


The SHIELD Study Leads to New Radiation Safety Initiatives in the Cath Lab at Spectrum Health
Accumulating evidence continues to link occupational radiation exposure in the cardiac catheterization laboratory with certain adverse health effects. Prior studies have suggested that interventional cardiologists may be at increased risk of developing posterior-subcapsular cataracts,1 premature carotid atherosclerosis,2 and left-sided brain malignancies.3 However, the adverse health effects of occupational radiation exposure may not be limited to interventional cardiologists; several studies have demonstrated certain radiation-related health risks among nurses and technologists. A recent meta-analysis investigating the risk of cataract demonstrated that nurses and technologists exposed to occupational radiation are at a roughly three-fold increased risk of cataracts compared to unexposed individuals.1 At least one study has demonstrated an increased risk of stroke among technologists performing fluoroscopically- guided interventional procedures.4 Some studies have even demonstrated an increased risk, albeit small, of breast cancer
among technologists,5,6 although this finding has not been consistently demonstrated in all studies.7 Taken collectively, the existing evidence at least raises the possibility that nurses and technologists could be at an increased risk of radiation-induced health effects. Consequently, it seems prudent to maximize radiation safety in an attempt to mitigate these risks.
The SHIELD Study
In order to further understand procedural factors associated with radiation doses among nurses and technologists during cardiac catheterization, we recently conducted the SHIELD (Combining Robotic-Stenting and Proactive Shielding Techniques in the Catheterization Laboratory to Achieve Lowest Possible Radiation Exposure to Physicians and Staff) study.8 In 764 consecutive cardiac catheterization procedures, the SHIELD study demonstrated that use of an accessory lead shield by nurses and technologists was associated with a nearly two-thirds reduction in staff radiation doses. Furthermore, cases involving percutaneous coronary intervention (PCI) or fractional flow reserve (FFR) were associated with 425% and 171% increases in the radiation doses to nurses, respectively. We speculated that the increased radiation doses observed among nurses during PCI and FFR arose from nurses approaching the patient to administer antiplatelet therapy, anticoagulants, and adenosine while fluoroscopy was in use.
These results from the SHIELD study have had an impact on the radiation safety culture in our laboratory. Prior to the SHIELD study, we lacked a uniform approach to radiation safety among our physicians, nurses, and technologists. Radiation safety was not regularly discussed at staff meetings and there was no recognition that our radiation safety practices might be suboptimal. When the SHIELD study uncovered the dramatic increases in radiation doses that our nurses were experiencing during PCI and FFR, there was a collective opinion in our laboratory that our approach to radiation safety could be improved. The results of the SHIELD study provided a platform for the staff to initiate change, but several challenges remained:
- How do you change an institutional radiation safety culture that has been established and engrained for so many years?
- How do you encourage physicians and staff members alike to care more about radiation safety?
- How do you empower staff members to be their own advocates for safety?
This article presents five initiatives that our staff members undertook in an attempt to positively impact the radiation safety culture in our laboratory.
Initiative #1: Forming a Radiation Safety Committee
 The first initiative we took to improve our radiation safety culture was to form a Radiation Safety Committee (RSC) specific to the catheterization laboratory that would convene monthly to address the challenges outlined above. In order for the committee to be most effective, it was decided that representation was needed from among all positions in the catheterization laboratory. Hence, an interventional cardiologist, two technologists, two nurses, and an individual from within the catheterization laboratory leadership, who could serve as the liaison between management and staff, were selected for the committee (Figure 1). At the first meeting of the RSC, a mission statement was developed: to make our laboratory a more radiation-safe environment by instituting changes in which staff, physicians, and patients would be exposed to less radiation. During its first year in existence, the RSC carried out initiatives #2-5 as described in the following paragraphs.
The first initiative we took to improve our radiation safety culture was to form a Radiation Safety Committee (RSC) specific to the catheterization laboratory that would convene monthly to address the challenges outlined above. In order for the committee to be most effective, it was decided that representation was needed from among all positions in the catheterization laboratory. Hence, an interventional cardiologist, two technologists, two nurses, and an individual from within the catheterization laboratory leadership, who could serve as the liaison between management and staff, were selected for the committee (Figure 1). At the first meeting of the RSC, a mission statement was developed: to make our laboratory a more radiation-safe environment by instituting changes in which staff, physicians, and patients would be exposed to less radiation. During its first year in existence, the RSC carried out initiatives #2-5 as described in the following paragraphs.
