


Protecting the Provider: A Reexamination of Cath Lab Radiation Safety
 In the delivery of high-quality healthcare, patient safety is always a major concern of providers and the public. The safety of healthcare workers frequently receives significantly less attention. Recent events have highlighted this issue and are altering this perspective, with greater recognition of the sacrifices and risks that healthcare workers routinely take to perform their jobs. Patient safety remains the number-one concern of healthcare providers. However, the health and safety of providers should receive equal attention, particularly when novel techniques and strategies can be adopted to mitigate provider risk.
In the delivery of high-quality healthcare, patient safety is always a major concern of providers and the public. The safety of healthcare workers frequently receives significantly less attention. Recent events have highlighted this issue and are altering this perspective, with greater recognition of the sacrifices and risks that healthcare workers routinely take to perform their jobs. Patient safety remains the number-one concern of healthcare providers. However, the health and safety of providers should receive equal attention, particularly when novel techniques and strategies can be adopted to mitigate provider risk.
During 2014, the Ebola patients treated within U.S. borders caught the attention of the mainstream media and the public. Besides the public’s general concern for the patients, much attention was devoted to the healthcare workers who were exposed to the virus while caring for Ebola patients. These events raised the public’s awareness of healthcare worker safety and also caused many people to ask: “How do we ensure the safety of healthcare providers who put themselves in harm’s way to look after their patients’ health?”
 This increased awareness is especially relevant to interventional cardiologists. Unlike patients, who are only exposed to ionizing radiation during their procedure, interventional cardiologists and other members of the cath lab team are repeatedly exposed to ionizing radiation, subjecting them to potentially serious long-term health issues. Additionally, the physical demands of performing their jobs while wearing heavy protective gear can lead to chronic orthopedic conditions that may prematurely end careers or force change into other fields of medicine.
This increased awareness is especially relevant to interventional cardiologists. Unlike patients, who are only exposed to ionizing radiation during their procedure, interventional cardiologists and other members of the cath lab team are repeatedly exposed to ionizing radiation, subjecting them to potentially serious long-term health issues. Additionally, the physical demands of performing their jobs while wearing heavy protective gear can lead to chronic orthopedic conditions that may prematurely end careers or force change into other fields of medicine.
With the increased interest in healthcare worker safety, it is an appropriate time to explore the risks associated with cath lab environments and novel technological solutions available to improve safety.
Assessing cath lab risks
 Medical procedures performed in the cath lab are a leading source of occupational ionizing radiation exposure for medical personnel1, due to the use of fluoroscopy and cine angiography during these procedures. This occupational radiation exposure is of particular concern because today’s interventional cardiologists are spending significantly greater time in the cath lab doing more complex and lengthy procedures. Further, the performance of percutaneous coronary intervention (PCI) procedures in cath labs has increased more than 50 percent since 20002, potentially exposing interventional cardiologists to additional radiation.
Medical procedures performed in the cath lab are a leading source of occupational ionizing radiation exposure for medical personnel1, due to the use of fluoroscopy and cine angiography during these procedures. This occupational radiation exposure is of particular concern because today’s interventional cardiologists are spending significantly greater time in the cath lab doing more complex and lengthy procedures. Further, the performance of percutaneous coronary intervention (PCI) procedures in cath labs has increased more than 50 percent since 20002, potentially exposing interventional cardiologists to additional radiation.
Although research studies have demonstrated substantial variations in the amount of ionizing radiation to which interventional cardiologists are exposed, a look at the literature reveals the following:
- One study showed that an interventional cardiologist’s head and neck area are generally exposed to approximately 20 to 30 millisieverts (mSv) per year3, which equates to 2 to 3 rems per year.
- Another demonstrated that cumulative doses for the average interventional cardiologist after 30 years in the cath lab fall between 50 to 200 mSv, equivalent to 5 to 20 rems, or 2,500 to 10,000 chest x-rays.4
- A third shows that interventionalists receive approximately 1 to 3 sieverts (Sv) to their head during their career (equivalent to 1,000 to 3,000 mSv, or 100 to 300 rems), which corresponds to about 500mSv to the brain5 (equivalent to 50 rems).
