


Patient Safety in the Cath Lab: A Team Sport Part II of III
 A patient with stable angina undergoes fractional flow reserve assessment in the cath lab for an intermediate left anterior descending coronary artery stenosis. The physician verbally orders heparin to be given and proceeds with placing a pressure wire. After several minutes, the patient develops chest pain, and the artery is found to have multiple areas of thrombosis, requiring thrombus aspiration and multiple long stents. An activated clotting time (ACT) is checked and is found to be <150 seconds. The (new) nurse is asked about the heparin, and said she never heard the order to administer it.
A patient with stable angina undergoes fractional flow reserve assessment in the cath lab for an intermediate left anterior descending coronary artery stenosis. The physician verbally orders heparin to be given and proceeds with placing a pressure wire. After several minutes, the patient develops chest pain, and the artery is found to have multiple areas of thrombosis, requiring thrombus aspiration and multiple long stents. An activated clotting time (ACT) is checked and is found to be <150 seconds. The (new) nurse is asked about the heparin, and said she never heard the order to administer it.
Who is at fault for this complication? Was it the nurse who never heard the order? Was it the physician who placed an intracoronary wire without confirmation the heparin was given, or that the ACT was therapeutic? Both? Neither?
The effective team
 Healthcare is, like most complex human activities, a team sport. There are many aspects to effective teams including a common purpose, mutual respect, effective leadership and conflict resolution, good communication, situational awareness, and flexibility. Ineffective teams are marked by strict hierarchies, fear of communicating concerns, and a lack of familiarity with team members and their roles. In some cath labs, the physician is king and sometimes acts accordingly — these may be some of the most dangerous labs to be in, as the staff may not feel at liberty to discuss their concerns. Creating a good communication environment in the cath lab therefore includes: a) effective communications procedures, b) a climate of respect where everyone can communicate their concerns, and c) effective management that encourages rather than discourages the reporting of potential safety issues.
Healthcare is, like most complex human activities, a team sport. There are many aspects to effective teams including a common purpose, mutual respect, effective leadership and conflict resolution, good communication, situational awareness, and flexibility. Ineffective teams are marked by strict hierarchies, fear of communicating concerns, and a lack of familiarity with team members and their roles. In some cath labs, the physician is king and sometimes acts accordingly — these may be some of the most dangerous labs to be in, as the staff may not feel at liberty to discuss their concerns. Creating a good communication environment in the cath lab therefore includes: a) effective communications procedures, b) a climate of respect where everyone can communicate their concerns, and c) effective management that encourages rather than discourages the reporting of potential safety issues.
 In the above example, rather than blaming the nurse for not hearing the order, or the physician for not confirming that the drug had been given before proceeding with wiring the vessel, experts in systems analysis would tell us that “to err is human” and that it was this lab’s system of communication that needs correction. As in the old game of “telephone”, where the message is distorted with each handoff, in the absence of structured and systematic communication procedures, miscommunications in a team will be frequent and lead to potentially disastrous consequences. Communications in the lab should be in the style of combat pilots with the “right stuff”: cool, clear and brief.
In the above example, rather than blaming the nurse for not hearing the order, or the physician for not confirming that the drug had been given before proceeding with wiring the vessel, experts in systems analysis would tell us that “to err is human” and that it was this lab’s system of communication that needs correction. As in the old game of “telephone”, where the message is distorted with each handoff, in the absence of structured and systematic communication procedures, miscommunications in a team will be frequent and lead to potentially disastrous consequences. Communications in the lab should be in the style of combat pilots with the “right stuff”: cool, clear and brief.
Effective communication
The U.S. Agency for Healthcare Research and Quality (AHRQ) has collected and developed several techniques that lead to clear, effective communication:
- SBAR (Situation – Background – Assessment – Recommendation). This is a systematic method of presenting information that organizes what might be a complex situation into an easily understandable summary. For instance, if you are a nurse calling a physician about a patient that you are worried about, you might say: a) I am calling about patient “X” who is having hypotension and flank pain; b) he just came out from a femoral cath two hours ago; c) I think he is having a retroperitoneal bleed; and d) I think you need to come here right away to assess him!
- Call-out. If it is not already clear who should be doing something, the physician needs to “call out” the person they are talking to by name, rather than just announcing to the air what he wants to have happen. For example, “Sally, please give X”. This is most critical in code situations when lots of new and unfamiliar personnel come into the cath lab.
