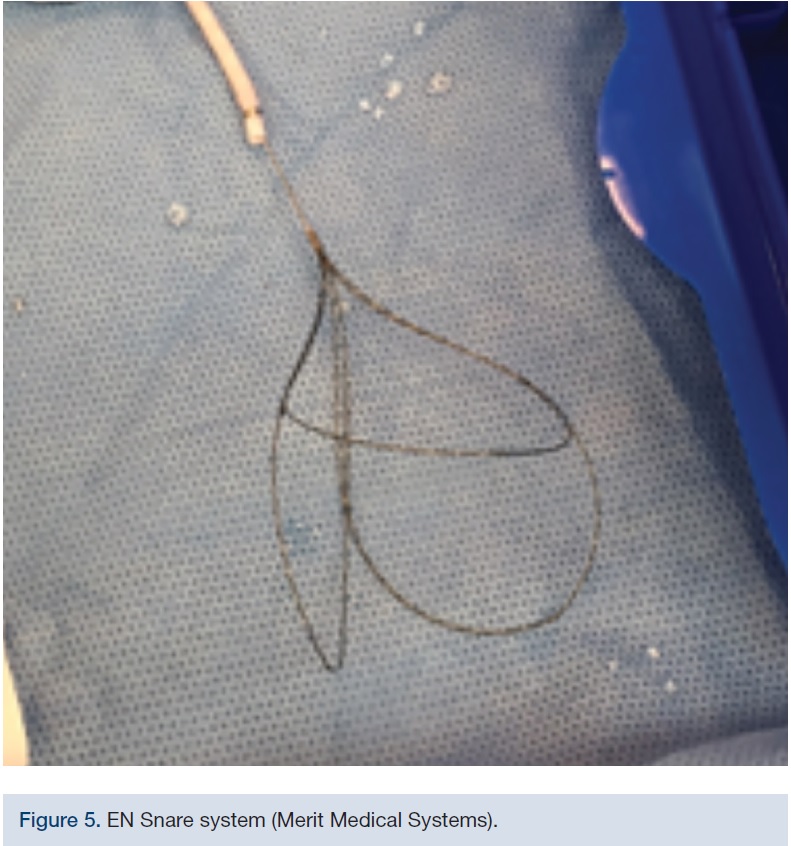 A 2D echocardiogram in February 2016 identified severe stenosis of the prosthetic aortic valve with a mean gradient of 70 mmHg. The left ventricular ejection fraction was normal. Compared to the transthoracic echocardiogram (TTE) in January 2010, there was a significantly higher AV gradient and now a mild to moderate mitral regurgitation. The left ventricle was normal in size and there was moderate concentric left ventricular hypertrophy. The right ventricle was normal in size, thickness, and function. The right ventricular systolic function was normal. The left and right atrial sizes were normal. The mitral valve leaflets appeared thickened, but opened well. There was mild mitral annular calcification and mild to moderate mitral regurgitation. The aortic root was normal in size. The inferior vena cava appeared normal. The aortic valve area was 0.67 cm2.
A 2D echocardiogram in February 2016 identified severe stenosis of the prosthetic aortic valve with a mean gradient of 70 mmHg. The left ventricular ejection fraction was normal. Compared to the transthoracic echocardiogram (TTE) in January 2010, there was a significantly higher AV gradient and now a mild to moderate mitral regurgitation. The left ventricle was normal in size and there was moderate concentric left ventricular hypertrophy. The right ventricle was normal in size, thickness, and function. The right ventricular systolic function was normal. The left and right atrial sizes were normal. The mitral valve leaflets appeared thickened, but opened well. There was mild mitral annular calcification and mild to moderate mitral regurgitation. The aortic root was normal in size. The inferior vena cava appeared normal. The aortic valve area was 0.67 cm2.The patient underwent a cardiac catheterization in early March 2016 that showed right coronary artery dominance and a diseased proximal ramus intermedius.
