


Spotlight: The Cleveland Clinic Sydell and Arnold Miller Family Heart and Vascular Institute
The authors can be contacted via Scott Hantz, BSN, RN, EMT-P, Nurse Manager, at hantzs@ccf.org
Tell us about your cath lab.
The Cleveland Clinic Cath/EP Labs have a total of 16 rooms plus 2 hybrid operating rooms (ORs). In the cath lab, we have 8 cath lab rooms plus 2 hybrid ORs that we utilize on Monday, Tuesday, and Wednesday of each week. The cath lab staff consists of 27 registered nurses (RNs), 7 x-ray technologists/registered cardiovascular invasive specialists (RCISs), 4 patient care techs, 2 patient schedulers, 1 inventory specialist, 2 IT specialists, 2 assistant nurse managers, and 1 nurse manager. The cath lab is staffed 24/7/365 with at least 2 staff members in-house to support our busy ST-elevation myocardial infarction (STEMI) program. We have staff that has been with the lab for more than thirty years as well as some who have been with us for as little as a couple of months. The staff work well together and use each other’s strengths to give each patient world-class care.
What procedures are performed in your cath lab?
Per our outcomes book, on an annual basis:
- Diagnostic cardiac catheterizations: 7000-8000
- Interventional cardiac procedures: 1500-1700
- Percutaneous aortic valvuloplasties: 150-250
- Percutaneous mitral valvuloplasties: 10-20

- Percutaneous atrial septal defect and patent foramen ovale closures: 40-70

Can you tell us about your transcatheter aortic valve replacement (TAVR) program?
We started a TAVR program in May 2006, one of the first three centers in the United States as part of the early feasibility trial (REVIVAL). We have been leaders in several TAVR trials and continue to be passionately involved in the field. We published our intital experience of all transfemoral cases performed in the catheterization laboratory, showing only 0.4% 30-day mortality1, almost 10 times lower compared to other studies at that time. We have now built another biplane hybrid OR, staffed by cath lab and OR personnel, where we do all transfemoral cases. Other alternative access cases are done in a different hybrid OR. We are typically performing 6-8 cases per week.
What percentage of your diagnostic caths is normal?
About 15%, although this number is difficult to interpret due to preoperative surgical catheterizations that can be normal and due to our highly complex cases.
Do any of your physicians regularly gain access via the radial artery?
Yes, at this time, we are 60% radial and we only see that number rising.
Who manages your cath lab?
Scott Hantz, BSN, RN, EMT-P, Nurse Manager, and Samir Kapadia, MD, Medical Director, Section Head.
Do you have cross-training? Who scrubs, who circulates and who monitors? 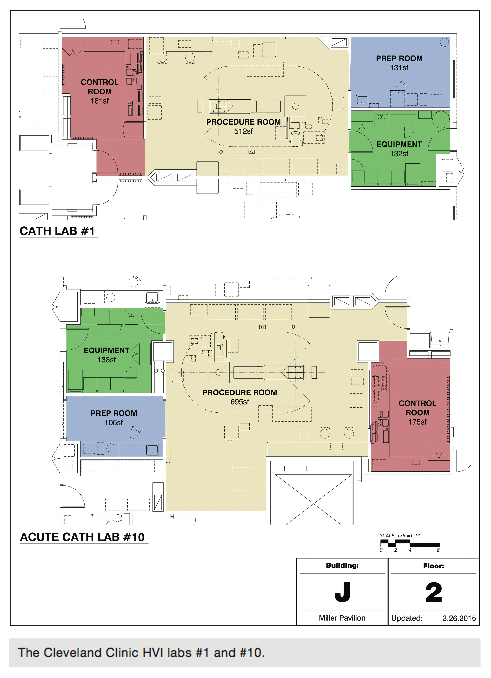
In the lab, we use the team approach. Each staff member is assigned a daily room assignment with other team members, usually consisting of 3-4 staff members with a mix of at least 2 RNs and 1 cardiovascular technologist. Each room is assigned a room charge who is the leader of the team in the room. Besides taking a leadership role in the lab they are assigned, the room charges are also responsible for effectively communicating to the charge issues that affect patient care in the room, such as patient flow or delays.