- Check-back – “close the circle” of communication. When an order is verbally made, the listener should a) confirm that the order was heard, and b) announce when the order has been completed and the drug given. The operator should not assume that his order was heard, and should ask if he/she did not hear a check-back. Check-backs are especially important with verbal orders in the cath lab, such as ones for heparin in the above example.
- Handover/handoff. When one technologist or nurse relieves another of duty in the cath lab, it is imperative that the departing staff passes along information about the drugs that have been given, the duration or phase of the procedure, and what has been tried already.
- Briefings and debriefings. Before any new, unusual, or complex procedure is attempted, the team should meet and review the case plan, any equipment that is needed, and any precautions that need to be taken. Conduct brief, open meetings of the cath lab promptly after complex procedures are completed or when complications occur. Discuss what went right during the procedure and what could be improved upon. Most importantly, debriefings allow the staff to have the opportunity to safely speak out about their concerns in an environment where it will not distract from patient care.
Stop the line!
 When there is a safety issue, or a potential disagreement or conflict arises, it is critical that every member of the cath lab staff be encouraged to bring up their concerns. On the door of our VA cath lab is a sign from our central office that reads “Stop the Line” (Figure 1). Originally from assembly lines, the saying empowers anyone from the janitor to the nurse to the physician to speak up if they spot a potential patient safety issue, whether it is a puddle on the floor, a broken ventilator, or a break in sterility. While the operating physician, cath lab manager, or hospital nursing supervisor ultimately makes the decision about whether a safety issue exists, front-line personnel should make their concerns heard. The AHRQ recommends the following strategies for effectively communicating safety concerns:
When there is a safety issue, or a potential disagreement or conflict arises, it is critical that every member of the cath lab staff be encouraged to bring up their concerns. On the door of our VA cath lab is a sign from our central office that reads “Stop the Line” (Figure 1). Originally from assembly lines, the saying empowers anyone from the janitor to the nurse to the physician to speak up if they spot a potential patient safety issue, whether it is a puddle on the floor, a broken ventilator, or a break in sterility. While the operating physician, cath lab manager, or hospital nursing supervisor ultimately makes the decision about whether a safety issue exists, front-line personnel should make their concerns heard. The AHRQ recommends the following strategies for effectively communicating safety concerns:
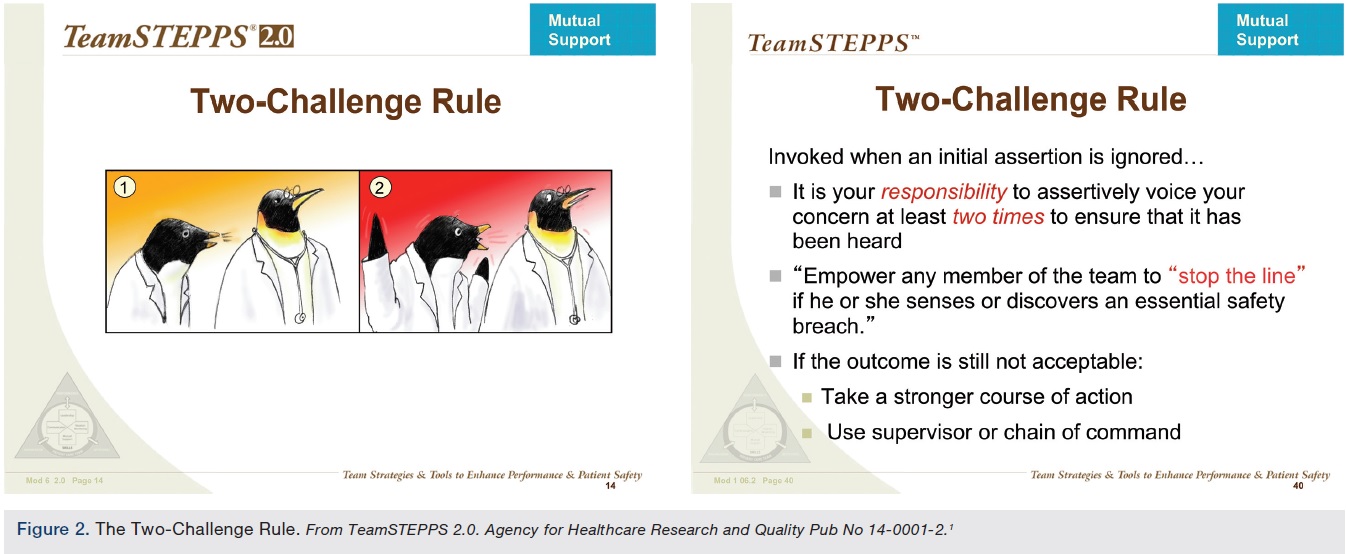
- Use the “two-challenge” rule. If any member of the team has a concern, it is their responsibility to communicate this to the operator, not just once, but at least twice (Figure 2). The operator must acknowledge the concern, and explain the rationale behind their decision. If the outcome is still unacceptable, you should consider taking a stronger course of action, or use the supervisory chain of command.