- A separate study showed that interventional cardiologists have a radiation exposure rate documented to be two to ten times higher than that of diagnostic radiologists.4

Adverse health effects
Despite the availability and use of personal protective equipment (PPE), such as lead aprons, leaded glasses and thyroid collars, there are significant radiation exposure risks that have the potential to negatively impact the health of interventional cardiologists and their staff. Below are some findings from recent scientific literature:
- Cataracts: The Occupational Cataracts and Lens Opacities in Interventional Cardiology (O’CLOC) study revealed that 50 percent of interventional cardiologists and 41 percent of cardiac cath nurses and technologists had significant posterior subcapsular lens changes, a precursor to cataracts, which is typical of ionizing radiation exposure.6
- Thyroid disease: Studies have reported structural and functional changes of the thyroid as a result of radiation exposure.7 Structural changes such as malignant and benign thyroid tumors develop at a linear rate to dose exposure. Functional changes that would result in hyper- or hypo-thyroidism were noted at elevated doses of external and internal radiation exposure.7
- Brain tumors and brain disease: A recent study focused on interventionalists who had been diagnosed with a variety of brain tumors. The study revealed that 86% of the brain tumors (where location is known) originated on the left side of the brain.8 This is significant, since interventional cardiologists typically stand with the left side of their body closest to the X-ray source and scattered radiation. In the general population, brain tumors originate with equal frequency on the left and right hemispheres.
- Cardiovascular changes: Recent studies suggest evidence of a link between low- to moderate-dose radiation exposure and cardiovascular changes, despite personal protective wear.5
- Reproductive health effects: For males, ionizing radiation has demonstrated a reduction in sperm.9 Additionally, cath lab staff members who may become pregnant while working in the cath lab must also take into consideration the effects that ionizing radiation can have on the developing fetus.
Additionally, there are orthopedic-related consequences from the heavy weight of lead gear worn by interventional cardiologists. The repeated standing and leaning over patients during procedures is fatiguing and commonly leads to chronic orthopedic conditions. A 2006 survey conducted by the Society for Cardiovascular Angiography and Interventions (SCAI) disclosed that interventional cardiologists suffer from a disproportionate amount of back, hip, and knee injuries leading to a significant amount of missed workdays.10 The weight of the personal protective gear is fatiguing, and a physician who is fatigued or experiencing discomfort may be more likely to be distracted or rush through a procedure.
Protecting the health of cath lab employees
There are two traditional techniques used to reduce radiation exposure. One is lead-based shielding, and the second is increasing the distance between the operator and the radiation source.
A relatively new approach to shielding includes devices that support lead aprons that hang from a boom, rather than being worn by clinicians. These hanging aprons provide effective radiation protection with a greater quantity of lead than is traditionally worn by operators. Since the operator is not physically supporting the lead, these devices have the potential to reduce orthopedic injuries and reduce overall operator fatigue.