Each team member is assigned a role for a case. Typically one team member scrubs, another is assigned as the circulator, and the other RN team member will monitor during the case and administer conscious sedation. The team rotates assignments after each case so that each team member participates in each role throughout the day. This allows the staff to stay proficient and competent in each role so that they can easily assume multiple roles if the situation dictates. 
Fellows and staff physicians also are also an integral part of our team. Fellows and attending cardiologists also help in turning the room around and scrubbing when needed.
Are there licensure laws in your state for fluoroscopy?
Yes, there are specific laws that pertain to the use of fluoroscopy in Ohio. We have a radiation safety department that is in place to make sure that all departments using fluoroscopy are in compliance with those laws.
Which personnel can operate the x-ray equipment (position the II, pan the table, change angles, step on the fluoro pedal) in your cath lab? 
The only staff that can operate the x-ray equipment are the physicians and our cardiovascular technologists (CVTs) who are also radiologic technologists. They must complete a 6-course didactic curriculum that is required by the standards set by the Cleveland Clinic. After the successful completion of this material, they are given machine-specific training. Only then can they be considered competent to “step on fluoroscopy” and teach new staff, such as incoming yearly fellows or new attending physicians. They also become our unit experts in regards to operating and troubleshooting x-ray related issues.
How does your cath lab handle radiation protection for the physicians and staff?
There are several ways we protect our staff members from radiation exposure. Our physicians wear lead goggles and there is a lead barrier consisting of a drape and movable shield for added protection. All our staff, of course, wears lead tops and aprons.  We stress the rule of maintaining a safe distance without compromising the care of the patient, especially during long cases. The physicians will routinely come off of fluoroscopy if there are any patient needs that have to be addressed at the bedside. We also have mobile shields that we can place at the left side of the bed. We have modified our x-ray settings to minimize radiation to the patients and published some important research papers on this subject.2,3
We stress the rule of maintaining a safe distance without compromising the care of the patient, especially during long cases. The physicians will routinely come off of fluoroscopy if there are any patient needs that have to be addressed at the bedside. We also have mobile shields that we can place at the left side of the bed. We have modified our x-ray settings to minimize radiation to the patients and published some important research papers on this subject.2,3
What are some of the new equipment, devices and products recently introduced at your lab?
The Cleveland Clinic has been and remains on the cutting edge as far as new technology being used in invasive cardiac medicine today. We have multiple vendors in the lab daily and they keep the staff up to date on emerging technologies, including advances in and uses of peripheral, structural, and interventional techniques and equipment. We encourage trials of new devices and have a specific process in place for these trials, which involves supply chain management and proper 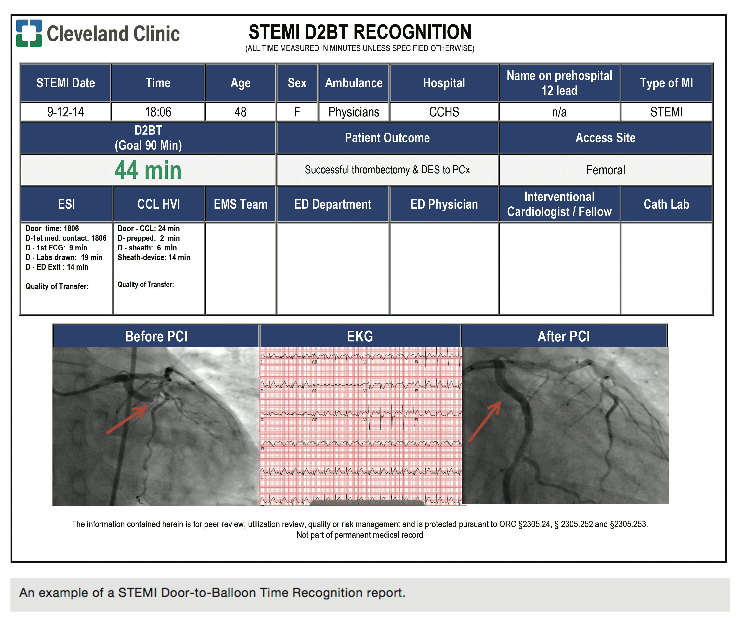 documentation of evaluation.
documentation of evaluation.
How does your lab communicate information to staff and physicians to stay organized and on top of change?