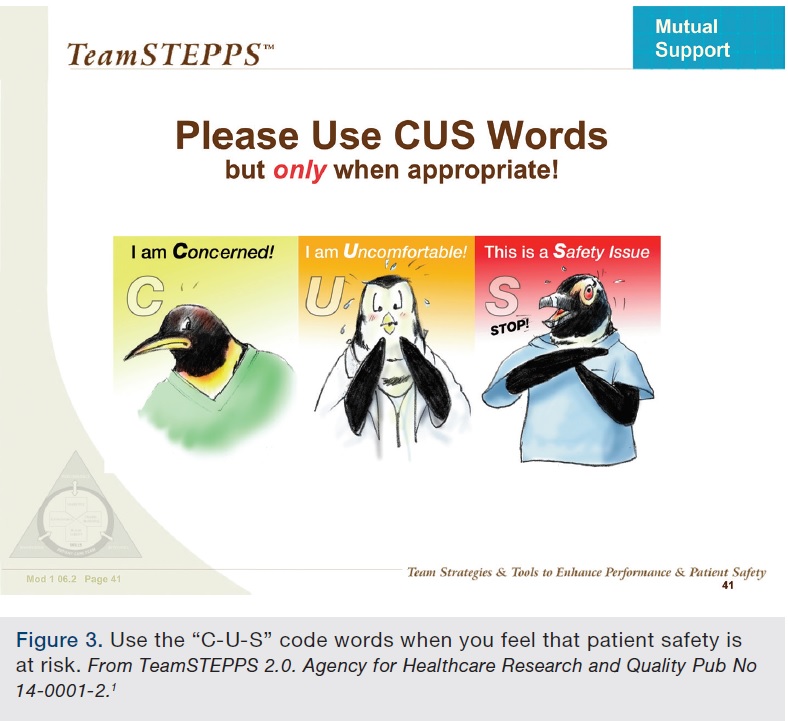
- Use the “C-U-S” code words when you feel that patient safety is at risk. Say either “I am Concerned”, or “I am Uncomfortable”, or “This is a Safety issue” (Figure 3). Code words should be treated seriously by the physician, and addressed.
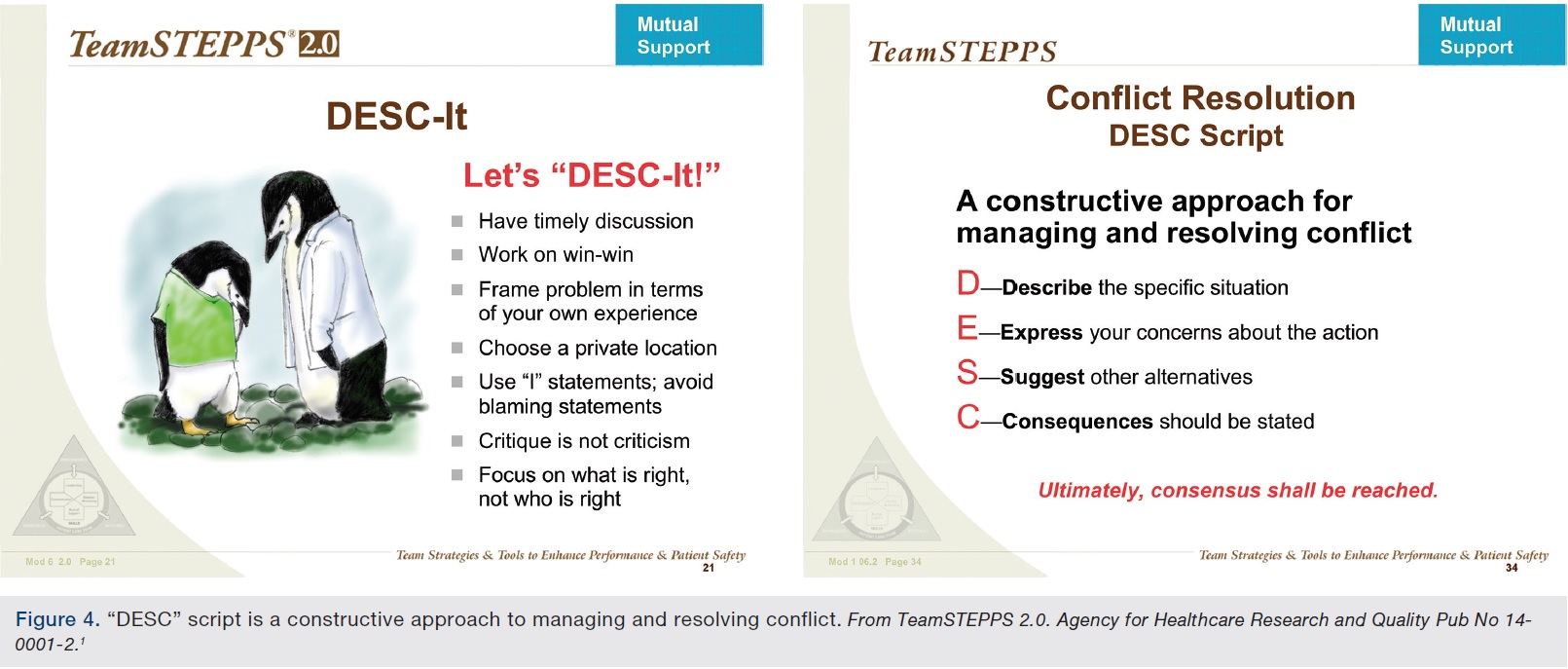
- Use “DESC” script (Describe, Express, Suggest, Consequences), a constructive approach to managing and resolving conflict (Figure 4). Describe the specific situation or behavior, and provide concrete data. Express how the situation makes you feel and what your concerns are. Suggest other alternatives and seek agreement. Consequences should be stated in terms of impact on the patient or team.
 Code words and safety challenges should naturally be used only as appropriate, and escalated in proportion to the safety risk. If an operator asks for a 3.0 mm balloon for a 3.0 mm vessel, no one should question that order. If the operator asked for a 4.5 mm balloon for the same vessel, one might express a little concern, and double check (twice) that the operator was sure of what he was asking for, and explaining that the balloon might cause a dissection. If the operator asked for a 20 mm valvuloplasty balloon for a coronary artery, and was visibly intoxicated, you should refuse that order entirely, remove the patient from the care of an impaired physician, and report the physician to the hospital administration or state medical board.
Code words and safety challenges should naturally be used only as appropriate, and escalated in proportion to the safety risk. If an operator asks for a 3.0 mm balloon for a 3.0 mm vessel, no one should question that order. If the operator asked for a 4.5 mm balloon for the same vessel, one might express a little concern, and double check (twice) that the operator was sure of what he was asking for, and explaining that the balloon might cause a dissection. If the operator asked for a 20 mm valvuloplasty balloon for a coronary artery, and was visibly intoxicated, you should refuse that order entirely, remove the patient from the care of an impaired physician, and report the physician to the hospital administration or state medical board.