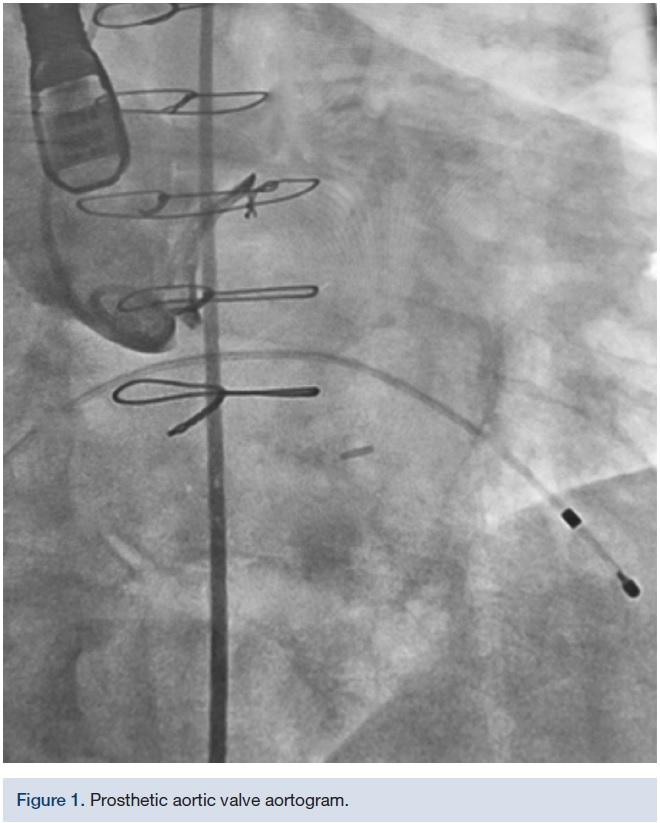
 The initial TAVR was attempted in the hybrid operating room (OR) with the heart team once the patient’s viral load was 104 Iu/ml and platelet count was 89,000. The left femoral artery was accessed with a 6 French (F) sheath and a 6F straight pigtail was advanced over a standard .035-inch wire into the non-coronary cusp of the ascending aorta. The left femoral vein was accessed with a 6F sheath and a temporary pacing wire was placed. A cutdown was performed on the right femoral artery, serially upsizing to an 18F DrySeal sheath (Gore Medical) over a .035-inch Lunderquist extra stiff wire (Cook Medical).
The initial TAVR was attempted in the hybrid operating room (OR) with the heart team once the patient’s viral load was 104 Iu/ml and platelet count was 89,000. The left femoral artery was accessed with a 6 French (F) sheath and a 6F straight pigtail was advanced over a standard .035-inch wire into the non-coronary cusp of the ascending aorta. The left femoral vein was accessed with a 6F sheath and a temporary pacing wire was placed. A cutdown was performed on the right femoral artery, serially upsizing to an 18F DrySeal sheath (Gore Medical) over a .035-inch Lunderquist extra stiff wire (Cook Medical). A 6F Judkins Right (JR) 4 catheter was advanced over a standard wire in an attempt to cross the aortic valve under fluoroscopy and 3D echo/transesophageal echocardiogram (TEE) guidance. A variety of wires and catheters were attempted (.035-inch Rosen wire [Cook Medical], .035-inch Cook straight tip [Cook Medical], Merit .035-inch angled Glidewire, .035-inch Lunderquist extra stiff straight wire, Steelcore .018-inch extra support [Abbott Vascular], 6F Amplatz Left1, 6F JR4, 6F MPA [Cardinal Health], 6F IM, 6F H-stick guide [Cardinal Health], and 6F straight and angled pigtail catheters), but the operators were unable to successfully cross the prosthetic stenotic aortic valve in a retrograde fashion. After 2.5 hours, the case was aborted.
