


Old But Forgotten Art of Palliative Therapy for Recurrent Malignant Pericardial Effusion by Percutaneous Balloon Pericardiotomy
Recurrent pericardial effusions are commonly associated with pericardial metastasis of malignant extra cardiac organs. The therapeutic options for the treatment include the instillation of sclerosing substances or chemotherapeutic agents in the pericardium, which are associated with high recurrence rates and patient discomfort.1 Another option is surgery to create a pericardial window; however, this technique has the drawback of requiring general anesthesia. Similar disadvantage is found in the case of thoracotomy to open a pleuropericardial window or pericardiectomy. This increases the mortality risk in an already critically ill patient. Percutaneous balloon pericardiotomy offers an alternative in these patients. In 1975, Flannery et al demonstrated that malignant pericardial effusions can be treated successfully in poor surgical candidates using an indwelling pericardial catheter.2 The technique has evolved through the years since and now includes balloon pericardiotomy in its present form.3 This case will discuss this underutilized technique and offer an alternative to be considered in critically ill patients.
Case Presentation
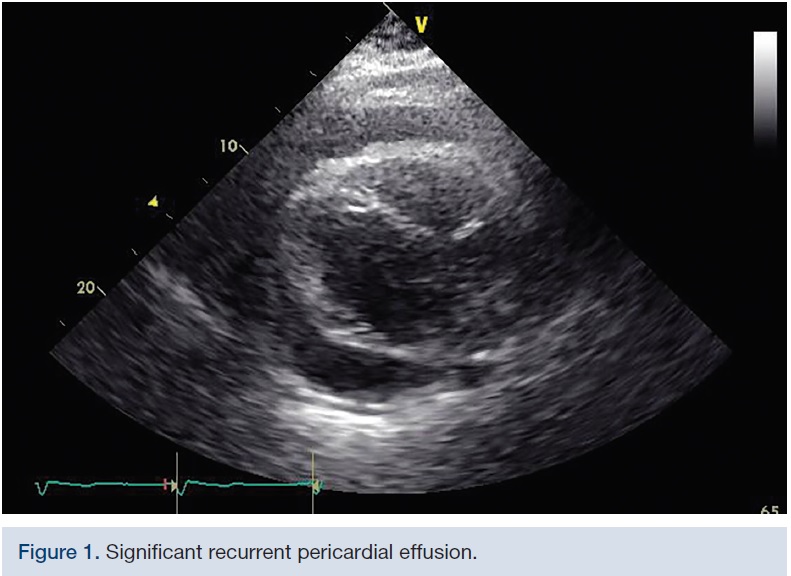 A 39-year-old female with past medical history of recurrent malignant pericardial effusions secondary to stage IV metastatic breast cancer, status post pericardial window placement two months prior, presented to hospital with complaints of worsening dyspnea. Transthoracic echocardiogram showed significant re-accumulation of pericardial fluid that was thought to be contributing to her symptoms (Figure 1). After pericardiocentesis with 800 ml of blood-tinged pericardial fluid, she came back to hospital with similar complaints in two weeks and repeat echocardiogram demonstrated significant pericardial fluid re-accumulation with tamponade physiology, at which point, palliative percutaneous balloon pericardiotomy was performed.
A 39-year-old female with past medical history of recurrent malignant pericardial effusions secondary to stage IV metastatic breast cancer, status post pericardial window placement two months prior, presented to hospital with complaints of worsening dyspnea. Transthoracic echocardiogram showed significant re-accumulation of pericardial fluid that was thought to be contributing to her symptoms (Figure 1). After pericardiocentesis with 800 ml of blood-tinged pericardial fluid, she came back to hospital with similar complaints in two weeks and repeat echocardiogram demonstrated significant pericardial fluid re-accumulation with tamponade physiology, at which point, palliative percutaneous balloon pericardiotomy was performed.