Initiative #2: Increasing the Availability and Consistent Use of Lead Shields
 Based on the observation from the SHIELD study that use of an accessory lead shield was associated with a nearly two-thirds reduction in radiation doses received by staff members, the RSC set out to increase the availability of accessory lead shields in our laboratory and to encourage their consistent use in all cases. Two barriers had to be overcome for this initiative to be successful. First, our laboratory did not have enough accessory shields for simultaneous use in each of our catheterization laboratory rooms. The RSC overcame this barrier by using the results of the SHIELD study to convince the hospital administration to purchase a dedicated mobile accessory lead shield for each of our rooms. Second, we found that some nurses were initially reluctant to use the shields, as they felt it was difficult to reach the medication pump on the IV pole while standing behind the shield. To address this barrier, one of the RSC members designed a mount on the lead shield that was capable of housing the medication pump (Figure 2). This simple alteration of the lead shields has led to their more consistent and widespread use by our nurses.
Based on the observation from the SHIELD study that use of an accessory lead shield was associated with a nearly two-thirds reduction in radiation doses received by staff members, the RSC set out to increase the availability of accessory lead shields in our laboratory and to encourage their consistent use in all cases. Two barriers had to be overcome for this initiative to be successful. First, our laboratory did not have enough accessory shields for simultaneous use in each of our catheterization laboratory rooms. The RSC overcame this barrier by using the results of the SHIELD study to convince the hospital administration to purchase a dedicated mobile accessory lead shield for each of our rooms. Second, we found that some nurses were initially reluctant to use the shields, as they felt it was difficult to reach the medication pump on the IV pole while standing behind the shield. To address this barrier, one of the RSC members designed a mount on the lead shield that was capable of housing the medication pump (Figure 2). This simple alteration of the lead shields has led to their more consistent and widespread use by our nurses.
Initiative #3: Getting Vocal to Protect Nurses
The observation from the SHIELD study that PCI and FFR were associated with significant increases in nurse radiation doses raised the concern that our nurses may be frequently approaching the patient to administer medications while fluoroscopy was in use. The RSC recognized that improved communication between staff members and physicians was a key component in addressing this problem and that all members of the laboratory team were responsible for speaking up to protect each other against unnecessary radiation exposure. To help promote these changes in our laboratory, the RSC implemented several new quality standards. One new standard was that the pre-procedural time-out was modified to include verification that all physicians, technologists, and nurses in the room are properly leaded and wearing their radiation dosimeters prior to enabling fluoroscopy. Another new standard involved making the scrub technologist in each case responsible for disabling fluoroscopy anytime personnel not wearing lead apparel entered the room. Finally, and perhaps most importantly, nurses and technologists are now expected to both verbally notify the physician when the need arises for the nurse to approach the patient. This improved communication, which includes technologists speaking up to enhance the safety of our nurses, ensures that the physician is given adequate verbal notification from multiple individuals to step off the fluoroscopy pedal prior to the nurse approaching the table.