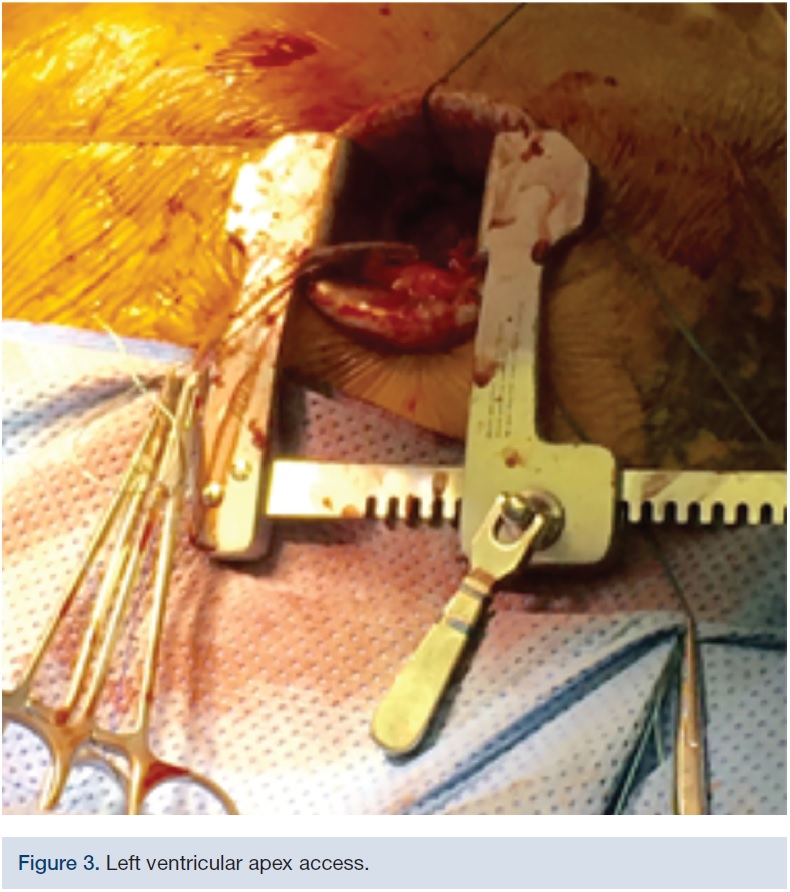
A week later, the case was re-attempted. The left femoral artery again underwent a surgical cutdown. Access through the right femoral artery and vein was replicated. A small thoracotomy was made in the 5th intercostal space over the point of maximal impulse and with the guidance of ultrasound. The pectoralis muscle was reflected off the ribs and the pleural space was entered. The pleural fat was cleared from the pericardium and the pericardium was sharply incised. Some filmy adhesions were removed and a small pericardial cradle was created. The apical dimple was identified. A 4-0 Prolene purse string was placed around the dimple.
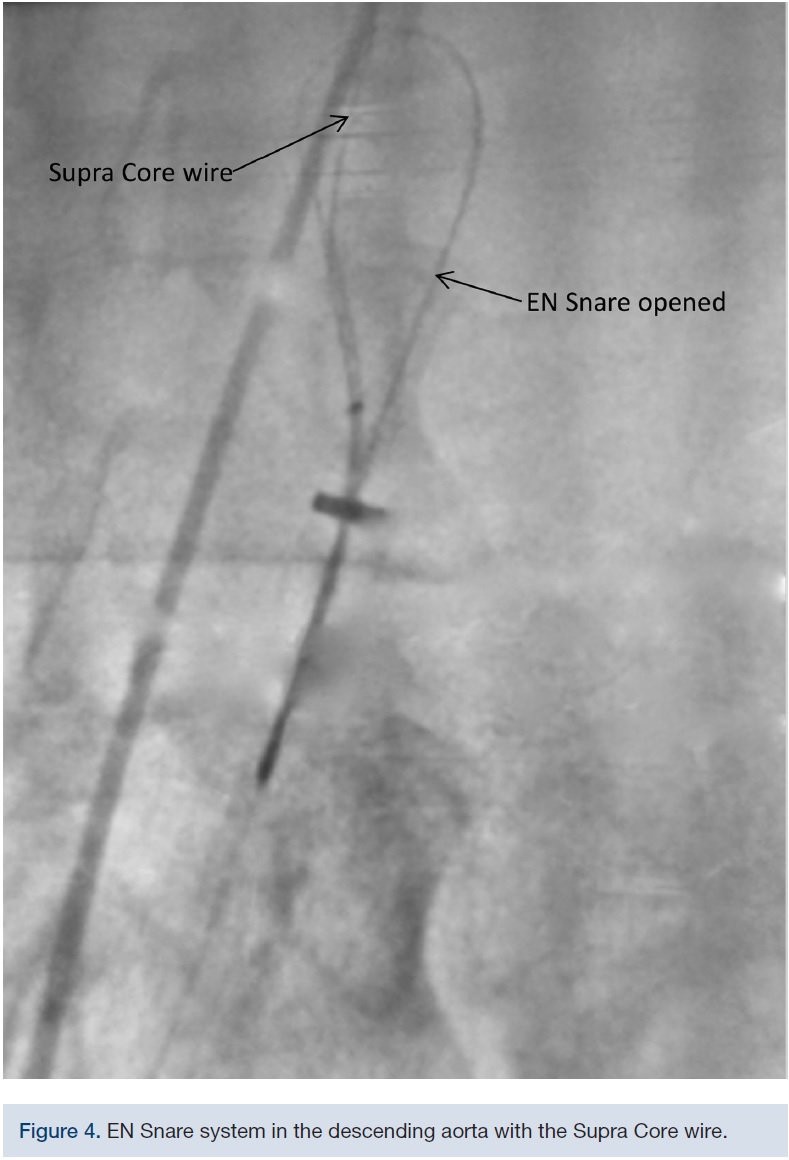
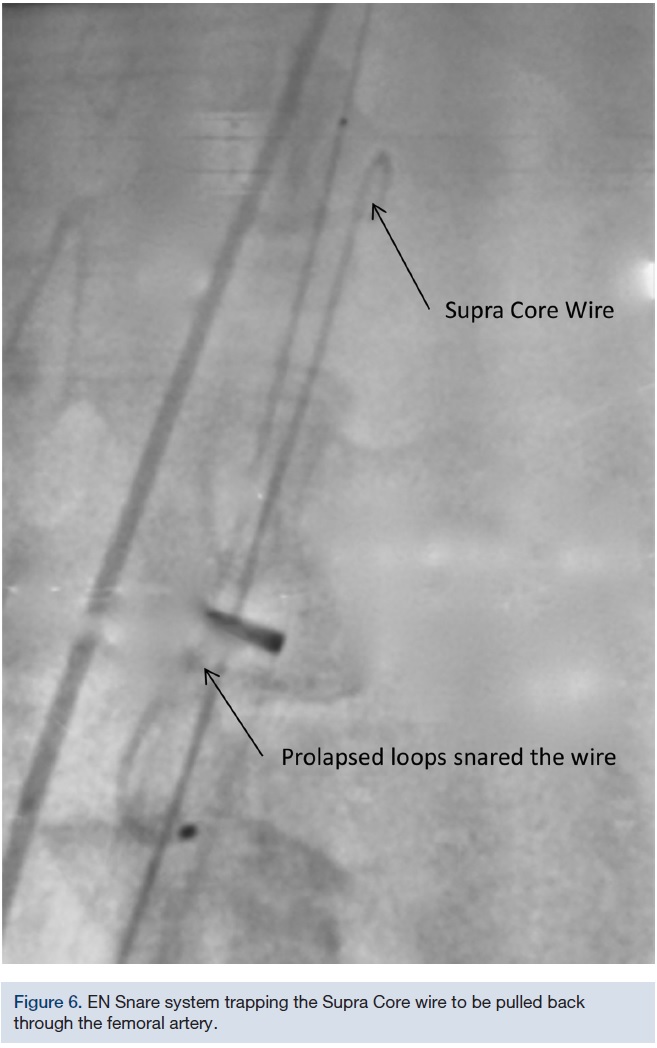
The 18F DrySeal sheath was placed through the right common femoral artery over an .035-inch Lunderquist extra stiff wire. A 4F micropuncture needle was advanced through the apical window into the left ventricular cavity. A micropuncture wire was advanced antegrade across the aortic valve into the ascending aorta. Finally, the micropuncture sheath was advanced over the wire into the ascending aorta, and the micropuncture needle and wire were removed. An .035 inch x 300 cm Supra Core 35 wire (Abbott Vascular) was advanced via the transapical sheath into the ascending aorta and ultimately, to the descending aorta. The transapical sheath was then removed. A triple-lobed EN Snare Endovascular Snare System (Merit Medical Systems) was inserted into the 18F femoral arterial sheath and the Supra Core .035-inch wire was trapped. Subsequently, a 6F pigtail catheter was advanced over the snared Supra Core .035-inch wire and placed into the left ventricle. The Supra Core .035-inch was replaced by a 260 cm Amplatz .035-inch Super Stiff wire (Boston Scientific) and advanced into the left ventricle through the pigtail catheter. The pigtail catheter was removed and an 18 mm Z-Med II balloon (B. Braun Interventional Systems) was inserted over the Amplatz super stiff wire. A standard balloon aortic valvuloplasty was performed in preparation of the valve positioning. After the balloon valvuloplasty, a 23mm CoreValve Evolut R was successfully deployed. A 22 mm True Dilatation balloon (Bard Peripheral Vascular) was utilized to perform post dilation aortic balloon valvuloplasty. The final result was a mild aortic insufficiency with a 5 mm transvalvular gradient.