A case study in miscommunication in the aviation industry occurred on Tenerife in the Canary Islands in 1977. Large aircraft were diverted to a small regional airport after a terrorist threat at the main international airport. Fog and crowded conditions on the tarmac led to planes crossing multiple active runways. The pilot of one 747, frustrated by delays, started the takeoff procedure (advancing the throttle) without getting clearance by the air traffic controller. His copilot stopped him by advising that clearance had not yet been given, and the pilot backed down and waited as suggested. The tower then gave instructions on the flight path after takeoff, and used the word “takeoff”, but did not say they were clear to go. The copilot read back that “We are now at takeoff”, interrupted by the pilot saying “We’re going”. The tower initially said “Ok”, which was nonstandard terminology, but quickly added “Stand by for takeoff, I will call you”. Unfortunately, the latter part of the message was lost by interference from another radio call on the same frequency. The copilot failed to challenge the pilot a second time, and the plane proceeded to take off, hitting a second 747 on the ground, and killing a combined 583 people on both planes in what remains the worst aviation disaster in history. In this case, unclear communication terminology, failure to close the circle of (confusing) communication, and failure to challenge authority a second time led to deadliest aviation disaster in history.
We have a lot to learn about effective team communication from other industries such as aviation and the military. Try these communication techniques in your cath lab the next time you see a potential safety issue.