Initiative #4: Tracking Radiation Doses and Providing Peer Comparisons
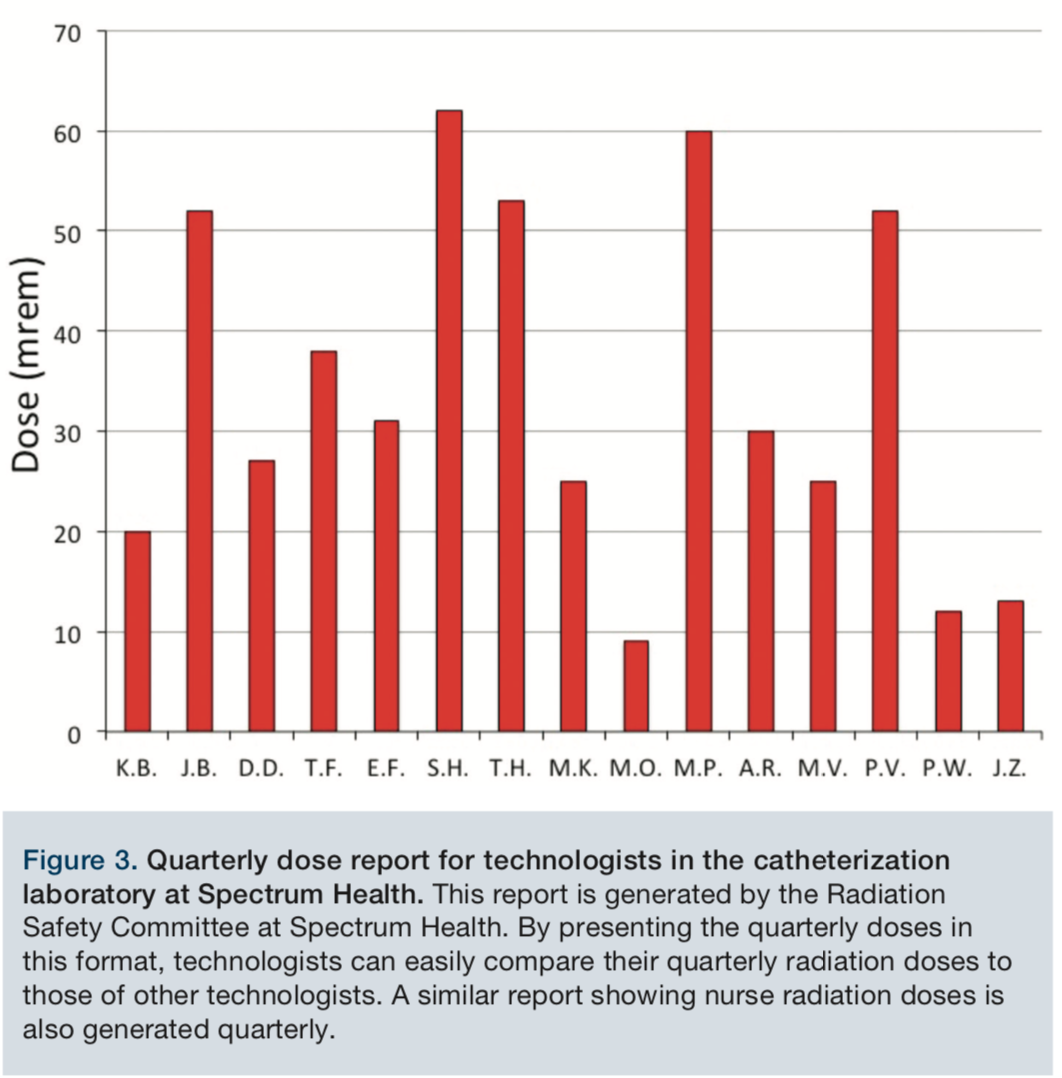 Radiation exposure data for our staff members have always been tracked by our institutional radiation safety officer and posted in the laboratory in the form of a quarterly report generated by the dosimeter company. Although informative, this quarterly report presents data in a table containing the doses of physicians, nurses, and technologists in a manner that does not facilitate easy comparisons between staff members and their peers. Furthermore, staff members in our laboratory rarely checked their doses on these reports and there was not regularly occurring discussion about these doses amongst team members. To address these limitations, the RSC began to collect the data from these quarterly reports and present them to nurses and technologists in a more simplified manner (Figure 3). This provided nurses and technologists the opportunity to compare their quarterly radiation doses with those of their peers and also allowed the RSC to determine whether the radiation safety initiatives being implemented were impacting radiation doses across the laboratory. The RSC radiation dose reports are now prominently displayed on a central communication board in the laboratory and are also discussed periodically in morning staff huddles. Furthermore, for individuals identified to have high quarterly doses relative to their peers, the RSC has provided additional education on methods to reduce exposure, even if the high quarterly doses are below the occupational limits. For those with low doses relative to their peers, the RSC has encouraged those individuals to share their behaviors with other staff members periodically at the morning huddle. We have found this collaborative team-based approach, which in some cases has led to behavior modification, to be effective in further engaging staff members to take greater interest in their own radiation protection and in the protection of their colleagues.
Radiation exposure data for our staff members have always been tracked by our institutional radiation safety officer and posted in the laboratory in the form of a quarterly report generated by the dosimeter company. Although informative, this quarterly report presents data in a table containing the doses of physicians, nurses, and technologists in a manner that does not facilitate easy comparisons between staff members and their peers. Furthermore, staff members in our laboratory rarely checked their doses on these reports and there was not regularly occurring discussion about these doses amongst team members. To address these limitations, the RSC began to collect the data from these quarterly reports and present them to nurses and technologists in a more simplified manner (Figure 3). This provided nurses and technologists the opportunity to compare their quarterly radiation doses with those of their peers and also allowed the RSC to determine whether the radiation safety initiatives being implemented were impacting radiation doses across the laboratory. The RSC radiation dose reports are now prominently displayed on a central communication board in the laboratory and are also discussed periodically in morning staff huddles. Furthermore, for individuals identified to have high quarterly doses relative to their peers, the RSC has provided additional education on methods to reduce exposure, even if the high quarterly doses are below the occupational limits. For those with low doses relative to their peers, the RSC has encouraged those individuals to share their behaviors with other staff members periodically at the morning huddle. We have found this collaborative team-based approach, which in some cases has led to behavior modification, to be effective in further engaging staff members to take greater interest in their own radiation protection and in the protection of their colleagues.
