


Pre-CLI: The Transformative Space Between PAD and CLI
Disclosure: Dr. Mustapha reports he is a consultant for Bard, Covidien, Cordis, CSI, Spectranetics, Boston Scientific, Cook, and Terumo.
Dr. J.A. Mustapha can be contacted at jihad.mustapha@metrogr.org.
For years, we have accepted critical limb ischemia (CLI) as an end result of peripheral arterial disease (PAD). Recently, we have noticed an influx of patients transforming from PAD into CLI over the course of years. One should stop and think about the course of transformation from PAD to CLI, and if there is any indication that these transformations occur during a time when the patient is no longer a claudicant, but not yet technically diagnosed as CLI. What do we call such patients? The most realistic  description, in my opinion, is pre-CLI.
description, in my opinion, is pre-CLI.
Figure 1 is an example of a patient referred to as advanced Rutherford 3 claudication, occasionally referred to as Rutherford 3a-b. But the same patient shows an anatomical obstruction in the arterial supply of the lower extremity consistent with CLI anatomical distribution. However, this patient presented with symptoms consistent with claudication. Historically, we differentiated these patients by performing additional hemodynamic assessments such as toe brachial index (TBI), toe pressures, ankle pressures, etc. This specific patient presents with claudication with anatomical variations consistent with CLI and a hemodynamic assessment consistent with CLI. We are now faced with a therapeutic options dilemma between high-risk revascularization of either a tibial vascular bypass surgical repair or high-risk endovascular revascularization. At this point in time, there is no trial data to answer the question of why and how these patients should be treated. It has been observed, in the arena of CLI therapists, that the provision of early therapy to patients with this type of anatomy may prevent or delay the presentation of CLI. As we well know once CLI presents, especially advanced CLI of Rutherford stages 5 and 6, there is a high association with comorbidities and mortality.
Therefore, these patients with strong evidence of CLI by means of anatomy and hemodynamic measurements, but not strong evidence of clinical presentation in terms of symptoms, fall into the category between advanced claudication and technical CLI. It is 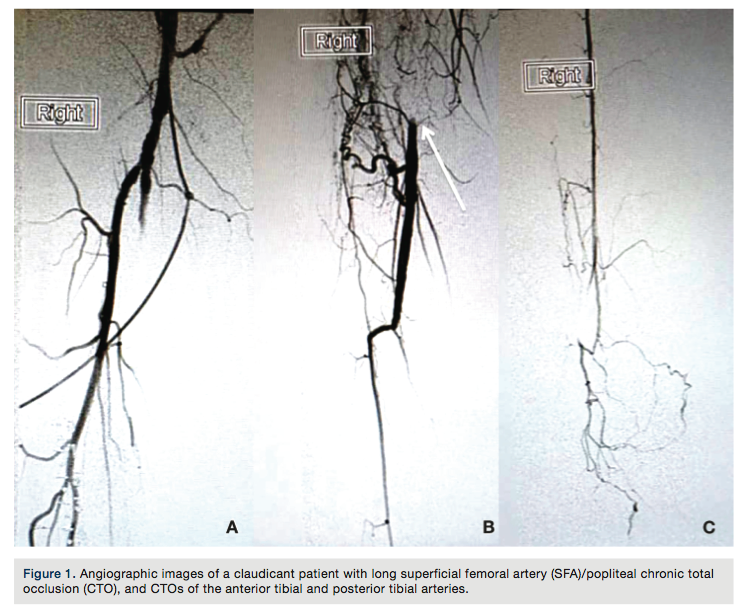 fair to say that this patient should be referred to as pre-CLI based on the fact they already have significant indications of CLI based on the anatomy and hemodynamic measurements.
fair to say that this patient should be referred to as pre-CLI based on the fact they already have significant indications of CLI based on the anatomy and hemodynamic measurements.
Of course the issue of what should be done with such patients remains controversial. Also, as mentioned above, the lack of data continues to be a major barrier as well. But such patients are becoming more common than ever, as there is far more awareness of the seriousness and implication of CLI, and because more research is being done on such patients. Now that we are able to identify these patients, it is my opinion that they should be revascularized if they meet one of the following criteria:
- The patient presents as pre-CLI with symptoms of advanced PAD and anatomical disease consistent with CLI anatomy, such as advanced tibial disease.
