


Spotlight: The Heart and Vascular Interventional Laboratory at UMass Memorial Medical Center
U Mass Memorial Health Care (UMMHC) is a dominant health care system in central Massachusetts. UMMHC is a non-profit organization integrated with the University of Massachusetts Medical School. It consists of four hospitals with 1125 beds throughout the system. Our department is called the Heart and Vascular Interventional Laboratory (HVIL), and is located on the University Campus of the flagship UMass Memorial Medical Center, the only hospital in the UMMHC system  with a full-service catheterization laboratory. We provide primary to quaternary health care for the integrated UMMHC system and serve as a regional myocardial infarction center for central Massachusetts, as well as parts of Connecticut and New Hampshire. We provide the most advanced technologies in electrophysiology (EP), interventional cardiology, and interventional vascular procedures.
with a full-service catheterization laboratory. We provide primary to quaternary health care for the integrated UMMHC system and serve as a regional myocardial infarction center for central Massachusetts, as well as parts of Connecticut and New Hampshire. We provide the most advanced technologies in electrophysiology (EP), interventional cardiology, and interventional vascular procedures.
What is the size of your lab?
The HVIL consists of a suite of 7 contiguous procedure rooms, plus a hybrid operating room located within the general OR. Of the seven main procedure rooms, two are primarily dedicated to cardiac procedures, two to EP procedures, and one to peripheral procedures. A third cardiac room is peripheral-capable and a seventh serves as a multifunctional “swing” room that can be used for a wide array of procedures. The hybrid operating room is used for transcatheter aortic valve replacements (TAVR), endovascular graft implantations, and repairs of ruptured abdominal aortic aneurysms. It is staffed by both HVIL and general OR personnel.
What is the mix in your lab?
The HVIL was formed from an integration of cardiac, electrophysiology and vascular staff, in a move to improve overall operating efficiency and patient flow, and consolidate costs. The staffing mix is flexible and based on patient acuity. Typical staffing for cardiac and EP cases consists of 1-2 registered nurses (RN) and one radiologic technologist (RT). Vascular cases are frequently staffed with 1 RN and 2 RTs. In addition to our clinical staff, there are 2 clinical quality managers, a supply coordinator, 2 patient care associates, and 4 ambulatory service representatives. We also have 2 dedicated IT specialists, 1 database coordinator, and 1 coding specialist. Our staff longevity ranges from one year to forty years with an average of 17 years experience.
What procedures are performed in your lab?
We perform a wide array of diagnostic and interventional vascular, EP, and cardiac procedures. In addition to standard vascular peripheral and carotid procedures, our vascular surgeons perform dialysis fistula repair, tunnel catheter insertion, and placement of inferior vena cava (IVC) filters, as well as endovenous laser treatment. Our electrophysiologists perform insertions of implantable cardioverter defibrillators (ICDs) and single and dual-chamber pacemakers, along with complex ablations for ventricular and atrial arrhythmias, including atrial fibrillation using cryoballoon, and hybrid percutaneous and surgical ablations. Our interventional cardiologists perform complex percutaneous coronary intervention (PCI) using rotational, orbital, and laser atherectomy  supported by imaging modalities such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), and if necessary, percutaneous left ventricular (LV) support using a balloon pump, Impella (Abiomed), or even extra-corporal membrane oxygenation. In addition to TAVR, our interventional cardiologists also perform structural heart interventions such as aortic, mitral and tricuspid valvuloplasty, and atrial-septal defect (ASD) and patent foramen ovale (PFO) closures.
supported by imaging modalities such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), and if necessary, percutaneous left ventricular (LV) support using a balloon pump, Impella (Abiomed), or even extra-corporal membrane oxygenation. In addition to TAVR, our interventional cardiologists also perform structural heart interventions such as aortic, mitral and tricuspid valvuloplasty, and atrial-septal defect (ASD) and patent foramen ovale (PFO) closures.
How many procedures are performed per week?
