


Reducing Radiation in the Cath Lab Using a Novel, Eye-Controlled, Moveable Region of Interest
As interventional procedures become more complex, how are we focusing on the importance of radiation safety?
 The more traditional focus, which I remember from the time of my fellowship a long time ago, was that everybody kept telling us, don’t take too many cine angiogram views. Work on fluoro. This was a way to reduce radiation at the time. We were interacting with radiation physicists once a year or so, but obviously they had so many other things to do throughout all the hospital laboratories, so their attention was expectedly limited in the cath lab. We had a rather poor understanding of what the values or measures of radiation we were paying attention to meant. We were mostly working with fluoro time or procedure time. It was very basic. As the procedures have gotten more complex, several things have happened. The equipment has gotten better and more sophisticated. We have ended up requiring less and less cine angiography, because we are more experienced in what to look at, and also as the result of medical education. The timing and the steps have been streamlined. A lot of the work that has been done has been on fluoro, and at the same time, we do many new types of procedures that require very non-standard positions at the table, such as valve procedures and vascular procedures, all of which have increased tremendously. The classic teaching doesn’t exactly fit for these procedures. For all these reasons, from a procedure point of view, we need to modernize how we deal with radiation. There are two layers of concern. One is radiation exposure to the patient, and the second is occupational exposure to the operator and team during all our procedures. Obviously those go hand-in-hand, because if we reduce our exposure, we reduce the exposures of each and every patient we treat.
The more traditional focus, which I remember from the time of my fellowship a long time ago, was that everybody kept telling us, don’t take too many cine angiogram views. Work on fluoro. This was a way to reduce radiation at the time. We were interacting with radiation physicists once a year or so, but obviously they had so many other things to do throughout all the hospital laboratories, so their attention was expectedly limited in the cath lab. We had a rather poor understanding of what the values or measures of radiation we were paying attention to meant. We were mostly working with fluoro time or procedure time. It was very basic. As the procedures have gotten more complex, several things have happened. The equipment has gotten better and more sophisticated. We have ended up requiring less and less cine angiography, because we are more experienced in what to look at, and also as the result of medical education. The timing and the steps have been streamlined. A lot of the work that has been done has been on fluoro, and at the same time, we do many new types of procedures that require very non-standard positions at the table, such as valve procedures and vascular procedures, all of which have increased tremendously. The classic teaching doesn’t exactly fit for these procedures. For all these reasons, from a procedure point of view, we need to modernize how we deal with radiation. There are two layers of concern. One is radiation exposure to the patient, and the second is occupational exposure to the operator and team during all our procedures. Obviously those go hand-in-hand, because if we reduce our exposure, we reduce the exposures of each and every patient we treat.
What are some of the daily, practical reminders of radiation exposure for those in the lab? How are we trying to keep the idea of radiation reduction in the forefront of people’s minds?
 First of all, there are certain alarms in the room. We get an audible alarm every 30 seconds of fluoro. We can get a visual alarm or even a shutdown alarm of the equipment system if somehow the equipment has overheated from a certain amount of radiation. Those are indirect messages, because they are equipment-driven. If our position has been a little different for a procedure, we may have more or less radiation than those alarms indicate. If you get an audible alarm, you have to make an effort to stop it, therefore reminding you that maybe your fluoro time has been a little bit in excess. In addition, we have the more active alarms by our nursing and technologist, depending per laboratory how they assign this role. There is an indicator somewhere in the control room that shows the radiation, and if the threshold is about to be reached, we have reminders. Let’s say if the threshold is 5, we have reminders from 3: you’ve reached 3, you may be reaching 5 soon, just start to finish up if you can or take it into account for what you are planning. If we do a certain lesion and are finishing up, and we are at 3.5, we are not going to undertake another lesion and risk a very high radiation exposure. This is manageable. We can interrupt and finish off, so to speak, our part later. The more difficult part is if we are doing some long procedure, such as a chronic total occlusion, where you anticipate significant radiation, but at the same time it is very hard to abruptly interrupt the procedure solely based on radiation. We still attempt to manage exposure by changing the camera views and so on.
First of all, there are certain alarms in the room. We get an audible alarm every 30 seconds of fluoro. We can get a visual alarm or even a shutdown alarm of the equipment system if somehow the equipment has overheated from a certain amount of radiation. Those are indirect messages, because they are equipment-driven. If our position has been a little different for a procedure, we may have more or less radiation than those alarms indicate. If you get an audible alarm, you have to make an effort to stop it, therefore reminding you that maybe your fluoro time has been a little bit in excess. In addition, we have the more active alarms by our nursing and technologist, depending per laboratory how they assign this role. There is an indicator somewhere in the control room that shows the radiation, and if the threshold is about to be reached, we have reminders. Let’s say if the threshold is 5, we have reminders from 3: you’ve reached 3, you may be reaching 5 soon, just start to finish up if you can or take it into account for what you are planning. If we do a certain lesion and are finishing up, and we are at 3.5, we are not going to undertake another lesion and risk a very high radiation exposure. This is manageable. We can interrupt and finish off, so to speak, our part later. The more difficult part is if we are doing some long procedure, such as a chronic total occlusion, where you anticipate significant radiation, but at the same time it is very hard to abruptly interrupt the procedure solely based on radiation. We still attempt to manage exposure by changing the camera views and so on.