As we all know, communication is the key to success. Without communication, the lab would fail. In our lab, we have monthly staff meetings that cover the high-level information that the lab needs, such as human resources policy changes or other enterprise information needing updating. The cath lab also has daily 0700am huddles that are led by the charge nurse, assistant nurse manager, or nurse manager. This information is focused more on day-to-day issues. Huddles are also the time for staff to voice any concerns about any process or department. We also have several communication boards in the scrub room. These boards talk about the STEMI process along with posting recent STEMI times for door-to-balloon or door-to-door-to-balloon times. There are also scheduling boards that have the staff schedule and when the next schedule will be posted, along with when the schedule will be pulled. The last group of boards is in our break room. These boards are employee  engagement boards featuring the employee of the month along with employee birthday boards. Electronic communication boards are used in our lab to monitor patient flow between prep/recovery and the main cath lab.
engagement boards featuring the employee of the month along with employee birthday boards. Electronic communication boards are used in our lab to monitor patient flow between prep/recovery and the main cath lab.
Who pulls sheaths post procedure?
Diagnostic sheaths are either closed with a closure device or pulled post procedure in the prep/recovery area or in the procedure room. Post intervention sheaths are either closed with a closure device or pulled post procedure in the prep/recovery area. With increasing radial access, sheath burden has decreased. Patients with sheaths that remain in post interventional procedures later in the day will be admitted to the hospital. These sheaths will be pulled after the results of a partial thromboplastin time (PTT) test by the in-house night shift staff. All intensive care unit (ICU) patients who have had procedures and sheaths that remain in place will return to the ICU. Depending on the time of day, these sheaths will be pulled by the ICU fellow or night shift staff if available. Once a cath lab staff member has successfully pulled ten sheaths without issues, that team member is competent to perform the task independently. 
Where are patients prepped and recovered (post sheath removal)?
All to-come inpatients are prepped in the prep/recovery area. All in-house patients come to the prep/recovery area before entering the cath lab. All ICU patients come directly to the cath lab suite. Sheaths removed in the prep/recovery area are pulled by RNs. If a sheath needs to be removed in the cath lab suite, an RN or CVT may be responsible for removal of the sheath. Prep/recovery pulls 90-93% of the arterial sheaths the cath lab sends to them.
Has your cath lab recently expanded in size and patient volume, or will it be in the near future?
The growth of cath labs is in structural and peripheral cases. It is clear that these fields are expanding, and with the atrial appendage occlusion and mitral valve replacement technologies, the field will grow even further. Awareness of peripheral vascular disease and expanding minimally invasive treatment options with growing expertise is making this field emerge as another major area of growth for us.
Is your lab involved in clinical research?
Research is a major focus in the cath lab. We are involved in randomized trials of coronary, peripheral, and structural interventions. We also have registries of our own patients that provide another opportunity for investigations. We also encourage and perform site-initiated research projects. For several years, our cath lab attendings have published more than 100 manuscripts each year.
Can you share your lab’s average door-to-balloon (D2B) times?
Our most recent D2B median time from Q1 2015 is 43 minutes. We have achieved these best practices of D2B times <90 minutes with rapid feedback and recognition reporting of each STEMI patient, along with a diligent team of caregivers that attend a weekly STEMI huddle where a comprehensive review of each STEMI patient is completed. The same team meets once a month to discuss current month and quarterly American College of Cardiology National Data Registry (ACC-NCDR) CathPCI D2B outcomes. The Heart and Vascular Institute (HVI) has made tremendous developments in ensuring optimal outcomes with D2B times <90 minutes for our patients by developing close collaboration with our local emergency medical services (EMS), allowing emergency department (ED) physician STEMI activation, instituting an ED bypass system that allows EMS to bypass the ED and directly transport patients to the cath lab, and sustaining a 24/7 staffed cath lab, the first in northeast Ohio. The dynamic teams involved in providing world-class care to our patients consist of our HVI chief quality officer, Emergency Services Institute (ESI) quality officer, section head of invasive cardiology, interventional cardiologists, HVI and ESI quality directors, HVI assistant nursing director, cath lab and ED nurse managers, critical care transport, pharmacy, and the quality facilitator for registries and reporting.
Who transports the STEMI patient to the cath lab?