We are prepared 24/7 for any and all cardiac or peripheral emergencies. In 2014, we averaged 57 cardiac diagnostic cases per week and 26 PCIs per week, of which 5 were primary PCI for ST segment elevation myocardial infarctions (STEMIs). In addition to 2974 diagnostic cardiac catheterizations and 1369 PCIs, we also performed 866 peripheral diagnostic cases, 931 peripheral interventional cases, and 2199 EP cases, for a total of 8,339 procedures performed in 2014. Unlike most catheterization laboratories with a high percentage of elective cases, only 22% of our cases are elective (compared to 35% nationally), with 52% being urgent and 26% being emergent (compared to 46% and 19% nationally, respectively).
Can you tell us about your TAVR program?
We began the TAVR program in 2013. From January to July 2015, we have performed more than 40 TAVR procedures in the OR/hybrid room. The TAVR team is an organized collaboration between OR and HVIL staff. After establishing a core TAVR group, we are now educating additional personnel to increase the number of TAVR-ready staff.
What percentage of your diagnostic caths is normal?
The incidence of non-obstructive disease found on elective diagnostic catheterizations averages around 40%, which is slightly lower than the 43% median for other American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) participants. However, elective cases constitute only 22% of our cardiac volume, with urgent or emergent cases having a much lower incidence of non-obstructive disease.
Do your physicians utilize radial access?
Approximately 90% of all our cases are radial access (ACC-NCDR PCI Registry). The rate of radial access for STEMI is 95%. Because of the high rate and improved safety of radial access, we are one of the few hospitals in New England to routinely discharge patients home on the same day of their PCI. Instituted two years ago, approximately 60% of elective PCIs are suitable for same-day discharge. We have recently expanded early discharge for stable acute coronary syndrome patients in whom revascularization  is the final element of their care.
is the final element of their care.
Who manages the cath lab?
The HVIL is managed with a collaborative model consisting of a physician medical director, Jeffrey J. Rade, MD, FACC, a senior director, Kathleen Korenda, MSN, ACNP, MBA, and a nurse manager, Mary Hodgerney, MSN, CNML, ACNP.
Are there licensure laws in your state for fluoroscopy?
Massachusetts state law allows only licensed radiologic technologists, physicians, credentialed nurse practitioners, and physician assistants to operate the fluoroscopic equipment. All staff is required to complete yearly competencies in radiation safety. Staff members directly involved in patient care are provided lead protection, leaded glasses, thyroid protection, and an exposure badge. We have incorporated radiation badge checks as part of our safety time out.
Regulations dictate that radiation technologists operate the x-ray equipment, and nurses administer medication and monitor conscious sedation. All staff members retrieve and set up equipment. Both RNs and RTs can scrub and set up the table. Generally, each room has 2 RNs and 1 x-ray technologist. Monitoring patient status and case recording is assigned to one of the RNs observing in the control room, while the other helps with medication administration and equipment retrieval.
What are some of the equipment or devices recently introduced in your lab?
Newer/updated technologies include OCT, a new approach to chronic total occlusions (CTOs), coronary orbital atherectomy (CSI), an updated version of the Impella, cryoablation, and a peripheral drug-coated balloon (DCB).
How does your lab handle communication?
We hold regular staff meetings, and utilize newsletters, emails, information/communication boards, and information disseminated through the resource/charge nurse on a daily basis.
How is coding handled in your lab?
We have a coding specialist that handles all coding for EP, cardiac, and vascular procedures. She attends coding seminars and is recertified on a yearly basis. The monitoring RN chooses and posts each procedure performed in the case. RFID technology (WaveMark) and bar coding ensures accurate charging and replenishment of equipment for each patient encounter.
Describe the path of hemostasis for diagnostic and interventional procedures.
As most of our access is radial, we use the Vasc Band (Vascular Solutions) or Neptune band (TZ Medical) for hemostasis. Before the patient is taken off the table, we assess for patent hemostasis. After application post procedure, these devices are managed by the nursing staff in the designated recovery area. Groin closure includes Perclose (Abbott Vascular), Angio-Seal (St. Jude Medical) and manual pressure. Manual pressure is addressed by the fellow, physician assistant (PA), or nurse practitioner (NP) directly involved in the procedure. Because of predominant use of radial access, our bleeding event rates are low: 0.1% for diagnostic catheterizations (vs 0.4% nationally) and 1.5% for PCI (vs 2.2% nationally). 
