


Case Report
Modified Crush via 6 French Radial Access

 Case Report
Case ReportA 77-year-old gentleman with a history of coronary artery disease status post previous stents to the left anterior descending coronary artery (LAD) and diagonal, and percutaneous transluminal coronary angioplasty (PTCA) in the past. He has diabetes and hypertension. He presented with chest pain after lifting some flower pots and experiencing shortness of breath. He subsequently ruled in for a non-ST elevation myocardial infarction, and was referred for diagnostic angiography and possible revascularization.
The right radial artery was prepped and draped in sterile fashion. The right radial artery was accessed with a Terumo Slender sheath. A Judkins left (JL) 3.5 was used to engage the left coronary system and Judkins right (JR)4 was used to engage the right coronary system and perform ventriculography.
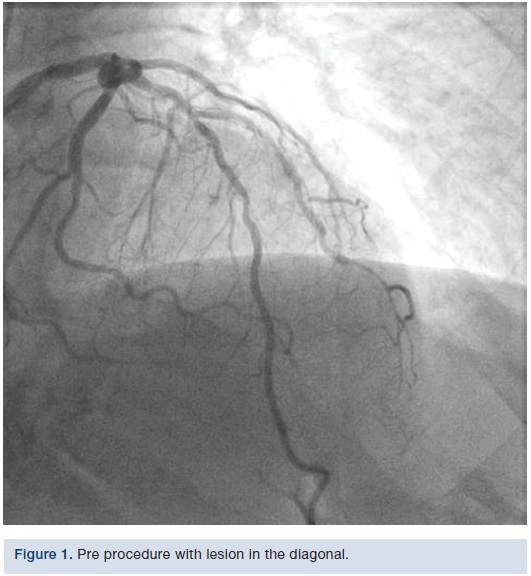
The LAD was patent in its proximal portion. The mid LAD gave rise to the diagonal (D)1, which had a stent going from the ostium to the mid portion. In some views, it appeared as though part of the struts could be in the LAD itself. The distal edge of the stent had a 95% to 99% restenosis and in-segment restenosis. Distally, the vessel was small and had a long 80% stenosis. The LAD itself had borderline 50% stenosis after the diagonal and then a patent stent. The remaining LAD appeared widely patent.
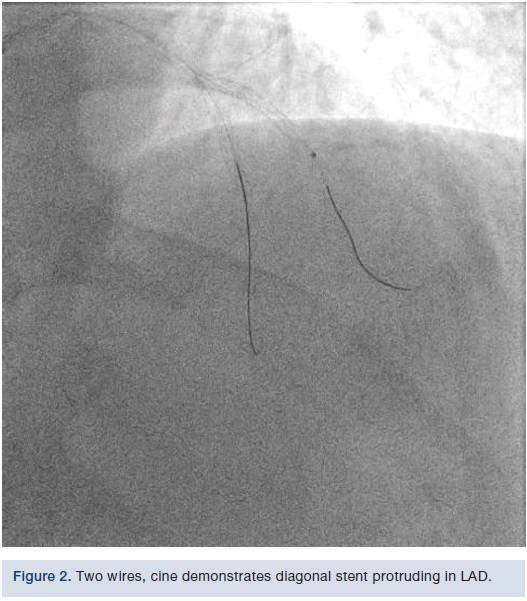
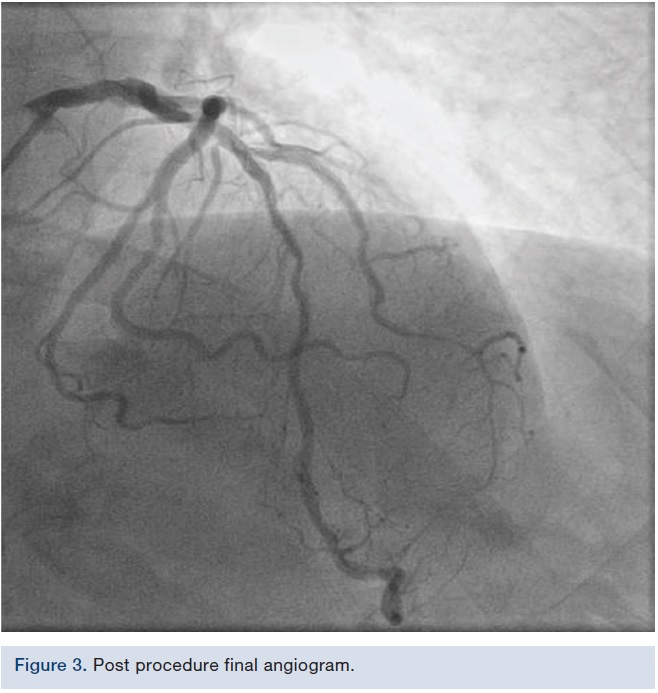
 We used a 6 French Extra Backup (EBU) 3.5 guide (Medtronic). We initially put a Runthrough wire (Terumo) down the diagonal and a Samurai wire (Boston Scientific) down the LAD. We then took a 0.9 laser after bivalirudin was administered and tried to cross into the diagonal; however, there was wire bias. The wire was pulled from the LAD into the diagonal, the laser was placed across the ostium, and then we rewired the LAD. Laser atherectomy was performed at a setting of 60/40, debulking the in-stent restenosis. We were then able to deliver a 2.5 x 10 mm AngioSculpt (Spectranetics), predilated, and placed a 2.5 x 24 mm Synergy drug-eluting stent (Boston Scientific) at 12 atmospheres. We post dilated with a 2.75 NC balloon (Medtronic), staying short of the ostium, because there was concern about where the stent was located. However, once we post dilated the stent, TIMI-3 flow was visible in both vessels. There was disease beyond the stent that was possibly wire spasm, but plaque shift in the LAD was visible as well, and on magnified views, it appeared that the struts might have been hanging out in the LAD, which would be why, when we manipulated the devices into the diagonal, some plaque shift took place in the LAD. There now appeared to be a 90% stenosis in the LAD focal right afterwards. Nitroglycerin was given and it did not resolve; therefore, we elected to go ahead and fix it. A Runthrough wire was put down the LAD and then a 2.75 x 12 mm noncompliant balloon that was used in the diagonal was dilated in the LAD. We crushed the ostium with the diagonal stent, and were then able to deliver a 3.0 x 16 mm stent going across the diagonal and overlapping with the previous LAD stent. The stent was deployed at 14 atmospheres. The LAD was rewired with the Runthrough wire and the Samurai wire pulled back. The diagonal was wired with the Samurai wire and now both wires were crossed. A 2.0 mm compliant balloon in the diagonal was dilated to 14 atmospheres, opening up the struts. A 3.0 x 12 mm noncompliant balloon was placed in the LAD and a 2.5 x 15 mm compliant balloon was placed in the diagonal. Nominal inflations were performed in both vessels, in a kissing manner. Final angiography revealed TIMI-3 flow without dissection, perforation, or embolization. The wires were removed. Orthogonal views were obtained, revealing TIMI-3 flow without dissection, perforation, or embolization. The patient tolerated the procedure well. The guide was removed and a TR Band (Terumo) was placed over the radial artery.