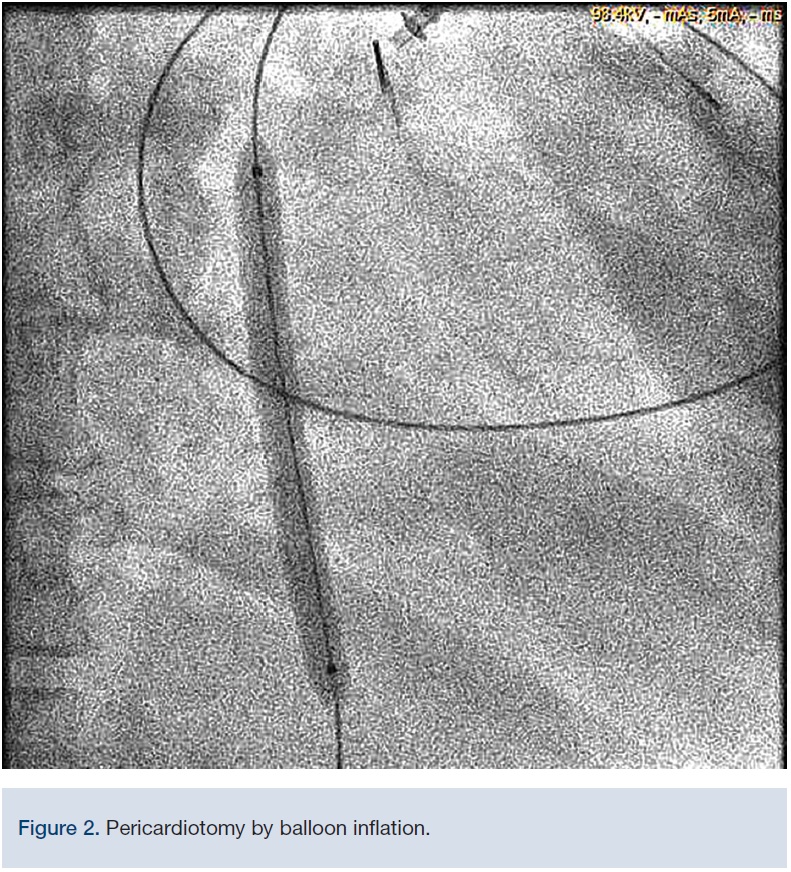 Procedure: A spinal needle was introduced under the xiphoid process, and directed posteriorly toward the tip of the left scapula until the pericardial space was entered and fluid aspirated. Bloody pericardial fluid was aspirated. Echo was used to confirm positioning. A long exchange wire was introduced via fluoroscopy and was shown to loop around the heart, confirming location in the pericardial space. A fenestrated pigtail catheter was introduced into the pericardial space over a guidewire and fluid collection was started, using the provided 50 ml syringe. After draining fluid, we exchanged the pigtail catheter for an over-the-wire 5.0 x 40 mm Admiral Xtreme balloon (Medtronic) to perform pericardectomy, followed by a 7.0 x 80 mm Admiral Xtreme balloon (Figure 2) without any complications. A post-procedure echo was performed with substantial reduction in pericardial fluid. Approximately 900 mL of blood-tinged pericardial fluid was aspirated into a collecting bag.
Procedure: A spinal needle was introduced under the xiphoid process, and directed posteriorly toward the tip of the left scapula until the pericardial space was entered and fluid aspirated. Bloody pericardial fluid was aspirated. Echo was used to confirm positioning. A long exchange wire was introduced via fluoroscopy and was shown to loop around the heart, confirming location in the pericardial space. A fenestrated pigtail catheter was introduced into the pericardial space over a guidewire and fluid collection was started, using the provided 50 ml syringe. After draining fluid, we exchanged the pigtail catheter for an over-the-wire 5.0 x 40 mm Admiral Xtreme balloon (Medtronic) to perform pericardectomy, followed by a 7.0 x 80 mm Admiral Xtreme balloon (Figure 2) without any complications. A post-procedure echo was performed with substantial reduction in pericardial fluid. Approximately 900 mL of blood-tinged pericardial fluid was aspirated into a collecting bag.
Discussion
Percutaneous balloon pericardiotomy offers an alternative in critically ill patients. It can be viewed as a percutaneous variant of the subxiphoid approach to creating a surgical window; however, it is less invasive and less traumatic. This case illustrates that it can be a simple procedure that can be performed in seriously ill patients (cardiac tamponade) with a low rate of complications and little discomfort. There are several therapeutic approaches available for large pericardial effusions. In the emergency setting, pericardiocentesis is often chosen; however, it often does not result in complete fluid evacuation and also is associated with high re-accumulation rates.4,5,6 More definitive management can be achieved via surgery by creating a pericardial window to allow continuous drainage and reduce the re-accumulation rates.7 However, some patients are poor surgical candidates and would likely not survive the creation of a surgical pericardial window.
The complications are similar to those of pericardiocentesis in general. The pericardial puncture is with little risk for cardiac perforation due to the abundance of fluid. The likely mechanism of pericardial drainage is that the fluid does not accumulate because it drains into the pleural cavity.
Conclusion
We found percutaneous balloon pericardiotomy to be a simple and safe procedure. It allows recurrent pericardial effusion to be treated successfully with less complications. This procedure can be considered as an alternative option for palliative therapy in critically ill patients or those at high surgical risk. The long-term prognosis of these patients depends mainly on their underlying disease.
References
- Puri A, Agarwal N, Dwivedi SK, et al. Percutaneous balloon pericardiotomy for the treatment of recurrent malignant pericardial effusion. Indian Heart J. 2012 Jan-Feb; 64(1): 88-89.
- Flannery EP, Gregoranos G, Corder MP. Pericardial effusion in patients with malignant diseases. Arch Intern Med. 1975: 135: 976-977.
- Galli M, Politi A, Pedretti F, et al. Percutaneous balloon pericardiotomy for malignant pericardial tamponade. Chest. 1995; 108(6): 1499-1501.
- Laham RJ, Cohen DJ, Kuntz RE, et al. Pericardial effusion in patients with cancer: outcome with contemporary management strategies. Heart. 1996; 75(1): 67-71.
- Fiocco M, Krasna MJ. The management of malignant pleural and pericardial effusions. Hematol Oncol Clin North Am. 1997; 11(2): 253-265.
- Chen EP, Miller JI. Modern approaches and use of surgical treatment for pericardial disease. Curr Cardiol Rep. 2002; 4(1): 41-46.
- Liberman M, Labos C, Sampalis JS, et al. Ten-year surgical experience with non traumatic pericardial effusions: a comparison between the subxyphoid and transthoracic approaches to pericardial window. Arch Surg. 2005; 140(2): 191-195.
Disclosures: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Neelima Katukuri, MD at nkatukuri@utmck.edu
