


The FY 2015 Financial Future: How the Cath Lab Impacts the Hospital Bottom Line
Kristin is a Decision Support Specialist with Corazon, Inc., offering a full continuum of services for the heart, vascular, neuro, and orthopedic specialties, with consulting, recruitment, interim management, and software solutions for hospitals nationwide. For more information, visit www.corazoninc.com. To reach Kristin, email ktruesdell@corazoninc.com.
Due to narrowing profit margins and increasing quality standards across the country, hospitals have been experiencing intense industry scrutiny of proper reimbursement, along with pressure to reduce costs, and both measure and achieve high-quality outcomes. It’s no wonder that cardiovascular (CV) services are at the forefront of administrators’ minds, as the specialty is one of the most significant service lines in a hospital — meaning, a CV program has the potential to bring high-volume and high-revenue procedures  to the hospital, but of course, not without high cost.
to the hospital, but of course, not without high cost.
In addition to setting overall financial goals for the hospital, administrators (at long last) have begun to set cardiovascular-specific goals that affect all levels of the organization. Indeed, the impact of these initiatives can often be felt from the administrative suite to the cath lab.
Corazon remains on the leading edge of payment updates and other important financial trends, and we believe it is imperative that hospitals are prepared for what is to come well in advance of the effective date of any changes. The following summary provides a high-level look at the upcoming fiscal year (FY)2015 changes in terms of financial and quality standards. Understanding these updates can help hospital and program leaders, along with the cath lab staff, to be aware of new criteria and how the changes, either major or minor, impact the hospital’s bottom line.
Payment updates
Inpatient payments
Under the Centers for Medicare and Medicaid Services (CMS) FY2015 hospital inpatient final rule, the market basket update is 2.9% for acute care hospitals; however, hospitals will only see a net increase of 1.4% in overall operating payment rates due to adjustments. These adverse adjustments include three items:
1. Documentation and Coding Adjustment = 0.8% decrease
o This adjustment was implemented in FY2008 when CMS converted the Diagnosis Related Groups (DRG) system from CMS-DRGs to MS-DRGs. CMS plans to continue this adjustment until $11 billion is recovered from hospitals between 2014 and 2017.
2. Productivity Adjustment = 0.5% decrease
o This adjustment was implemented in FY2012 to address economic productivity.
3. Accountable Care Act (ACA) Adjustment = 0.2% decrease
o This adjustment was implemented in FY2011 to address the needs of the Accountable Care Act and healthcare cost savings. CMS plans to continue this adjustment until FY2019 unless changes are made after the November 2016 presidential election.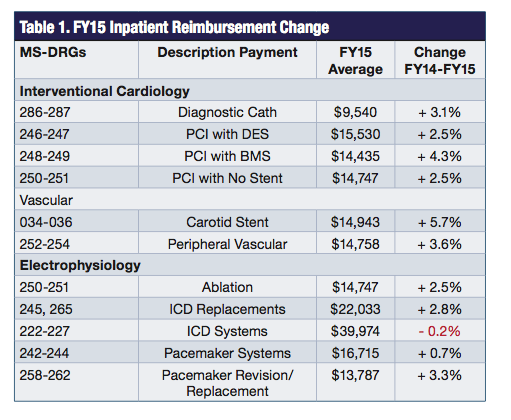
Even though hospitals lost 1.5% in operating payments due to adjustments, facilities should still realize a gain in inpatient reimbursement rates over the last fiscal year. Table 1 highlights a comparison of payments from FY2014 to FY2015 for the most common inpatient cath lab procedures.
With the exception of total ICD systems, all cath lab procedures will receive an increase for inpatient payments.
In addition to the overall increases in cath lab reimbursement, CMS also added two new MS-DRGs to further define endovascular valve replacement (EVR), otherwise known as transcatheter aortic valve implant or repair (TAVI or TAVR).