We used a 6 French Extra Backup (EBU) 3.5 guide (Medtronic). We initially put a Runthrough wire (Terumo) down the diagonal and a Samurai wire (Boston Scientific) down the LAD. We then took a 0.9 laser after bivalirudin was administered and tried to cross into the diagonal; however, there was wire bias. The wire was pulled from the LAD into the diagonal, the laser was placed across the ostium, and then we rewired the LAD. Laser atherectomy was performed at a setting of 60/40, debulking the in-stent restenosis. We were then able to deliver a 2.5 x 10 mm AngioSculpt (Spectranetics), predilated, and placed a 2.5 x 24 mm Synergy drug-eluting stent (Boston Scientific) at 12 atmospheres. We post dilated with a 2.75 NC balloon (Medtronic), staying short of the ostium, because there was concern about where the stent was located. However, once we post dilated the stent, TIMI-3 flow was visible in both vessels. There was disease beyond the stent that was possibly wire spasm, but plaque shift in the LAD was visible as well, and on magnified views, it appeared that the struts might have been hanging out in the LAD, which would be why, when we manipulated the devices into the diagonal, some plaque shift took place in the LAD. There now appeared to be a 90% stenosis in the LAD focal right afterwards. Nitroglycerin was given and it did not resolve; therefore, we elected to go ahead and fix it. A Runthrough wire was put down the LAD and then a 2.75 x 12 mm noncompliant balloon that was used in the diagonal was dilated in the LAD. We crushed the ostium with the diagonal stent, and were then able to deliver a 3.0 x 16 mm stent going across the diagonal and overlapping with the previous LAD stent. The stent was deployed at 14 atmospheres. The LAD was rewired with the Runthrough wire and the Samurai wire pulled back. The diagonal was wired with the Samurai wire and now both wires were crossed. A 2.0 mm compliant balloon in the diagonal was dilated to 14 atmospheres, opening up the struts. A 3.0 x 12 mm noncompliant balloon was placed in the LAD and a 2.5 x 15 mm compliant balloon was placed in the diagonal. Nominal inflations were performed in both vessels, in a kissing manner. Final angiography revealed TIMI-3 flow without dissection, perforation, or embolization. The wires were removed. Orthogonal views were obtained, revealing TIMI-3 flow without dissection, perforation, or embolization. The patient tolerated the procedure well. The guide was removed and a TR Band (Terumo) was placed over the radial artery.Discussion
 Bifurcation lesions, along with chronic total occlusion (CTOs), remain one of the more challenging lesion subsets for the interventional cardiologist. Treatment of bifurcation lesions remains a lesion subset with continued controversy over a 1- or 2-stent strategy. In addition, lesion subsets are described as left main (LM) and non-LM bifurcations. A full discussion on treatment of coronary bifurcation lesions is beyond the scope of this article; however, here we will discuss some the techniques and modifications used to treat from a radial approach.