Where are patients prepped and recovered?
Over eighty percent of patients are prepared in our short stay recovery area. This area is utilized to ensure all information, intravenous (IV) access, skin prep, premedication, and consent are completed prior to entry to the procedure room. Upon completion of the procedure, the patient is returned and recovered in the same short stay area. This ensures continuity of care, since the admitting RN cares for the patient following the procedure.
How is inventory handled in your cath lab and who handles supplies?
We have a dedicated supply coordinator that utilizes the Wavemark inventory system. A McKesson supply chain management e-procurement system is used for hospital-wide ordering.
Is your lab involved in clinical research?
Yes, currently we are involved in:
• ABSORB (ABSORB Everolimus Eluting Bioresorbable Vascular Scaffold System – Abbott Vascular);
• SIELLO (safety and effectiveness of the Siello S pacing lead – Biotronik);
• EMANATE (Eliquis evaluated in acute cardioversion coMpared to usuAl treatmeNts for AnTicoagulation in subjEcts with NVAF – Bristol-Myers Squibb, Pfizer);
• ALLSTAR (ALLogeneic Heart STem Cells to Achieve Myocardial Regeneration – Capricor Therapeutics);
• Sodium Nitrite in Acute Myocardial Infarction (whether the intravenous infusion of sodium nitrite safely prevents ischemia-reperfusion injury in subjects with acute myocardial infarction resulting in improved left ventricular function – Johns Hopkins University and Hope Pharmaceuticals);
• CARIN (CMX-2043 to prevent contrast-induced acute kidney injury in acute coronary syndrome patients undergoing coronary angiography – Ischemix, LLC);
• ARTEMIS (Affordability and Real-world Antiplatelet Treatment Effectiveness After Myocardial Infarction Study – AstraZeneca); and
• PROTEGO (to confirm the long-term safety and reliability of the Protego DF4 right ventricular lead – Biotronik).
We are also involved in investigator-initiated and National Institutes of Health (NIH)-sponsored research studies, such as TRIP-PCI (a Phase II, multicenter, randomized, placebo-controlled study to evaluate the safety and efficacy of PZ-128 [pepducin] in 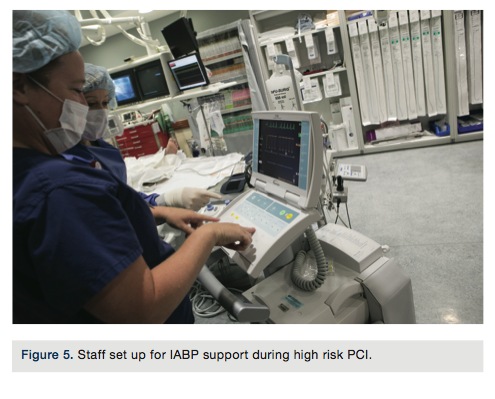 patients undergoing non-emergent PCI).
patients undergoing non-emergent PCI).
Can you tell us about your lab’s door-to-balloon times and STEMI program?
Our median door-to-balloon time for June 2015 (D2B) was 62 minutes. There are several measures we utilize to help maintain the shortest D2B times in the region. We developed a regional STEMI program to ensure patients presenting to the 11 referring sites receive the same safe standard of care as those that present directly to our emergency department (ED). This includes standardized medication recommendations and no IV drips. We provide outreach education to local and regional emergency medical services (EMS) using a structured feedback process, including time, to individuals directly involved in each STEMI. We have developed a STEMI time study sheet to assist us in maintaining our excellent D2B times. The data from those sheets are reviewed daily, directing immediate change where necessary.
Who transports the STEMI patient to the cath lab during regular and off hours?