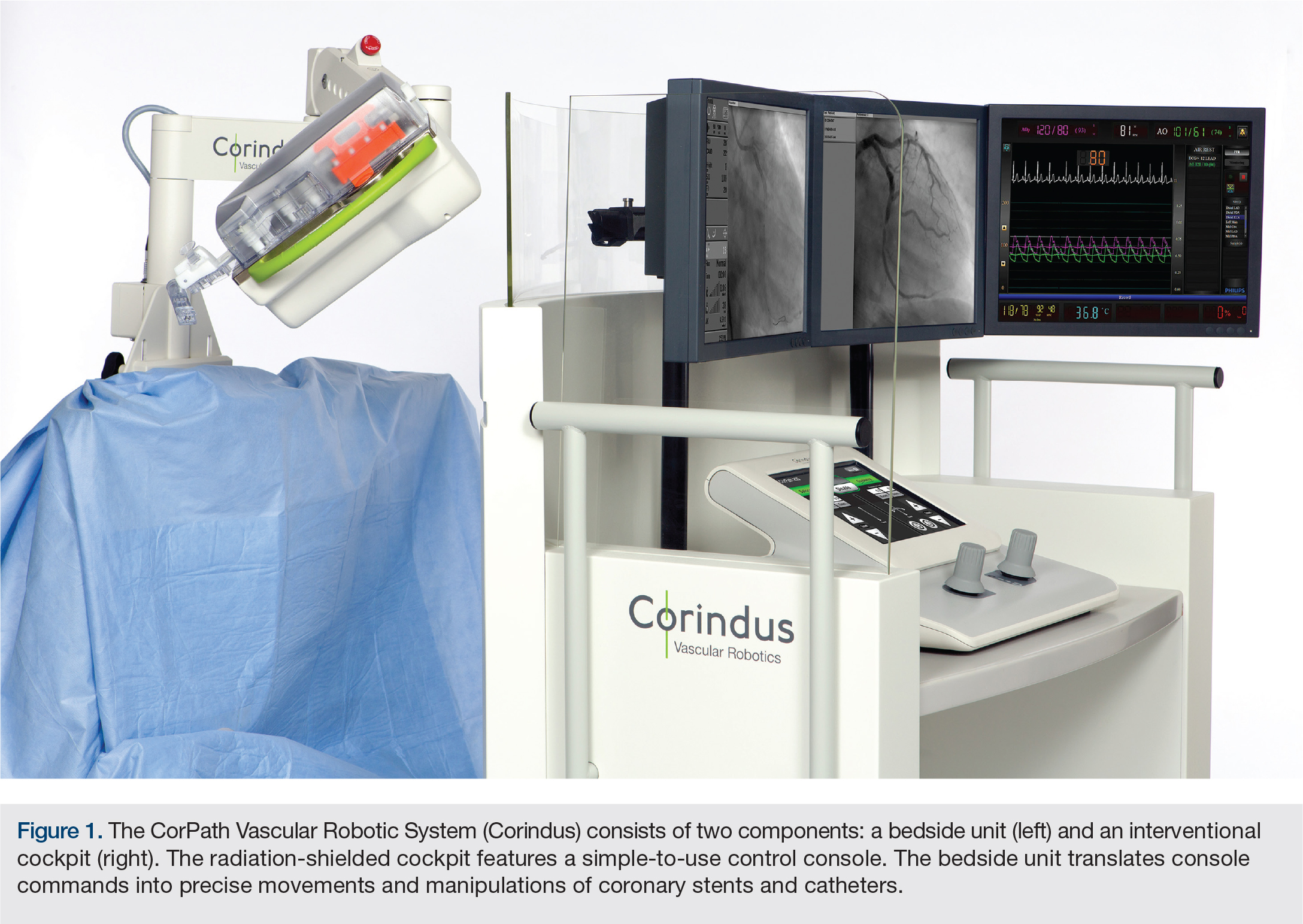
The advent of robot-assisted percutaneous coronary intervention (PCI) represents another novel approach to reducing radiation exposure to operators. Robotic systems for PCI allow interventional cardiologists to perform procedures remotely, away from the patient’s bedside. Seated in a radiation-protected cockpit, the physician uses digital controls to robotically manage catheters, guide wires, angioplasty balloons, and stents to clear blockages and restore blood flow. These technologies are beneficial in reducing exposure by positioning operators further from the radiation source, but also have the potential to mitigate the impact that wearing PPE has on operators, such as orthopedic pain, missed work and disability.