From the in-house ED, the ED nursing and/or medic team transports patients to the cath lab. A cardiology fellow and/or ED resident will also accompany the patient to the cath lab. When the ED bypass system is used, EMS will directly transport the patient to the cath lab. There are no off hours in our lab, since we are staffed 24/7/365. For in-house STEMIs, the nursing staff brings them down to the cath lab. Out-of-house STEMIs are flown in or come by critical care transport to the cath lab.
What do you do when the call team is already busy doing a procedure and a STEMI comes into the ED?
All STEMI cases during the hours of 7am-7pm that arrive to the ED are taken to the lab. The STEMI patient may be brought to the room of the on-call physician or to another open lab. If the two above options are not available, a back-up lab will be utilized and staff pulled to take care of the patient. On the off shift, there are only two people in-house, with the third staff member reporting in from home. If a STEMI patient arrives during an ongoing case, that patient will go to the cardiovascular ICU (CICU) until the team is available to take the patient to the lab. If the current case is close to completion, one team member, with the help of the Cardiac Medical Emergency Team (CMET), will be utilized to take the patient directly to the lab.
What quality measures are practiced in your cath lab?
Patients are able to review a number of metrics and outcomes related to quality, safety and patient experience on Medicare.gov’s Hospital Compare website. This enables patients to make an informed decision about where to seek care. Preventing hospital-acquired infections, avoiding and preventing harm to patients, advancing a safety culture, developing and implementing care coordination, improving clinical practices to drive outcomes, and delivering timely, efficient, effective, and equitable care across the continuum of care are safety and quality strategies across our organization. Applying evidence-based standards, maintaining volume standards, and consistent tracking of outcomes and complications are fundamental metrics tracked in our cardiac catherization lab.
The quality director serves as a leadership role to collaborate in the development and implementation of plans to drive improvement. Local owners and support resources from the cardiac cath lab implement and sustain the improvement activities.
Are you recording fluoroscopy times/dosages?
During each case, radiation exposures are displayed on the syngo imaging monitor (Siemens Healthcare). The staff member monitoring the case can update the team at regular intervals with real-time radiation exposure time and dosages. If the exposure level exceeds 5 Gy, an alarm notifies the monitor person, who then notifies the team, and especially the attending physician, that 5 Gy has been reached. If a patient’s radiation dosage exceeds 5 Gy during a case, the cardiology fellow provides follow-up teaching regarding possible complications that could occur due to an exposure of 5 Gy or more. In the rare instance that a patient reaches a dose of 10 Gy or higher, they are also given instructions regarding aftercare, but are also followed and monitored during their hospital stay for possible complications related to radiation exposure.
After each case, the Sensis system (Siemens Healthcare) automatically captures and calculates the total dosage. Dosages are monitored and recorded daily in a detailed fluoroscopy log that we submit to our radiation safety committee on a quarterly basis. Each cath film has a log of cine runs with amount of radiation used and can be easily accessed.
Who documents medication administration during the case?
All medication documentation is completed by the monitor staff member. This may be either an RN or a CVT.
Are your physicians dictating their cath procedure reports, or do they use a structured reporting tool?
We have a structured reporting system (syngo-based) that is customized for our use. We have been using these databases for several years. The cath reports are done as soon as the catheterization is finished and then finalized in the next few days.
Do you use the American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR) or any other outside data collection registry?
Yes, the Heart and Vascular Institute participates in the ACC-NCDR CathPCI Registry, as well as ICD, Impact, and the Society of Thoracic Surgeons (STS)/ACC Transcatheter Valve Therapy (TVT) and STS Adult Cardiac registries.
How are new employees oriented and trained at your facility?
Our team has implemented a unique, individualized orientation process that spans 18 months. The new staff member goes through a traditional orientation process that lasts 12 weeks, during which they are paired with an experienced preceptor. During this time period, the new staff member becomes acclimated to the lab. They are first introduced to diagnostic orientation. This allows the new staff member to become familiar with the cath lab’s processes, equipment, routine, and personnel. Diagnostic orientation typically lasts for 6 weeks. The new staff member then goes through another 6 weeks of interventional orientation, where they are introduced to more advanced theories such as stents, balloons, assist devices, STEMIs, etc.