Initiative #5: Radiation Safety Education
 With the belief that periodic education and frequent reminders might lead to more consistent use of safe radiation practices among physicians and staff members, the RSC undertook several initiatives aimed to keep our physicians and staff members thinking about radiation safety. One approach was to identify several radiation safety behaviors that the RSC wanted to engrain in our laboratory’s safety culture. Each month, one of these radiation safety behaviors is selected by the RSC as the focused behavior for that month. For example, in January 2018 the RSC “safety behavior of the month” was to “keep the image intensifier as low as possible to the patient in order to reduce the radiation dose”. This behavior was discussed daily in the morning huddle (Figure 4) and posted using colorful signs on the doors leading into all of our procedure rooms as a visual reminder to our physicians and staff members. Another educational initiative instituted by the RSC was to make real-time dosimeters (RaySafe i2, Unfors RaySafe) available to staff members for personal use. These real-time dosimeters provide the wearer the opportunity to see their radiation doses in real-time on a bedside monitor during the course of a case. Hence, while wearing the badge, staff members are able to learn which of their personal behaviors increases radiation exposure and which behaviors limit exposure.
With the belief that periodic education and frequent reminders might lead to more consistent use of safe radiation practices among physicians and staff members, the RSC undertook several initiatives aimed to keep our physicians and staff members thinking about radiation safety. One approach was to identify several radiation safety behaviors that the RSC wanted to engrain in our laboratory’s safety culture. Each month, one of these radiation safety behaviors is selected by the RSC as the focused behavior for that month. For example, in January 2018 the RSC “safety behavior of the month” was to “keep the image intensifier as low as possible to the patient in order to reduce the radiation dose”. This behavior was discussed daily in the morning huddle (Figure 4) and posted using colorful signs on the doors leading into all of our procedure rooms as a visual reminder to our physicians and staff members. Another educational initiative instituted by the RSC was to make real-time dosimeters (RaySafe i2, Unfors RaySafe) available to staff members for personal use. These real-time dosimeters provide the wearer the opportunity to see their radiation doses in real-time on a bedside monitor during the course of a case. Hence, while wearing the badge, staff members are able to learn which of their personal behaviors increases radiation exposure and which behaviors limit exposure.
Conclusions
The radiation safety initiatives described in this article have seemingly led to positive changes in the radiation safety culture in our laboratory. We believe these changes have made a significant impact in making our laboratory a safer environment for staff members. After witnessing the impact that these initiatives have had on the radiation safety culture within our laboratory, we hope sharing them might lead to the adoption of similar initiatives in other laboratories around the world.
References
- Elmaraezy A, Morra ME, Mohammed AT, et al. Risk of cataract among interventional cardiologists and catheterization lab staff: a systematic review and meta-analysis. Catheter Cardiovasc Interv. 2017; 90: 1-9.
- Andreassi MG, Piccaluga E, Gargani L, Sabatino L, Borghini A, Faita F, Bruno RM, Padovani R, Guagliumi G, Picano E. Subclinical carotid atherosclerosis and early vascular aging from long-term low-dose ionizing radiation. J Am Coll Cardiol Intv. 2015; 8: 616-627.
- Roguin A, Goldstein J, Bar O, Goldstein JA. Brain and neck tumors among physicians performing interventional procedures. Am J Cardiol. 2013; 111: 1368-1372.
- Rajaraman P, Doody MM, Yu CL, et al. Incidence and mortality risks for circulatory diseases in US radiologic technologists who worked with fluoroscopically guided interventional procedures, 1994-2008. Occup Environ Med. 2016; 73: 21-27.
- Doody MM, Freedman DM, Alexander BH, et al. Breast cancer incidence in US radiologic technologists. Cancer. 2006; 106: 2707-2715.
- Preston DL, Kitahara CM, Freedman DM, et al. Breast cancer risk and protracted low-to-moderate dose occupational radiation exposure in the US radiologic technologists cohort, 1983-2008. British J Cancer. 2016; 115: 1105-1112.
- Boice JD Jr, Mandel JS, Doody MM. Breast cancer among radiologic technologists. JAMA. 1995; 274: 394-401.
- Madder RD, LaCombe A, VanOosterhout S, et al. Radiation exposure among scrub technologists and nurse circulators during cardiac catheterization. J Am Coll Cardiol Intv. 2018; 11: 206-212.