You have been involved in a study with the eye-tracking dose reduction technology from ControlRad. Can you explain what that is?
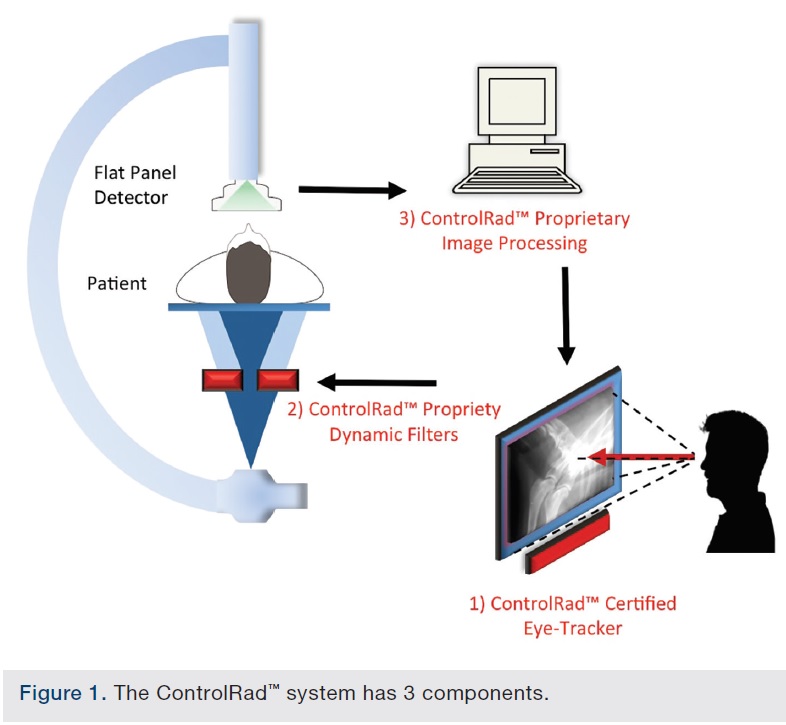
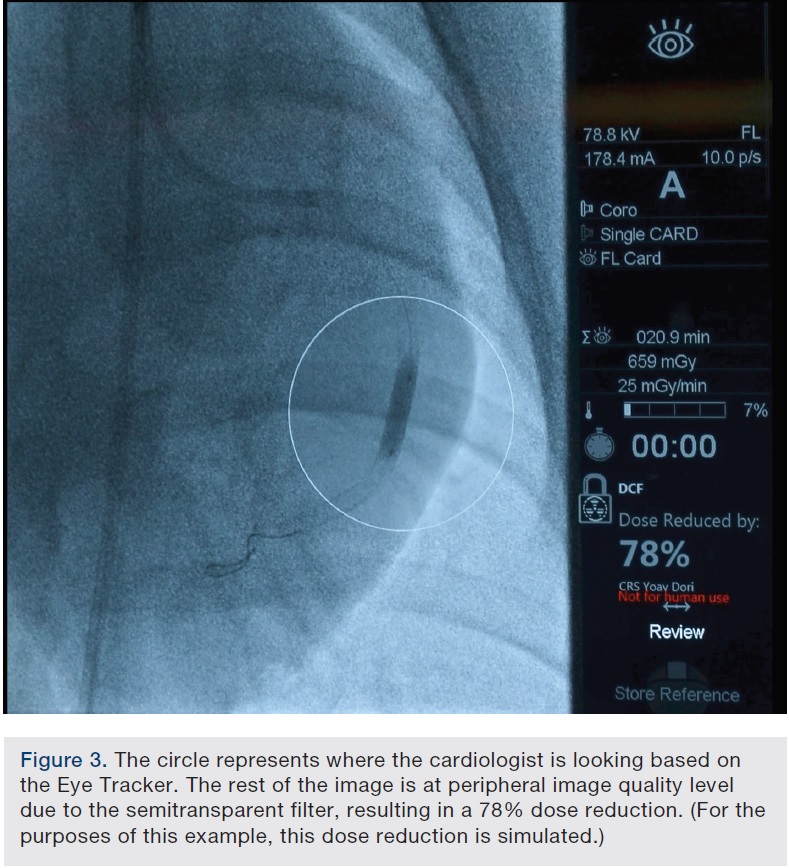 The basic principle capitalizes on how our visual system is designed. Only 5% of our field-of-view is clear; the rest is in our periphery. Yet we use the same amount of x-ray on the entire image, even though we can’t see it all at once. During an interventional procedure, although we want to know our surroundings, 90% of the time during fluoroscopy, we are focused specifically on the blockage itself. We are either passing wires, putting a stent or putting a balloon, or doing atherectomy, but essentially we are focused on a rather limited part of the screen. What if we could track where we were looking and focus the x-ray beam only where it is needed? That is the trick of this technology. It is able to track our eyes to determine where we are looking. It then moves, in real time, a semi-transparent filter that is above the tube in order to deliver perfect resolution where we need it, while delivering less radiation where we don’t need it — the part of the image that we aren’t looking at and that is in our peripheral vision. The end result is a 75% radiation dose reduction. For example, if the tip of the catheter is moving and I notice it in my peripheral vision, I will move my gaze to the catheter. The eye tracker will adjust its on-the-fly transparent filters to provide perfect resolution wherever I am looking, while keeping the rest of the image at a peripheral level image quality.
