


New Setup for Dual Injection for Chronic Total Occlusion Percutaneous Coronary Interventions Using a Single Automated Contrast Injector System
This article received a double-blind review from members of the Cath Lab Digest Editorial Board.
Disclosure: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Naveen Rajpurohit, MD, at lakshya.naveen@gmail.com.
Introduction
Dual injections are crucial for performing chronic total occlusion (CTO) percutaneous coronary interventions (PCI). They help in optimal visualization of the proximal and distal caps, distal vessel beyond the CTO, and collaterals. With dual injection, as the collateral bed fills with contrast, the non-contrast containing competitive flow is reduced and this provides adequate visualization of the CTO vessel. It provides critical information regarding the lesion length, size, and location of distal target vessel and helps decide the optimal strategy for CTO PCI. It can help decide if a retrograde approach is feasible. Thus, it is often the first step in determining the feasibility of a CTO PCI.1 During CTO PCI, it plays a crucial role in clarifying the position of the guide wire and other equipment. Currently, there is no standard setup for dual injection during CTO PCIs using an automated contrast injector system (ACIST CVi, ACIST Medical).
Over the last decade, ACIST has been promoted as a strategy to reduce the amount of contrast use and improve outcomes during diagnostic and interventional procedures.2,3 ACIST use would be helpful in CTO PCI as it provides better control over the rate, amount, and rate of rise of contrast. In addition, it can prevent hydraulic enlargement of the sub-intimal space during dissection/re-entry techniques and increase chances of successful re-entry. Currently, manual injectors are used in addition to ACIST for dual injection during CTO PCIs. We introduce a novel setup for dual injection with the help of one ACIST.
Setup
A four-way central stopcock (Marquis stopcock 1050 psi) connects contrast tubing to the ACIST at one end and to the catheter at access site 1 at the other end, using 12-inch arterial pressure tubing (Figure 1A). The middle port of the four-way stopcock is connected to one of the side ports of a three-way stopcock at access site 2 using a tubing connector with similar ends (Figures 1B and 1C). We used the injection line tubing (54-inch) available in the ACIST AngioTouch Kit for this purpose, as this is the only readily available long tubing available in our catheterization laboratory that has similar receiving connections on its ends (i.e., the connection on the four-way stopcock and the stopcock at the second catheter are 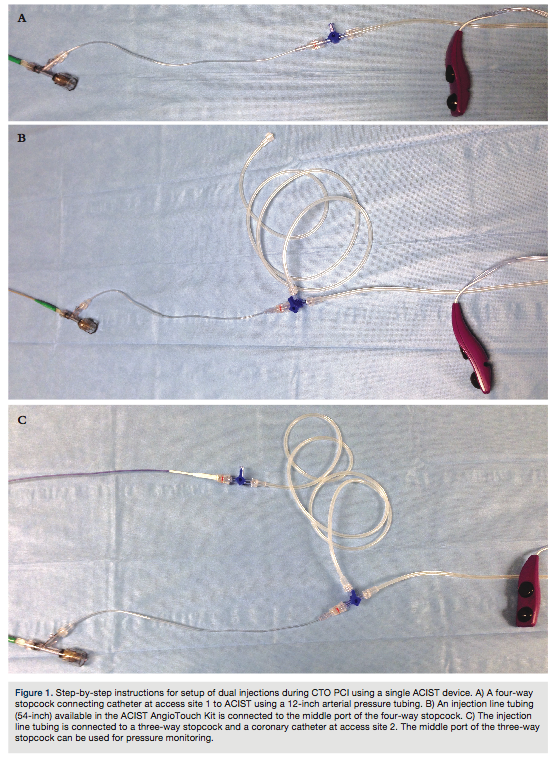 similar and not complementary). However, if a shorter tube is available (such as the 12-inch arterial pressure tubing used between the first catheter and four-way stopcock with “similar” receiving ends), that could be used to connect the 4-way stopcock and the second catheter.
similar and not complementary). However, if a shorter tube is available (such as the 12-inch arterial pressure tubing used between the first catheter and four-way stopcock with “similar” receiving ends), that could be used to connect the 4-way stopcock and the second catheter.
The three-way stopcock is connected to the catheter at access site 2 at one of its ends and to the four-way stopcock at its other end using a tubing connector as mentioned above (Figure 1C). The middle port of the three-way stopcock is connected to a pressure transducer using a connector tube for pressure monitoring through the catheter at access site 2. The pressure through catheter at access site 1 is measured through the ACIST system.
Injection
For dual injection: Appropriate settings for injection are dialed into the ACIST injector system. The pressure waves at both the catheters are confirmed individually by turning the stopcocks appropriately. Once it is confirmed that the pressure waves look normal and there is no dampening, the central stopcock is turned down so that it is open to both the ports. The three-way stopcock at site 2 is turned off towards the pressure line so that it is open to flow into the catheter from the connector tube. The injection is performed (Figure 2).
For single-catheter injection though access site 1: Appropriate settings for injection are dialed into the ACIST injector system. The central four-way stopcock is turned off to the middle port (which connects to three-way stopcock). The stopcock at access site 2 is turned off to the connector tubing so that continuous pressure from the catheter can be monitored. Injection is performed. This would inject only the catheter at access site 1, while continuously monitoring the pressure at access site 2.
For single-catheter injection through access site 2: Appropriate settings for injection are dialed into the ACIST injector system. The four-way stopcock is turned off to the end connecting to the catheter at access site 1. The three-way stopcock at access site 2 is turned off to the pressure line. Injection is performed.
The total volume of contrast used for dual or single injections is displayed at the ACIST screen. During a dual injection, the volume of contrast injected and the pressure of injection from each catheter tip is not the same, as the length of the tubing from the four-way stopcock to each of the coronary catheters is different. However, the difference is insignificant. We attained images with adequate and timely visualization of both the coronary systems using dual injection with this technique 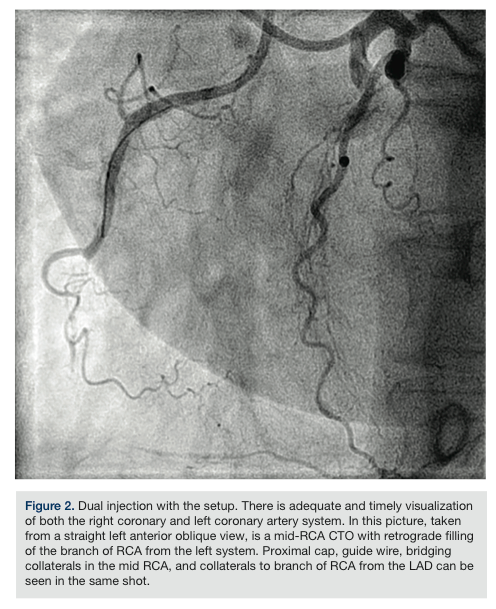 (Figure 2). There was no significant time lag between contrast injections from the ends of the catheters.
(Figure 2). There was no significant time lag between contrast injections from the ends of the catheters.
We introduce here a simple yet effective and safe method of using a single ACIST device for dual injections for CTOs using four-way stopcock and extra tubing. This simple technique saves time and extra equipment on the catheterization table during complex CTO procedures.
References
- Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012; 5(4): 367-379.
- Brosh D, Assali A, Vaknin-Assa H, et al. The ACIST power injection system reduces the amount of contrast media delivered to the patient, as well as fluoroscopy time, during diagnostic and interventional cardiac procedures. Int J Cardiovasc Intervent. 2005;7(4):183-187.