After the completion of the 12-week orientation process, the new staff member is then counted in staffing, becoming an independently functioning staff member. From the period of 12 weeks to 1 year, they are typically paired with our more experienced cath lab staff until they feel completely comfortable in the unit. During this time, they participate in any and all of the types of cases done at the Clinic. At 12 months, they are again paired with an experienced structural heart preceptor, where they will focus on learning advanced structural theory including TAVRs, PFOs, paravalvular leak closures, and so on. After 3 months, they will spend an additional 3 months with a peripheral preceptor, and learn theories and procedures related to functioning independently in our peripheral diagnostic and interventional cases. We, as a team, decided on this process, because it allows new staff members learn and grow at a reasonable pace that fosters successful learning.
During the orientation process, the new staff member will meet weekly with the lab educator and the manager to make sure everyone is on the same page. The educator is also in the lab to assist with education such as advanced cardiac life support/basic life support (ACLS/BLS) as well as different technologies that are in the lab.
What continuing education opportunities are provided to staff members?
We provide our staff with multiple continuing education unit (CEU) opportunities. In cooperation with our equipment vendors, we have been able to provide excellent, high-level educational opportunities relating to advanced cardiac concepts. We also provide opportunities to our staff to go off-site to get super user training in order to become resources for the team.
How do you handle vendor visits to your lab?
- The vendor process in our lab is very specific.
- Vendors must be VendorMated.
- Representatives must wear orange scrubs.
- They must sign in the office whenever they are in the lab.
- They are required to make an appointment with the manager in order to introduce themselves and explain the reason for their visit.
- We have a table set up outside the lab specifically for representatives. This decreases the chance for clutter in the labs.
- Vendors need to schedule at least 4 hours a month for staff education. If they do not, they will not be allowed in the lab.
How is staff competency evaluated?
We have recently reviewed this issue and made some significant changes. We now have the equipment-specific vendors in the lab and available for teaching at least once a month. This gives our staff an opportunity to discuss issues, answer any questions they have regarding issues, and stay current with the latest technology as it becomes available. Also, the educator will assist in in-services to help make sure all staff is competent with all technology that is in our lab. We have unit-specific checklists for all technologies. When this checklist is completed, the staff is considered expert.
Does your lab have a clinical ladder?
The Cleveland Clinic has a clinical stepladder for all RNs that provides the opportunity for our staff to be recognized for accomplishments and education that goes above and beyond the required unit-specific requirements. RNs can move up to the next step annually by meeting criteria set forth by the Clinic. We highly encourage our staff to apply for the opportunity to participate in the clinical ladder program and make every effort to assist them in successfully submitting the required criteria material. We have seen a steady increase in RNs taking advantage of the career ladder. The career ladder has helped transform the cath lab by encouraging higher staff engagement.
How does your lab handle call time for staff members?
On-call is a maximum of 2 twelve-hour shifts in a 4-week period. Each team is comprised of a minumum of two RNs and a CVT, or three RNs. Of note, 2 call team members are in-house staff, so only one person comes from home. On-call team members are expected to arrive to the lab between 30-45 minutes from the activation of the page. Our rapid response team covers the lab until our third staff member arrives, which solidifies our teamwork philosophy and gives us the ability to take care of our STEMIs in a rapid manner.
Do you have flextime or multiple shifts?
No flextime is utilized in the lab. Staff members either work 2 eight-hour and 2 twelve-hour shifts per week, or 3 twelve-hour shifts per week.
Where is your cath lab located in relation to the operating room (OR) and emergency department (ED)?
The OR is located 2 floors directly above the cath lab. The emergency department is located in a different building, but is connected by walkways. It is a 4- to 5-minute walk from the ED to the lab.
What trends have you seen in your procedures and/or patient population?
We have seen some decline in stable coronary artery disease patients for coronary interventions. However, patients with acute MI, non ST-elevation MI, and complex coronary artery disease have increased in volume. There is a large increase in patients with aortic stenosis referred for TAVR. Our peripheral vascular disease volume is primarily from obstructive disease and is comprised of a large number of patients with critical limb ischemia. We have also seen an increase in this volume.
What is unique or innovative about your cath lab and staff?
1. STEMI program: The Cleveland Clinic has in-house staff 24/7/365. We have had D2B times in the low 20-minute range as a result.