Bifurcation lesions, along with chronic total occlusion (CTOs), remain one of the more challenging lesion subsets for the interventional cardiologist. Treatment of bifurcation lesions remains a lesion subset with continued controversy over a 1- or 2-stent strategy. In addition, lesion subsets are described as left main (LM) and non-LM bifurcations. A full discussion on treatment of coronary bifurcation lesions is beyond the scope of this article; however, here we will discuss some the techniques and modifications used to treat from a radial approach. The Medina classification1 appears to be the most commonly used nomenclature to describe bifurcation lesions. It assigns a 0 or 1 to the three segments involved (main branch or MB [proximal], MB [distal], side branch or SB) with a 1 assigned to a stenosis >50%. It does not, however, take into account bifurcation angles, lesion length, and calcification.
 There are multiple stenting techniques commonly described (crush, cullotte, T-stent, TAP, DK crush, V stent, SKS, etc). The European Bifurcation Club has put forth a formalized stenting classification (MADS) based mainly on the first stent implanted (M-main proximal stent; A-main across side first; D-distal first; S-side first).2
There are multiple stenting techniques commonly described (crush, cullotte, T-stent, TAP, DK crush, V stent, SKS, etc). The European Bifurcation Club has put forth a formalized stenting classification (MADS) based mainly on the first stent implanted (M-main proximal stent; A-main across side first; D-distal first; S-side first).2A number of trials have compared 1- and 2-stent techniques. A meta-analysis of these trials demonstrated similar outcomes with the two strategies in regards to cardiac death, target lesion revascularization (TLR), and stent thrombosis.3 However, myocardial infarction (MI) and stent thrombosis were higher in the 2-stent strategy. The NORDIC and BBC meta-analysis concluded that provisional stenting was superior to a 2-stent approach, driven mostly by the incidence of MI (periprocedural and subsequent). No significant difference was noted in target vessel revascularization (TVR).4 Subsequently, the DKCRUSH-II trial (which compared the DK crush vs provisional stenting strategies) concluded a reduced incidence of restenosis with the DK crush technique in both the MB and SB with a reduction in TLR and TVR. There was no significant difference in major adverse cardiac events (MACE) between the two techniques.5
A majority of bifurcation cases can be performed from a radial approach using a 6 or 7 French guiding catheter, particularly the large lumen guide catheters. The atherectomy devices (Rotablator [Boston Scientific], CSI, and laser atherectomy), as well as atherotomy balloons, can fit through a 6 French guide. The 7 French will allow for better support as well as better visualization, as “puffs” can be difficult in a 6 French system with a lot of gear in the vessel. The outer diameter (OD) of the guide catheter is typically the same size as a smaller sheath size (the OD of a 7 French guide is about the same as a 5 French sheath), therefore, if radial artery size is a concern, a sheathless approach or the Slender sheaths (Terumo) should be utilized.6-8
Provisional Side Branch Stenting
Typically the provisional side branch approach is done with stent, a stent and balloon, or 2 balloons in the guide; therefore, this approach can be performed in a 6 French guide. The approach is performed as follows:
The more difficult branch is wired first, followed by the second wire. Ideally, it should be advanced with minimal rotation to avoid wire wrap. The main branch is either pre-dilated or undergoes primary stent placement. The jailed wire is a safe technique, as long as the stent is not deployed over the radio-opaque part of the wire. The stent is sized to the distal main branch and after deployment, the proximal optimization technique (POT) is performed to avoid proximal stent malapposition. Therefore, it is necessary to have knowledge of the stent expansion capability. Choosing the correct platform can avoid proximal overexpansion and stent fracture. At this point, a decision is made about treating the side branch, usually based on size of the vessel (>2 mm), flow, angina and electrocardiographic changes. Koo et al demonstrated that most side branch ostial stenoses are non-significant by fractional flow reserve (FFR).9 If the side branch is treated, then kissing balloon inflation should be performed to correct stent distortion from side branch pre-dilation.
