


Spotlight: Mercy Cardiac Cath Lab
The authors can be contacted via Nancy Hintz, RN, BSN, CCRN, at nancy.hintz@allina.com. For more information, visit mhvi.com.
Tell us about your hospital and cath lab.
Mercy Hospital is part of Allina Health and is a 271-bed, not-for-profit hospital that serves the health needs of the northwestern Minneapolis-St. Paul Metropolitan area. Mercy Hospital was named to the Truven Health study’s 100 Top Hospitals for large community hospitals nationwide. In addition, Mercy is among Truven Health’s 50 Top Cardiovascular Hospitals for community hospitals nationwide. Mercy is the only Minnesota hospital listed in these categories.
Mercy Hospital has five total cath laboratories. Two rooms are dedicated to electrophysiology, one room is predominately for peripheral intervention, and the other two rooms are dedicated for coronary procedures. Our team consists of 8 registered nurses (RNs), 6 cardiovascular technologists (CVTs) and 6 registered radiologic technologists (RT[R]s). A separate, dedicated electrophysiology team is made up of an additional 3 RNs, 2 CVTs and 3 RT(R)s. Our combined years of experience add up to 362!
What procedures are performed in your cath lab?
We perform a wide variety of cardiac procedures, including complex right and left heart catheterization, pulmonary hypertension studies, diagnostic angiography with intravascular ultrasound (IVUS), optical coherence tomography (OCT), fractional flow reserve (FFR), and coronary interventions. We utilize orbital and rotational atherectomy, coronary and peripheral laser, and the intra-aortic balloon pump (IABP) and Impella (Abiomed). We also perform patent foramen ovale (PFO) and atrial septal defect (ASD) closure, valvuloplasty, and work on chronic total occlusions (CTOs). Our peripheral angiography and interventional procedures can involve angioplasty, stenting, use of the Crosser catheter (Bard Peripheral Vascular), the Ekosonic Endovascular System (EKOS Corporation), atherectomy, and abdominal aortic aneurysm (AAA) repairs.
Are you performing transcatheter aortic valve replacement (TAVR)?
 We opened a multipurpose, hybrid operating room in July 2014 and plan to begin TAVR procedures in the future.
We opened a multipurpose, hybrid operating room in July 2014 and plan to begin TAVR procedures in the future.
Does your cath lab perform primary angioplasty with surgery on site?
Yes, we have surgical backup within our hospital.
What percentage of your diagnostic caths is normal?
Three percent of our diagnostic caths are normal. We have an active cardiac computed tomography (CT) program that has allowed us to decrease our normal catheterization rate.
Do any of your physicians regularly gain access via the radial artery?
Our interventional physicians are skilled in radial access when appropriate.
Who manages your cath lab?
Nancy Hintz, RN, BSN, CCRN, is the cath lab manager. Erin Brandt, RN, CCRN, is the patient care supervisor. Barry Burrell is the director of cardiovascular services, and Mike Rasmussen is the executive director and vice president of cardiovascular services.
Do you have cross-training? Who scrubs, who circulates and who monitors?
All staff members scrub. The RT(R)s are the only ones to pan the table. The RNs are the only ones who administer sedation. The CVTs mainly monitor cases; however, a few RNs and RT(R)s can also monitor cases. We also have a daily charge nurse who  oversees the flow of the day for both the electrophysiology and cardiovascular labs. Our staff enjoys the flexibility of rotating roles during cases.
oversees the flow of the day for both the electrophysiology and cardiovascular labs. Our staff enjoys the flexibility of rotating roles during cases.
Which personnel can operate the x-ray equipment (position the II, pan the table, change angles, step on the fluoro pedal) in your cath lab?
The RT(R) manages the imaging equipment and table movement. The physician operates the foot pedal to control dosing.
How does your cath lab handle radiation protection for physicians and staff?