2. Average first patient start times are in the 90% range.
3. Room turnaround times are around 16.1 minutes.
4. We have the ability to perform wide range of complex procedures safely and effectively.
What’s special about your city or general regional area in comparison to the rest of the U.S.? How does it affect your “cath lab culture”?
The Cleveland Clinic has been ranked as number one for treatment of cardiovascular diseases by U.S. News & World Report for the last 21 consecutive years. All workers in the cath lab, from technologists to nurses to fellows to attendings, are all very proud of this ranking and work hard to maintain our status. Passionate staff makes this cath lab a unique and pleasurable place to work.
References
- Kapadia SR, Svensson LG, Roselli E, Schoenhagen P, Popovic Z, Alfirevic A, et al. Single center TAVR experience with a focus on the prevention and management of catastrophic complications. Catheter Cardiovasc Interv. 2014 Nov 1; 84(5): 834-842. doi: 10.1002/ccd.25356.
- Agarwal S, Parashar A, Ellis SG, Heupler FA Jr, Lau E, Tuzcu EM, Kapadia SR. Measures to reduce radiation in a modern cardiac catheterization laboratory. Circ Cardiovasc Interv. 2014 Aug; 7(4): 447-455. doi: 10.1161/ CIRCINTERVENTIONS.114.001499.
- Agarwal S, Parashar A, Bajaj NS, Khan I, Ahmad I, Heupler FA Jr, Bunte M, Modi DK, Tuzcu EM, Kapadia SR. Relationship of beam angulation and radiation exposure in the cardiac catheterization laboratory. JACC Cardiovasc Interv. 2014 May; 7(5): 558-566. doi: 10.1016/j.jcin.2013.12.203.
A question from the American College of Cardiology’s National Cardiovascular Data Registry:
How do you use the NCDR Outcome Reports to drive quality improvement initiatives at your facility? 
Group risk-adjusted outcomes and case appropriateness are reviewed quarterly via the ACC-NCDR registry. Areas of concern are identified by the leadership, drill-down analyses performed as needed, and an action plan developed. Appropriate use criteria (AUC) data are supplemented by quantitative coronary analysis (QCA) from our Core Lab in conjunction with fractional flow reserve (FFR) data. Follow-up outcomes are then carefully reviewed for improvement. Numerous staff-specific, risk-adjusted outcomes (e.g. death, myocardial infarction, blood product usage, contrast-induced nephropathy) are tracked annually and on an as-needed basis. Similar processes for structural interventional cases have just been developed, and are under development for peripheral interventions. Major adverse outcomes are reviewed at a monthly morbidity and mortality conference or weekly cath conferences. Detailed processes to review product utilization in the catheterization laboratory on a per-staff basis are also reviewed.
The NCDR Institutional Outcomes Report provides us with the ability to trend performance data, benchmark outcomes, identify any potential areas of opportunity, and serve as a foundation to initiate quality improvement discussions with key stakeholders. With our current practice of weekly data submissions, we have to ability to stay up-to-date on key metrics such as door-to-balloon times, procedural complications, discharge medication compliance, monitor appropriateness of percutaneous coronary intervention, and more with the use of the NCDR online dashboard.
We routinely discuss these data in our staff meeting. We also have a dashboard that lets us see individual data. We are proactive in maintaining excellent outcomes. NCDR data are useful for benchmarking purposes.
The Society of Invasive Cardiovascular Professionals (SICP) has added two questions to our spotlight:
1. Do you require your clinical staff members to take the registry exam for Registered Cardiovascular Invasive Specialist (RCIS)? Does staff receive an incentive bonus or raise upon passing the exam?
Several staff members have obtained the RCIS credential, which was supported by prep classes and physicians. We continually encourage all cath staff to obtain RCIS education, which is not required at this time. If the x-ray technologists achieve the RCIS, they will be moved to a higher pay grade. We also have many RNs who hold and/or are going on for their BSN and also MSNs in nurse practitioner, education, or business disciplines.
2. Are your clinical and/or managerial team members involved with any professional organizations that support the invasive cardiology service line, such as the SICP, ACVP, or regional organizations?
Yes, the nurses, technologists and physicians are involved. We have leadership roles at all levels in different organizations. Some of the organizations where we are very active include the American College of Cardiology, American Heart Association, Society for Cardiovascular Angiography and Interventions, and the ACC-NCDR.