- The patient presents with hemodynamic indications consistent with CLI disease.
The revascularization choice between endovascular intervention or vascular bypass should be determined based on the best option for the anatomy we are faced with.
In Figure 2, far more advanced anatomical disease can be seen, speaking volumes to the fact that a CLI diagnosis cannot be made by observation and physical assessment alone. This patient, at this point, has no feeling in the lower extremities, including the feet. Therefore, this patient does not complain of any rest pain and is active. The question here is, what do we do with this type of patient? Again, this is a controversial issue, but a reality we face every day. Theoretically, we can extrapolate that some of these patients don’t have feeling secondary to diabetic neuropathy. Additionally, ischemic neuropathy caused by advanced and chronic lack of blood supply to the lower extremities may lead to some of these patients losing feeling in their feet.
Interestingly, not all of these patients will have a hemodynamic abnormality consistent with CLI, which could be due to multiple underlying causes. The most common is calcification of the tibial pedal vessels, which tend to cause elevated ankle-brachial indexes and other hemodynamic measurements such as TBIs.
Again, this leaves us with yet another major dilemma: patients with no active rest pain or claudication found to have angiographically determined advanced disease, as shown in Figure 3. What do we do with such patients? There is a significant split in opinion between operators on how such patients should be treated. Some would say leave it alone and observe until there is progression of symptoms. Some would say medical therapy alone is sufficient. Some would say definitely revascularization of some sort. My personal opinion has been to evaluate and assess each patient individually. In my practice, I have seen many such patients present with this type of anatomy; we have observed them over time and they tend to do well. However, with the sudden occurrence of any acute change, such as any trauma leading to skin breakdown or additional loss of a collateral for any reason (embolization, plaque rupture or acute thrombosis of a collateral), we see presentation of another devastating event: the cold foot. Development of 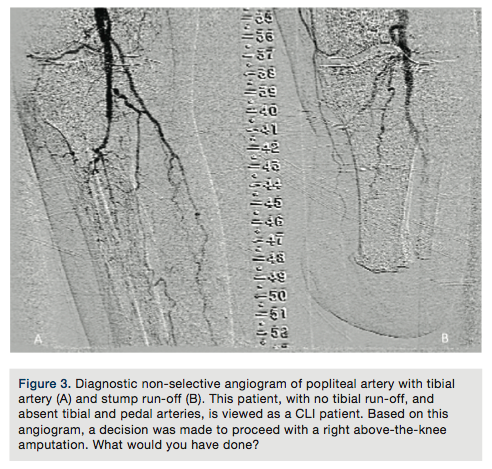 a cold foot quickly puts these patients in the critical category of acute CLI with high likelihood for need of amputation. This prevents an ethical dilemma. Should we have treated such patients earlier when they were stable, with no apparent urgency, and created some revascularization to the foot, leaving a backup system for the future? Would this have made a difference in patient outcome? Observational theory would say yes, but medicine requires data. We don’t yet have this data available to us now, at the time we need to make critical decisions for the best patient outcome.
a cold foot quickly puts these patients in the critical category of acute CLI with high likelihood for need of amputation. This prevents an ethical dilemma. Should we have treated such patients earlier when they were stable, with no apparent urgency, and created some revascularization to the foot, leaving a backup system for the future? Would this have made a difference in patient outcome? Observational theory would say yes, but medicine requires data. We don’t yet have this data available to us now, at the time we need to make critical decisions for the best patient outcome.
In my opinion and in my current practice, I tend to look at these pre-CLI patients with the same binocular vision I use for CLI patients. Once the anatomical variation of CLI is present and any hemodynamic abnormality of CLI is present, regardless of the initial presentation, I believe these patients should have some form of revascularization. They should potentially be treated early and with the same aggressiveness with which we treat CLI patients today. Although we don’t have clinical trials to support my opinion at this time, I am hopeful we will in the near future. In the meantime, pre-CLI is a serious stage of advanced PAD and should be addressed as an urgent matter.