Transport depends on several factors. If a room is available, the ground/air ambulance team will deliver the patient directly to the waiting STEMI team in the procedure room. If a patient requires evaluation, if a room is not immediately available, or the staff has not yet arrived during off hours, the patient will be held in one of the trauma bays (designated as a STEMI room) in the ED. For the latter, transport would then be performed by the ED RN and the in-house transport structure. Inpatient STEMIs are transported to the catheterization laboratory by the patient’s RN and the interventional cardiology fellow. The transport teams do not change for off-shift hours.
What do you do if the call team is already busy doing a procedure and a STEMI comes in?
Multiple activations require a triage and prioritization process. During normal operating hours, we have enough built-in flexibility to typically accommodate simultaneous activations with minimal delays. Having multiple rooms offers the advantage of eliminating “turnaround” time in urgent situations. If necessary and safe to do so, an active procedure can be halted or a scheduled patient can be potentially “bumped” to follow an emergent case. While multiple off-hour STEMI activations occur frequently, simultaneous activations are more challenging, but fortunately, relatively rare. In the setting of simultaneous STEMIs, the most urgent or the in-process case would go forward and the next case would follow in another room. As one case is winding up, one or two of the staff  can break off to prepare a second room.
can break off to prepare a second room.
What measures has your cath lab implemented in order to cut or contain costs?
Over the last few years, physician and staff schedules were reviewed and adjusted to maximize room utilization. The lab hours of operation were changed to decrease down time. A late-stay team was added to the schedule, in addition to the call team, to finish cases running past normal hours.
RN and RT staff began orienting to basic shared competencies in both areas. This increases productivity by providing the ability to utilize all staff where needed.
Supplies and equipment have been scrutinized and consolidated where possible to maximize savings through contracts and bulk pricing.
What quality control/quality assurance measures are practiced in your cath lab?
Within the last few years, we have developed a standardized nursing handoff sheet. This is to address National Patient Safety Goal (NPSG) #2, safe handoff. Addressing this issue can help to reduce up to 85% of errors caused by lack of full information transfer.
One of our communication boards displays the D2B times and other issues in the lab on a monthly basis. We have an idea board for any and all thoughts addressing improving efficiency, decreasing waste, or something as simple as improving our trash recycling efforts.
Are you recording fluoroscopy times/dosages?
Every case involving fluoroscopy or cine time is recorded in the case record by the RN. At completion, the x-ray is terminated and the doses are recorded in the report section for radiation dosage. Doses are closely monitored by our IT staff and in-house radiation safety officer. The HVIL medical director receives notification from the radiation safety officer of every case that exceeds standard limits.
Who documents medication administration during the case?
The RN who gives the medication documents the administration. This is the nurse inside the lab who also helps with equipment retrieval and patient needs. The nurse in the control room documents case events and is a backup to ensure all medication administration is documented.
Are your physicians dictating their cath procedure reports or do they use a structured reporting tool?
The cardiac physicians use the Centricity DMS reporting system (GE Healthcare). The peripheral physicians dictate their reports.
How does your cath lab compete for patients? Has your institution formed an alliance with others in the area?
We have formed alliances with 11 hospitals, primarily serving central Massachusetts, northern Connecticut and southern New Hampshire, but will also receive patients from Rhode Island and eastern New York State via our Life Flight or Boston Med Flight. There is only one other hospital in central Massachusetts with an active cardiac catheterization laboratory. We provide ongoing and timely feedback to referring physicians and hospitals regarding patient outcomes and door-to-balloon times.
How are new employees oriented and trained at your facility?
New staff members without prior catheterization laboratory experience are oriented over a three-month period. New staff members with prior experience are assessed by several experienced staff members and an appropriate, adjusted orientation is agreed upon. We start with basic procedures and educate up to the more complex.
What continuing education opportunities are provided to staff members?
We have frequent in-services on equipment we stock, but may not use routinely. The weekly staff meeting can provide continuing education credits if applied for. Dedicated time is available on a weekly basis for learning needs identified by staff requests. Staff has the ongoing opportunity to attend the weekly interventional cardiology and HVIL clinical conferences.