The robotic-assisted PCI system being used at Spectrum Health is called CorPath (Corindus Vascular Robotics). The CorPath System allows physicians to perform PCI procedures from the comfort of a radiation-shielded cockpit that includes angiographic and hemodynamic monitors. Physicians using the system are able to take measurements, with sub-millimeter accuracy, of relevant anatomy, as well as advance or retract guide wires and/or balloon stent catheters with movements as small as a millimeter. A clinical trial has shown that using the robotic system reduced radiation exposure to the primary operator by more than 95 percent.11
Elevating healthcare worker safety
Interventional cardiology is a uniquely rewarding, highly innovative profession. The bulk of the innovation in our field over the past 3 decades has appropriately been focused on patient care. However, the manner and circumstances with which that care has been delivered in the cath lab has changed little over time. New approaches are now available to begin to mitigate the biomechanical, orthopedic, and radiation risks of working in the cath lab. The CorPath System is an example of a device with tremendous promise to reduce these hazards for interventional cardiologists, contributing to longer, healthier careers. We have been excited to bring this innovative technology to our cath labs as part of the evolution of our environment.
References
- Sun Z, AbAziz A, Yusof AK. Radiation-induced noncancer risks in interventional cardiology: optimisation of procedures and staff and patient dose reduction. Biomed Res Int. 2013; 2013: 976962. doi: 10.1155/2013/976962.
- Best PJ, Skelding KA, Mehran R, Chieffo A, Kunadian V, Madan M, et al; Society for Cardiovascular Angiography & Interventions’ Women in Innovations (WIN) Group. SCAI consensus document on occupational radiation exposure to the pregnant cardiologist and technical personnel. Catheter Cardiovasc Interv. 2011 Feb 1; 77(2): 232-241. doi: 10.1002/ccd.22877.
- L Renaud. A 5-y follow-up of the radiation exposure to in-room personnel during cardiac catheterization. Health Phys. 1992 Jan; 62(1): 10-15.
- Picano E, Andreassi MG, Piccaluga E, Cremonesi A, Guagliumi G. Occupational risks of chronic low dose radiation exposure in cardiac catheterisation laboratory: the Italian Healthy Cath Lab study. EMJ Int Cardiol. 2013; 1: 50-58.
- Picano E, Vano E, Domenici L, Bottai M, Thierry-Chef I. Cancer and non-cancer brain and eye effects of chronic low-dose ionizing radiation exposure. BMC Cancer. 2012 Apr 27; 12: 157. doi: 10.1186/1471-2407-12-157.
- Vano E, Kleiman NJ, Duran A, Romano-Miller M, Rehani MM. Radiation-associated lens opacities in catheterization personnel: results of a survey and direct assessments. J Vasc Interv Radiol. 2013 Feb; 24(2): 197-204. doi: 10.1016/j.jvir.2012.10.016.
- Ron E, Brenner A. Non-malignant thyroid diseases after a wide range of radiation exposures. Radiat Res. 2010 Dec; 174(6): 877-888. doi: 10.1667/RR1953.1.
- Roguin A, Goldstein J, Bar O, Goldstein JA. Brain and neck tumors among physicians performing interventional procedures. Am J Cardiol. 2013 May 1; 111(9): 1368-1372. doi: 10.1016/j.amjcard.2012.12.060.
- Burdorf A, Figà-Talamanca I, Jensen TK, Thulstrup AM. Effects of occupational exposure on the reproductive system: core evidence and practical implications. Occup Med (Lond). 2006 Dec; 56(8): 516-520.
- Dehmer GJ. Occupational hazards for interventional cardiologists. Catheter Cardiovasc Interv. 2006 Dec; 68(6): 974-976.
- Weisz G, Metzger DC, Caputo RP, Delgado JA, Marshall JJ, Vetrovec GW, et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (Percutaneous Robotically-Enhanced Coronary Intervention) Study. J Am Coll Cardiol. 2013 Apr 16; 61(15): 1596-1600. doi: 10.1016/j.jacc.2012.12.045.
Disclosure: Dr. Wohns and Dr. Madder report no conflicts of interest regarding the content herein.
The authors can be contacted via David.Wohns@spectrumhealth.org.