All staff in the room has personally fitted lead aprons with optional lead glasses. All staff has radiation monitoring badges that are changed and monitored monthly. There is a mobile lead shield available in each room for the nurses and a suspended one for the physicians. We also have a sterile, disposable, lead-free shield the physician lays on the patient’s groin for scatter protection (RadPad, Worldwide Innovations & Technologies, Inc.). Our physicians also try to avoid triggering fluoro/cine when a nurse or staff member needs to move close to the patient during the procedure. We also use low-dose fluoro at 7.5 frames per second (FPS), stand as far back from the image intensifier as possible, and avoid high-dose cine.
Are you recording fluoroscopy times and dosages?
We record the time and dose from each case from the Mac-Lab monitoring system (GE Healthcare) that we utilize in our lab.
Who documents medication administration during the case?
The RN is responsible for documenting all medication administered throughout the case.
How does your lab communicate information to staff and physicians to stay organized and on top of change?
We use email and communication boards posted throughout the department. Staff meetings are held regularly as well. We utilize a visual improvement board where problems and issues are shared and discussed in staff huddles, and the staff are empowered to implement ideas for improvement.
What are some of the new equipment, devices and products introduced at your lab lately?
Orbital atherectomy and SubQ ICD (subcutaneous implantable cardioverter defibrillator, Boston Scientific) have both been recent additions to our lab.
How is coding and coding education handled in your lab?
Two staff members do the procedure coding and a separate group handles the physician coding. Staff attends webinars and seminars to stay current with coding changes and updates.
Who pulls the sheaths post procedure, both post intervention and diagnostic?
Our RNs and two of our cardiovascular associates are trained to pull sheaths. To gain competency, staff first reviews several sources of validation (including Mosby Nursing Skills and Consult books, and current hospital policy and procedures). This content prepares the staff member to effectively pull a sheath manually, achieve hemostasis, and be prepared to treat potential complications. Staff then observes 1-2 manual sheath pulls and the novice participates in a return demonstration (x2) before being considered competent.
Where are patients prepped and recovered (post sheath removal)?
The patients are placed in a private room on arrival. All admission data is collected, blood is drawn, and an IV is started. Patients are then brought to the lab by the RN that will be caring for them.
We have a pre and post area we refer to as CV Short Stay. In the prep/recovery unit, the RNs and cardiovascular associates are all trained to pull with manual pressure. We utilize Angio-Seal (St. Jude Medical), Mynx (AccessClosure/Cardinal Health), Perclose Proglide (Abbott Vascular), and Starclose (Abbott Vascular) in the lab. Patients are either brought back to recovery for sheath pull and discharge, sheath pull and home if they are a same-day stent, or admitted to our telemetry unit as an inpatient.
How is inventory managed at your cath lab? Who handles the purchasing of equipment and supplies?
We have a dedicated CVT who manages our entire inventory. She oversees the entire inventory usage in the cardiovascular, electrophysiology, and peripheral vascular labs.
Is your lab involved in clinical research?
The Mercy Cath Lab is part of Allina Health, and in close collaboration with Metropolitan Heart and Vascular Institute, is heavily involved in cardiac research with studies relating to electrophysiology, stem cell research, peripheral vascular disease, acute coronary syndrome medications, and new devices. At any given time, our cath lab is involved in multiple research studies.
Dr. Jeff Chambers is a very active principal investigator (PI) both at local and national levels. Currently he is the national PI for the ORBIT II study, a pivotal trial to evaluate the safety and efficacy of the Diamondback 360 Orbital Atherectomy System (CSI) in  treating de novo, severely calcified coronary lesions.
treating de novo, severely calcified coronary lesions.
Along with Dr. Chambers, we have other physicians actively involved in research. Dr. Daniel Dulas is a PI on LEVANT 2 trial comparing the Moxy drug-coated balloon (Bard Peripheral Vascular) versus standard balloon angioplasty for the treatment of femoropopliteal arteries, as well as other peripheral vascular disease studies. Dr. Stephen Remole is currently the PI for several new and exciting electrophysiology trials. Without an efficient, competent, and hardworking cath lab, these PIs would not be able to accomplish their work within cardiac research.