The case was completed with surgical closure of the cutdown, and apical window and manual pressure of the femoral artery. The patient was admitted to the surgical intensive care unit with a chest tube and temporary pacemaker.
A 2D echo with color flow and doppler was repeated in April 2016, a month post-procedure. A mild to moderate perivalvular regurgitation was noted around the prosthetic aortic valve. There was no gross rocking of the valve, but there was a potential space between the valve and aortic annulus resulting in a mild peri-valvular aortic insufficiency due to the large calcified plaque on the aortic cusp.
This case offered a unique method for the placement of the CoreValve Evolut R via the apical approach with the use of a snare system. The innovative technique allowed the operators to cross the stenotic aortic valve in an antegrade fashion. This case provides an alternate avenue for placing the CoreValve when complicated aortic valve anatomy prevents routine retrograde placement of the crossing or support wire.
However, as reported in the literature, this process has its own distinctive set of complications and risks due to the apical puncture, as described in a Canadian multicenter study comparing transfemoral (TF) and transapical (TA) approaches.10
Even though this patient presented with serious comorbidities, he was discharged five days after the TAVR procedure and has vocalized a significant change in his quality of life at subsequent follow-up appointments.
References
- Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(13):e1-e142.
- Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, et al. A prospective survey of patients with valvular heart disease in Europe. The Euro Heart Survey on Valvular Disease. Eur Heart J. 2003; 24: 1231-1243.
- Bach DS, Nishimura RA, Tajik AJ, Schaff HV, Danielson GK. Evaluation of patients with serve symptomatic aortic stenosis who do not undergo aortic valve replacement: the potential role of subjectively overestimating operative risk. Circ Cardioasc Qual Outcomes. 2009; 2: 533-539.
- Edwards FH, Grover FL, Shroyer AL, Schwartz M, Bero J. The Society of Thoracic Surgeons National Cardiac Surgery Database: current risk assessment. Ann Thorac Surg. 1997; 63: 903-908.
- Roques F. The logistic EuroSCORE. Eur Heart J. 2003; 24: 881-882.
- Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous transcatheter implantation of an aortic valve for calcific aortic stenosis; first human case description. Circulation. 2002; 106: 3006-3008.
- Walther T, Kempfert J. Transapical vs.transfemoaral aortic valve implantation: which approach for which patient, for a surgeon’s standpoint. Ann Cadiothorac Surg. 2012; 1(2): 2016-2019.
- Popma JJ. Presented at: Transcatheter Cardiovascular Therapeutics 2013; October 28, 2013-November 1, 2013; San Francisco, California.
- PMA P130009/S034 FDA Summary of Safety and Effectiveness Data. https://www.accessdata.fda.gov/cdrh_docs/pdf13/p130009s034b.pdf. Accessed May 10, 2016.
- Rodés-Cabau J, Webb JG, Cheung A, Ye J, Dumont E, Feindel CM, Osten M, et al. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk: acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol. 2010 Mar 16;55(11):1080-1090.
The authors can be contacted via Bernadette Speiser, Palo Alto VA Health Care System, 3801 Miranda Avenue, Palo Alto, California 94304-129. Tel. 650-493-5000, email bernadette.speiser@va.gov.