The basic principle capitalizes on how our visual system is designed. Only 5% of our field-of-view is clear; the rest is in our periphery. Yet we use the same amount of x-ray on the entire image, even though we can’t see it all at once. During an interventional procedure, although we want to know our surroundings, 90% of the time during fluoroscopy, we are focused specifically on the blockage itself. We are either passing wires, putting a stent or putting a balloon, or doing atherectomy, but essentially we are focused on a rather limited part of the screen. What if we could track where we were looking and focus the x-ray beam only where it is needed? That is the trick of this technology. It is able to track our eyes to determine where we are looking. It then moves, in real time, a semi-transparent filter that is above the tube in order to deliver perfect resolution where we need it, while delivering less radiation where we don’t need it — the part of the image that we aren’t looking at and that is in our peripheral vision. The end result is a 75% radiation dose reduction. For example, if the tip of the catheter is moving and I notice it in my peripheral vision, I will move my gaze to the catheter. The eye tracker will adjust its on-the-fly transparent filters to provide perfect resolution wherever I am looking, while keeping the rest of the image at a peripheral level image quality.
Does the operator wear eyewear?
No, you don’t need to wear anything. When I have used the system, I wear my protective radiation eyeglasses. Others have not. It tracks the eyes. So it works with whatever you usually wear.
When you begin a procedure, do you have to check in with the system, so it makes sure to capture your eye movements?
You have to do one calibration to adjust for your eyes, which is then stored in the system. After that, for every procedure, you spend a few seconds to communicate with the system, and then it starts tracking you. This was my experience in the various experiments where I have either been present or directly involved. You have the capacity, if you don’t want the system in use any more or for some reason you really want to pay attention to everything on the monitor, to turn it off immediately. It then returns to 100% radiation on the entire field of view.
Let’s say you do make a dramatic change in where you are looking onscreen. Are you waiting a beat for the system to follow you?
It happens immediately. There may be some milliseconds of delay, but it is definitely under my eyesight detection threshold.
Can you tell us about the study and whether it quantified a reduction in radiation with system use?
We conducted a study1 to quantify the dose reduction with the use of the eye tracker system. We performed coronary angioplasty and stenting in animals, comparing dose with and without the use of the eye tracker system. The procedures included wire passage and all the various steps. The eye tracking dose reduction technology demonstrated a 75% reduction in the radiation exposure measures. There were multiple measurements, because essentially this was a radiation physics study, not a clinical study. A special radiation physicist provided various detectors in multiple areas and all showed a significant level of reduction throughout the procedures. At the same time, we were able to perform the procedure very easily, without noticeable delays as we were looking at various parts of the screen.
So there isn’t any burden on the operator in terms of workflow, other than the initial system check-in.
That is correct. You do have an option to turn the system on and off, so if you don’t want it at a certain point, you can turn it off, and if you want it back, you can enable it again. There has also been some development of a touch-screen method, where you can draw a circle or rectangle on the screen as an alternative to the eye tracker. You can mark on the screen that you want a certain area maintained. It may be helpful in very long cases such as chronic total occlusions, when there may be multiple operators involved.
What do you anticipate as the future of this technology?
This technology will be extremely helpful to reduce radiation during fluoroscopy. It could be of significant benefit to patients, because they will also benefit from less radiation. After all, the patient is the one that is extremely close to the radiation source. At the same time, it will significantly reduce the burden on the entire operating team. Patient radiation reduction and operating team radiation reduction should be a very big motivation to eliminate any obstacles that need to be overcome.
Reference
- Balter S, Simon D, Itkin M, Granada JF, Melman H, Dangas G. Significant radiation reduction in interventional fluoroscopy using a novel eye controlled movable region of interest. Med Phys. 2016 Mar; 43(3): 1531-1538.
Disclosure: Dr. Dangas reports he is a non-financial advisor to ControlRad.
Dr. George Dangas can be contacted at george.dangas@mountsinai.org.