How do you handle vendor visits to your lab?
All vendors to the hospital must register every day and display a badge for that day. The HVIL restricts vendors from using the break room and from walking into cases unless specifically invited by the attending physician for that case.
How is staff competencies evaluated?
The individual is responsible for completing online and face-to-face competency tests on a yearly basis. These include electrocardiogram (EKG) interpretation, intra-aortic balloon pump counter pulsation therapy, wound care, IV insertion, policy updates, moderate sedation protocol, and medication administration testing. Every x-ray technologist and RN is basic life support (BLS) and advanced cardiac life support (ACLS) certified.
Is there a particular mix of credentials needed for each call team?
Each call team consists of one attending physician (cardiac or peripheral), one fellow (cardiac or peripheral), two RNs, and one RT. We perform both peripheral and cardiac procedures on a daily basis, so there are no additional credentials required to take call.
Within what time period are call team members expected to arrive to the lab after being paged?
We have a 30-minute response time. Staff members live at varying distances from the hospital; earlier arrivals will begin the information gathering and room set up before the rest of the team arrives, so we can accept the patient to the lab as soon as possible.
Do you have flextime or multiple shifts?
We have a modified fixed schedule. We start our days at 7:00am and run until 5:30pm, except for Wednesday, when we start at 7:30am and run until 6:00pm, in order to accommodate physician and staff meetings. Each workday has a late-stay team responsible for completing cases not quite completed by shift end. The late-stay team consists of 2 RNs and an RT.
Has your lab recently undergone a national accrediting agency inspection?
Our Joint Commission visit was in 2014. The best advice is to continuously seek improvement. Be consistent in your approach to every case, practice effective communication, and stay focused on the needs of the patient.
Where is your cath lab located in relation to the operating room (OR) and ED?
The operating rooms are on the same floor and on the other side of a dividing corridor. The ED is located one floor down on the other side of the dividing corridor. Transport from/to either is very easy.
What trends have you seen in your procedures and/or patient population?
The shift to radial approach has essentially eliminated groin complications. This has also improved patient satisfaction related to immediate mobility and prompt discharge times. The use of wrist hemostasis devices has freed up fellows immediately post procedure.
The patient population demographics have remained consistent, with 67% being male and 33% female.
What is unique or innovative about your cath lab staff?
The HVIL staff is quite unique and extremely innovative. Because nearly 80% of the cardiac cases are urgent or emergent, we have had to maximize flexibility within our system to accommodate the tremendous hour-to-hour unpredictability in case mix and volume. Integrating EP and cardiac/vascular staff and developing shared competencies has allowed us to better adapt to this ever-present unpredictability.
The high percentage of radial cases (89% vs 26% of other reporting NCDR institutions) has allowed us to institute a same-day PCI program that makes us a stand out for both safety and patient satisfaction.
We are unique in that the average number of years of cardiac cath lab experience for our staff is roughly 17. Our recognition-primed decision-making prevents errors rather than reacting to them. Our skill level and ability improves patient safety, lab efficiency, and has allowed the opportunity to continue growth into new competencies and technologies.
Our lab is unique in that it performs procedures such as TAVR and convergent a-fibs in a hybrid OR. Staff are actively involved in developing workflows and macros to accommodate the shared procedures, and have learned to provide skilled care in the OR environment. We routinely accommodate procedures from standard diagnostics to highly specialized endovascular, EP, and cardiac procedures. Education and learning is ongoing as we frequently trial and evaluate new equipment and technology.
We continuously explore opportunities for new types and numbers of procedures we perform. This has allowed us to expand our skills and our repertoire of procedures. All of these innovations maintain profitability and improve our marketing abilities.
What’s special about your city or general regional area in comparison to the rest of the U.S.? How does it affect your cath lab culture?
We service a very diverse population in central Massachusetts. There is only one other cardiac catheterization laboratory in the area. We have nurtured connections with 11 area hospitals to mutually benefit all involved, while improving service to the communities we serve.