Can you share your lab’s average door-to-balloon (D2B) times?
Our average D2B time is 51 minutes. We have the ability for the Emergency Medical Services (EMS) to activate the ST-elevation myocardial infarction (STEMI) team, where the patient then bypasses the emergency department. We have excellent communication between departments and between facilities. We also have an ongoing acute MI quality team that meets regularly to assess our progress and looks for areas of improvement.
Who transports the STEMI patient to the cath lab during regular and off hours?
It truly depends on from where the patient is coming. Sometimes the ambulance crew will bring them directly to the lab. If a patient presents in the emergency department, the critical resource nurse will bring them to the cath lab, or cath lab staff will go get the patient from the emergency department. If it is after hours, the patient is usually held in the emergency department until the call team arrives.
What happens when the call team is already busy doing a procedure and a STEMI comes into the ED?
We cover peripheral call as well as coronary call. We are fortunate to have four staff members on front call and two on backup call. If the four-member call team is busy doing a peripheral case and a STEMI comes in, a team member will call in the two back-up 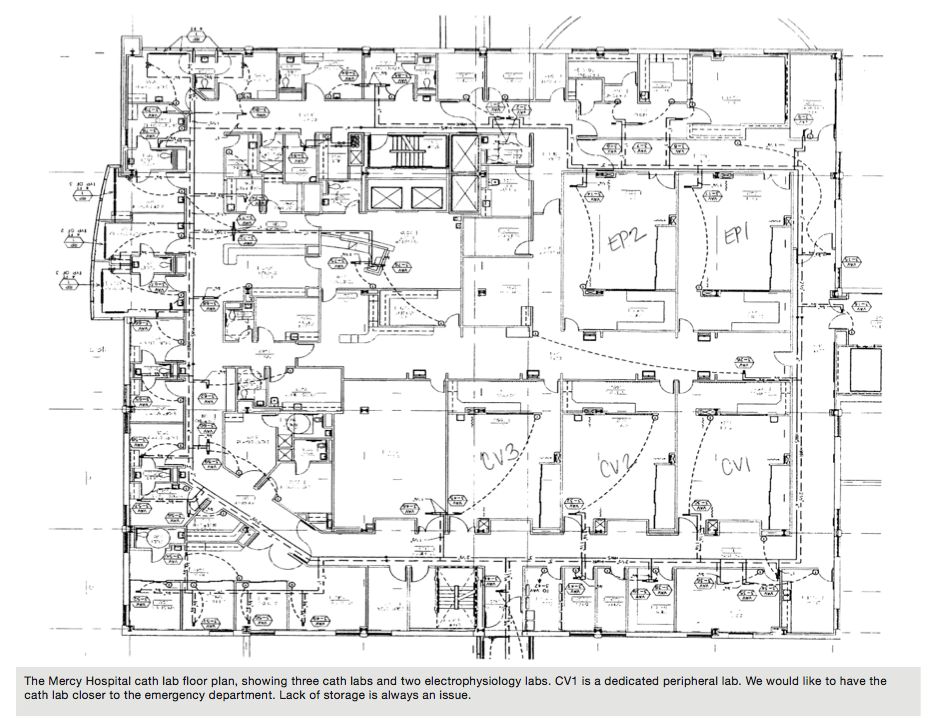 call people to come in and do the case as a three-member team. We work two three-man teams until one of the cases is completed.
call people to come in and do the case as a three-member team. We work two three-man teams until one of the cases is completed.
What measures has your cath lab implemented in order to cut or contain costs?
Allina has a very active cardiovascular supply chain team. They work with and coordinate the cardiovascular service line to review and assist with medical supply costs.
Are your physicians dictating their cath procedure reports, or do they use a structured reporting tool?
We utilize CardioDoc, Lumedx’s primary tool for post-procedural reporting, replacing the need for dictation. Lumedx reports are interfaced to our EMR Epic. Lumedx’s Apollo Advance Clinical Patient Database is a comprehensive cardiovascular database management system that is signed by the RN.