If you have a question or case example that you would like to share, please contact me by email at arnold.seto@va.gov.
Reference
- TeamSTEPPS 2.0. Agency for Healthcare Research and Quality Pub No 14-0001-2. Available at: https://www.ahrq.govhttps://s3.amazonaws.com/HMP/hmp_ln/imported/wysiwyg/professionals/education/curriculum-tools/teamstepps/instructor/essentials/pocketguide.pdf.
Q &A WITH DR. SETO
Safety Q&A
If you have a question or case example that you would like to share, please contact Dr. Arnold Seto by email at arnold.seto@va.gov.
Question
From a CLD reader
“How do you address safety issues with physicians that regularly rush STEMI [ST-elevation myocardial infarction] patients to the cath lab when the entire 3-person team has not yet arrived? The physician wants to help the patient quickly, but the staff has 30 minutes to respond; having the patient transferred to the cath lab without the staff ready compromises the care received by the patient. What would help the physician understand that we too want to help the patient, but safety is priority?”
Answer
Arnold Seto, MD, MPA, Chief, Cardiology, Long Beach VA Medical Center, Long Beach, California
This is a common and challenging situation that the reader poses. On the one hand, rapid revascularization is a goal and a quality measure for the hospital. As we have been reminded repeatedly, “time is muscle” and all efforts should be made to minimize the door-to-balloon (D2B) time. On the other hand, bringing a critically ill acute STEMI patient to the cardiac cath lab when insufficient staff is present to handle potential complications (cardiac arrest, shock) can be a serious safety issue. STEMI patients have about 5% mortality, and need all hands on deck when things go wrong (as they quickly and easily could). The physician has a responsibility to exercise good judgment for the safety of the patient, rather than try and break records on the D2B time.
The communication techniques described in the attached article would be helpful in helping the physician understand the safety concerns of the staff. Using the code words “I am concerned”, or “I am uncomfortable” about bringing a patient to the lab should help them understand that you have serious safety concerns about the situation. Describe the potential consequences of inadequate staffing: “What if the patient codes when only one team member is alone with the patient?” and “As soon as the patient is out of the ER, they are no longer going to take responsibility for the patient if he arrests (and it would be on your/our heads)”.
Educate the physician on the things that the staff who arrive early will be doing to expedite the procedure once everyone is present, including entering the patient information into the system, preparing the table if not already done so, calling for a bed, and taking report. Bringing a patient in when these tasks are incomplete can potentially slow down a procedure even while incurring a risk to the lab. Finally, data from the NCDR CathPCI registry1 suggests that reductions in D2B time have not been met with reductions in mortality, suggesting that pre hospital delays to care may be more important than a few (i.e., 10) minutes of waiting the full team to arrive.
Working in a collaborative fashion with the physician may open up alternatives that address everyone’s concerns. For example, if only 2 out of 3 team members are present, one could request that the ER nurse transporting the patient stay in the lab and assist with moving the patient, monitoring, or moderate sedation until the last staff member arrives. If a fellow or attending physician is already present and willing to serve, they could be counted as part of the team, so long as they are willing to help move the patient, set up/pan the table, and do chest compressions if needed.
Ultimately, however, your facility has established as its standard of care a 3-member cath lab team. It would take only one sentinel event during the period of inadequate staffing to force a policy change. (Imagine what hay a plaintiff’s attorney could make out of a death that occurred while the cath lab was short staffed!) The majority of cath labs have a standard operating procedure, policy, or at least an unwritten rule that the patient is brought up only when the entire team is present (or 2-3 out of 4, or 2 out of 3, always including at least one nurse). Otherwise, the decision is usually on the discretion of the accepting nurse based on the acuity of the patient and the estimated arrival time of the remaining team members.
The physician is only part of the team that helps shape the policy of the cath lab and hospital. A physician cannot demand an ICU nurse take more than 2 patients, or that a patient in shock with a balloon pump be transferred to a step down unit, because there are established policies and safety procedures that preclude it. If the flexibility of using discretion in the cath lab is failing, the cath lab team, manager, and physicians should together decide what the policy should be, so that everyone is comfortable with it moving forward.
Reference
- Menees DS, Peterson ED, Wang Y, Curtis JP, Messenger JC, Rumsfeld JS, Gurm HS. Door-to-balloon time and mortality among patients undergoing primary PCI. N Engl J Med. 2013 Sep 5; 369(10): 901-909.