2-Stent Technique
An initial 2-stent strategy is typically considered when the SB is large (>2.5 mm) with >50% stenosis or positive FFR. The T-and-protrusion (TAP), culotte, mini-crush, or double crush techniques can be used. The original crush technique required a large guiding catheter to accommodate the 2 stents. This was modified to allow for transradial access using a balloon in the MB to crush the SB stent and then deploying the MB stent.10 The technique has further evolved into the double kiss crush. The double kiss crush is performed with 1) SB stenting with minimal protrusion in MB (1-2 mm), followed by removal; 2) MB balloon inflation (crush); 3) rewiring of the SB, dilation, and then kissing balloon inflation in the MB and SB; 4) MB stenting after removal of the SB balloon; 5) POT; 6) SB wiring and kissing balloon inflation in the MB and SB; 7) re-POT. This modified double kiss crush technique seems to have better success with final kissing balloon inflations and less repeat intervention as compared to classic crush. The culotte technique can either be done as a provisional option (first stent in MB and second stent in SB), or with the first stent from the MB to the SB (followed by POT) and then second stent deployment.11
With either technique, imaging (intravascular ultrasound [IVUS] or optical coherence tomography [OCT]) or FFR may help guide SB therapy. Imaging will also help choose appropriate stent size, expansion, apposition, and carinal coverage. As previously stated, a full discussion is beyond the scope of this article; however, Sawaya et al offer a nice review of the various techniques and provide illustrations.12
References
- Medina A, Suarez de Lezo J, Pan M. [A new classification of coronary bifurcation lesions]. Rev Esp Cardiol. 2006; 59: 183.
- Louvard Y, Thomas M, Dzavik V, et al. Classification of coronary artery bifurcation lesions and treatments: time for a consensus! Catheter Cardiovasc Interv. 2008 Feb 1; 71(2): 175-183.
- Katritsis DG, Siontis GC, Ioannidis JP. Double versus single stenting for coronary bifurcation lesions: a meta-analysis. Circ Cardiovasc Interv. 2009; 2: 409-415.
- Behan MW, Holm NR, Curzen NP, et al. Simple or complex stenting for bifurcation coronary lesions: a patient-level pooled-analysis of the Nordic Bifurcation Study and the British Bifurcation Coronary Study. Circ Cardiovasc Interv. 2011; 4: 57-64.
- Chen SL, Santoso T, Zhang JJ, et al. A randomized clinical study comparing double kissing crush with provisional stenting for treatment of coronary bifurcation lesions: results from the DKCRUSH-II (Double Kissing Crush versus Provisional Stenting Technique for Treatment of Coronary Bifurcation Lesions) trial. J Am Coll Cardiol. 2011; 57: 914-920.
- From AM, Gulati R, Prasad A, Rihal CS. Sheathless transradial intervention using standard guide catheters. Catheter Cardiovasc Interv. 2010 Dec 1;76(7):911-6. doi: 10.1002/ccd.22742.
- Kwan TW, Cherukuri S, Huang Y, et al. Feasibility and safety of 7F sheathless guiding catheter during transradial coronary intervention. Catheter Cardiovasc Interv. 2012 Aug 1; 80(2): 274-280. doi: 10.1002/ccd.24310.
- Cheaito R, Benamer H, Hovasse T, et al. Feasibility and safety of transradial coronary interventions using a 6.5-F sheathless guiding catheter in patients with small radial arteries. Catheter Cardiovasc Interv. 2015 Jul; 86(1): 51-58. doi: 10.1002/ccd.25508.
- Koo BK, Kang HJ, Youn TJ, et al. Physiologic assessment of jailed side branch lesions using fractional flow reserve. J Am Coll Cardiol. 2005 Aug 16; 46(4): 633-637.
- Lim PO, Dzavík V. Balloon crush: treatment of bifurcation lesions using the crush stenting technique as adapted for transradial approach of percutaneous coronary intervention. Catheter Cardiovasc Interv. 2004 Dec; 63(4): 412-416.
- Zhang JJ, Chen SL. Classic crush and DK crush stenting techniques. EuroIntervention. 2015; 11 Suppl V: V102-V105. doi: 10.4244/EIJV11SVA23.
- Sawaya FJ, Lefèvre T, Chevalier B, et al. Contemporary approach to coronary bifurcation lesion treatment. JACC Cardiovasc Interv. 2016 Sep 26; 9(18): 1861-1878. doi: 10.1016/j.jcin.2016.06.056.
Disclosures: Orlando Marrero reports he is a consultant for Boston Scientific. Dr. Zaheed Tai reports the following: speaker/proctor for Terumo, Spectranetics, Boston Scientific, and Abiomed.
Orlando Marrero, RCIS, MBA can be contacted at orlm8597@icloud.com.
Dr. Zaheed Tai can be contacted at zaheedtai@gmail.com.