- MS-DRG 266 – Endovascular Cardiac Valve Replacement with MCC* = $52,743
- MS-DRG 267 – Endovascular Cardiac Valve Replacement without MCC = $39,602
*Major complication or comorbidity (MCC)
Previously, EVR has been embedded in standard valve MS-DRGs 216-221. But after years of technology improvements and clinical studies, along with broadening capabilities with hybrid rooms, and cardiology and cardiac surgeon collaboration, CMS has finally realized the differences in resource utilization. In FY2015, the average valve reimbursement per case is $38,096, whereas the average TAVR reimbursement per case is $46,172. By separating TAVR from standard valves, hospitals will see a gain of approximately $8,000 for a TAVR case over previous years.
Outpatient payments
Since close to half of the cath lab procedures are paid as outpatients, payments for this population must also be critically reviewed. In the proposed rule released by CMS in July 2014, big changes are coming to the outpatient payment system, particularly for percutaneous coronary intervention (PCI) procedures.
Based on the recommendation in last year’s final outpatient rule, CMS is proposing to move forward with the implementation of comprehensive Ambulatory Payment Classifications (APCs). Comprehensive APCs combine a number of procedures required to support the delivery of the primary service into a single all-inclusive payment with no additional reimbursement for affiliated procedures performed during the same operative session. Based on their proposal, CMS is making modifications to restructure all device-dependent APCs into 28 comprehensive APCs (c-APCs). The changes are intended to reflect a true prospective payment system similar to the inpatient approach.
The changes also further promote the predicted shift towards a packaged payment system in accordance with CMS’s long-term goals of encouraging efficient service delivery while reducing costs with bundled payments.
CMS has increased payment on many APCs as a result of the composite APC proposals to reflect the increase in overall costs and the elimination of separate payments for multiple procedures, additional vessels procedures, and other services. Hospitals are required to append the status indicator “J1” to specify the c-APC. Table 2 illustrates the conversion to c-APCs for PCI procedures.
There is no direct correlation from one APC to c-APC (i.e., not all drug-eluting stents are in c-APC 319 – Level III Endovascular Procedures). However, the shift to c-APCs has positively affected the reimbursement hospitals will receive for PCI stenting procedures. c-APC 0229 and c-APC 0319 are proposed to be reimbursed at $9,549 and $14,759, respectively, as compared to a range of $6,364 to $7,714 in CY2014.
In addition to the 50% increase in PCI payments, CMS is also proposing changes to the peripheral vascular and electrophysiology APC structure, which would result in an increase of 2% for peripheral cases and 10% for electrophysiology cases.
Quality updates
In order to realize maximum reimbursement potential, hospitals must adhere to the three quality standards noted below or else receive a reduction in base payments. For hospitals with poor quality performance, the CY2015 increases in reimbursement for cath-lab based procedures will easily be overshadowed by penalties.
Readmissions
The Hospital Readmissions Reduction Program requires a reduction to a hospital’s base operating DRG payment to account for excess readmissions of selected applicable conditions. The maximum reduction increased to 3% in FY2015 vs. 2% in FY2014. In addition to the three existing conditions measured (acute myocardial infarction, heart failure, and pneumonia), CMS included chronic obstructive pulmonary disease (COPD), along with total hip arthroplasty and total knee arthroplasty (THA/TKA) to be used for FY2015 and future years. CMS has also made revisions to the FY2014 algorithm to exclude planned readmissions within 30 days of discharge.