Do you use the American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) or any other outside data collection registry?
Yes, we submit to the NCDR for both CathPCI Registry and ICD Registry.
How does your cath lab compete for patients? Has your institution formed an alliance with others in the area?
We are the only major hospital serving our area.
How are new employees oriented and trained at your facility?
New employees get 8 to 12 weeks of orientation with a primary preceptor. They shadow with someone on call for two months following their orientation.
What continuing education opportunities are provided to staff members?
The physicians offer lunch-and-learns once a month. They educate on a topic of their choice, such as a new procedure, or on topics where staff have requested more knowledge. Staff is also invited to the cardiology fall conference. It is an evening event with 4-5 cardiologists giving presentations on changes, new practices and updates.
An industry representative is welcome to give educational updates or information, if there is a CEU with their presentation. We also have a foundation at our cardiology clinic that supports our staff going to national conferences such as Transcatheter Cardiovascular Therapeutics (TCT).
How do you handle vendor visits to your lab?
We utilize Reptrax vendor credentialing. Vendors check in at a designated area in the hospital. They receive a badge with their picture on it. Each vendor is required to make an appointment and it is approved by the manager or lead tech. No one is allowed in the lab without a badge.
How is staff competency evaluated?
Each staff member has a yearly performance review with the manager. This year we will be seeking feedback from the physicians on each employee’s performance.
Does your lab have a clinical ladder?
Not at this time, but we do have a lead RT(R) and a lead CVT.
Is there a particular mix of credentials needed for each call team?
There are four primary call team members with two backup members. The mix needs to be able to form two three-man teams consisting of two RNs, two RT(R)s, and two CVTs.
Within what time period are call team members expected to arrive to the lab after being paged?
There is an expected response time of 30 minutes.
Do you have flextime or multiple shifts?
We have two 8-hour shifts with 7:30 and 8:30 am start times. The 8:30 am start time is considered the call shift.
Has your lab recently undergone a national accrediting agency inspection?
We are Chest Pain Certified (Cycle 4) with the National Association of Cardiovascular Patient Care (NACPC). We follow NACPC best practices to ensure collaboration between hospital and EMS.
Where is your cath lab located in relation to the operating room and emergency department?
The cardiac cath labs are located on the third floor. The emergency department and OR are located on the first floor.
What is unique or innovative about your cath lab?
We utilize a Patient Advisory Committee to integrate the “patient voice” into our processes. The PAC is composed of previous patients who collaborate with staff to improve care delivery and experience. This is a forum where we can run potential changes past actual patients and they give us feedback on what we could do better.
What’s special about your city or general regional area in comparison to the rest of the U.S.? How does it affect your “cath lab culture”?
Minneapolis is home to major medical device companies such as Medtronic, St. Jude Medical, and Boston Scientific. With 10,000 sparkling lakes and an abundance of scenic paths and trails, it’s no surprise Minneapolis-St. Paul has been named as one of the best places to live and work by Travel & Leisure and CNN.
A question from the American College of Cardiology’s National Cardiovascular Data Registry:
How do you use the NCDR Outcome Reports to drive QI initiatives at your facility?
These reports are presented and reviewed at bi-weekly quality meetings with interventionalists. They are analyzed for trends and potential performance improvement opportunities, allowing us to continuously improve our standard of care.
Questions from the Society of Invasive Cardiovascular Professionals (SICP):
1. Do you require your clinical staff members to take the registry exam for Registered Cardiovascular Invasive Specialist (RCIS)? Does staff receive an incentive bonus or raise upon passing the exam?
The RCIS is not currently required, but is encouraged. There is no bonus at this time.
2. Are your clinical and/or managerial team members involved with any professional organizations that support the invasive cardiology service line, such as the SICP, ACVP, or regional organizations?
Staff members are involved with the American Heart Association (AHA) American College of Cardiology (ACC), and The Society of Invasive Cardiovascular Professionals (SICP).