Value-based purchasing (VBP)
The estimated base operating DRG payment amount reductions for FY2015 (1.5% reduction) is the same amount available for value-based incentive payments, which is approximately $1.4 billion overall. The measures for FY2015 were finalized in previous 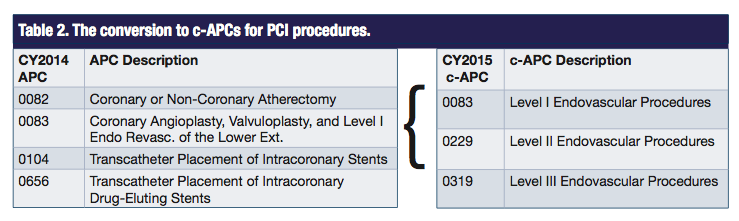 rulings, which include 19 measures. CMS also made final and proposed rulings for the future VBP program in FY2017 and beyond, which includes a reduction of 1.75% in FY2016 and 2.0% in FY2017.
rulings, which include 19 measures. CMS also made final and proposed rulings for the future VBP program in FY2017 and beyond, which includes a reduction of 1.75% in FY2016 and 2.0% in FY2017.
Hospital-acquired conditions (HAC)
As part of the Affordable Care Act, a 1% reduction in payment is made to hospitals whose ranking is in the lowest-performing quartile. CMS estimates that approximately 760 hospitals will be subject to the reduction, which equates to approximately $330 million. Each year, Medicare will reassess hospitals and decide which should be penalized. While the amount of the penalty does not change, the criterion Medicare uses expands. In October 2015, Medicare will add rates of surgical site infections to its analysis, and in October 2016, it will include incident rates of two germs that are resistant to antibiotic treatment.
Corazon recommends that hospitals pay close attention to quality data for the current year, especially because as standards shift, current outcome trends will help to determine whether a hospital will be penalized or incentivized in the future.
Other notable updates
Two-midnight rule
As published in the final inpatient rule, Recovery Audit Contractor (RAC) enforcement of the two-midnight rule has been delayed until March 31, 2015. Under the two-midnight rule, a patient qualifies as an inpatient admission if the patient stays at the hospital for at least two midnights. Although the two-midnight rule was finalized in the FY2014 ruling, it was initially delayed until October 2014 due to extreme resistance.
Corazon advocates that hospitals evaluate the financial impact of the two-midnight rule and understand the details of patients with one-day length of stays. Corazon’s proven model calculates the impact of this rule not only from a revenue standpoint, but also from the cost of resources. For example, a hospital with a total of 100 cases with length of stays between 1.0 – 1.9 days can expect a decrease in payments of approximately $500,000 if the two-midnight rule is implemented.
Hospital charge transparency
As part of the Affordable Care Act, this is the first year that hospitals are required to make public a list of their standard charges. This is a huge step towards greater consumer transparency; unfortunately, CMS has not published guidelines on how to make the list public. Regardless, hospitals should be prepared for consumers to price shop healthcare, particularly those with high-deductible health plans. We recommend hospitals look at each contracted rate and complete a competitive pricing exercise to discover how charges compare to that of competitors.
Cath lab staff impact
The final rulings went into effect October 1, 2014 for the inpatient payment system and January 1, 2015 for the outpatient payment system. Savvy hospital and program leaders should always be looking at the reimbursement for the cardiovascular service line, as changes to this specialty and included sub-specialties can have a big impact on the bottom line.
Particularly, staff in the cardiac cath lab can play a major role in achieving — or hindering the ability to achieve — the highest possible reimbursement for their hospital. For instance, six of 19 measures evaluated in the VBP program are associated with performance in the cath lab setting or post-procedure (AMI-7a, AMI-8a, HF-1, HCAHPS, MORT-30-AMI, MORT-30-HF). Therefore, to assist in contributing to a positive reimbursement reward, members of the cath lab team will need to heavily focus on improving quality, patient satisfaction, and outcomes.
Based on this summary, Corazon recommends all hospitals pay close attention to the financial and quality performance of the CV service line, and the cath lab in particular. Though many of the FY2015 changes are positive, implementing efforts to maintain cardiovascular profit margins can favorably impact the overall organizational bottom line. An initial look at financial, operational, and quality processes can reveal areas needing improvement and/or areas of opportunity. Any potential opportunity to improve performance should be considered a priority.
