


Flaring of Ostial Coronary Stent Using Flash Ostial Balloon for Aorto-Ostial Coronary Disease in a Right Coronary Artery Chronic Total Occlusion Intervention
_0.jpg) The anatomic nature of percutaneous stenting of aorto-ostial lesions remains an angiographic challenge for interventional cardiologists. There are greater than 300,000 aorto-ostial stenting procedures performed worldwide each year.1-2 Herein, we present an interesting case of an aorto-ostial percutaneous coronary intervention using the Flash Ostial Balloon of a right coronary artery chronic total occlusion via a retrograde approach.
The anatomic nature of percutaneous stenting of aorto-ostial lesions remains an angiographic challenge for interventional cardiologists. There are greater than 300,000 aorto-ostial stenting procedures performed worldwide each year.1-2 Herein, we present an interesting case of an aorto-ostial percutaneous coronary intervention using the Flash Ostial Balloon of a right coronary artery chronic total occlusion via a retrograde approach.
Case
 A 50-year-old male with established multivessel coronary artery disease complicated by a prior myocardial infarction, known chronic total occlusions (CTO) of his left circumflex and right coronary arteries (RCA), chronic angina with Canadian Cardiovascular Society class 3 symptoms, exertional dypnea, chronic systolic heart failure, and systemic hypertension presented for attempted percutaneous coronary intervention to his dominant RCA CTO after failed optimization of medical therapy.
A 50-year-old male with established multivessel coronary artery disease complicated by a prior myocardial infarction, known chronic total occlusions (CTO) of his left circumflex and right coronary arteries (RCA), chronic angina with Canadian Cardiovascular Society class 3 symptoms, exertional dypnea, chronic systolic heart failure, and systemic hypertension presented for attempted percutaneous coronary intervention to his dominant RCA CTO after failed optimization of medical therapy.
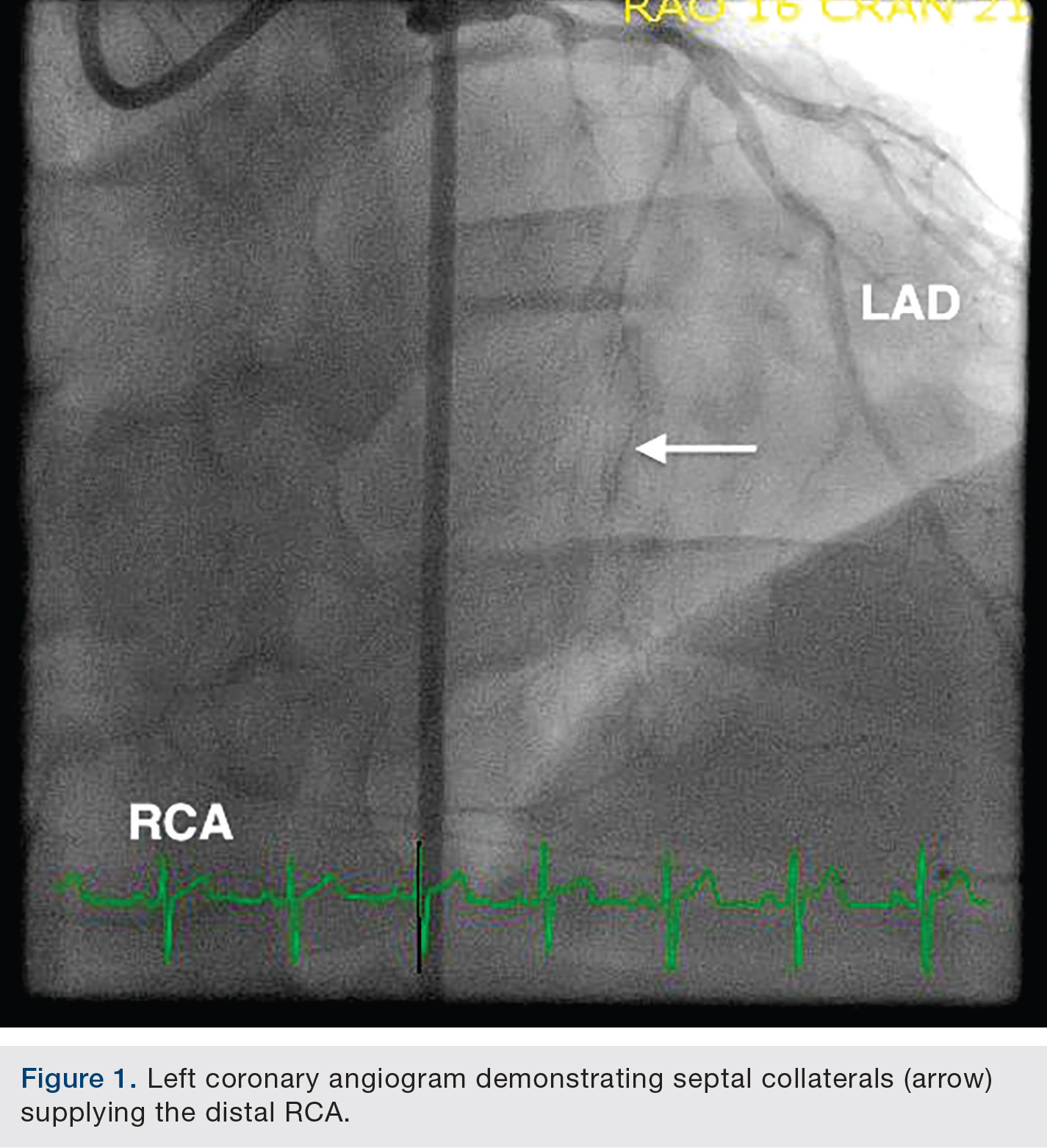
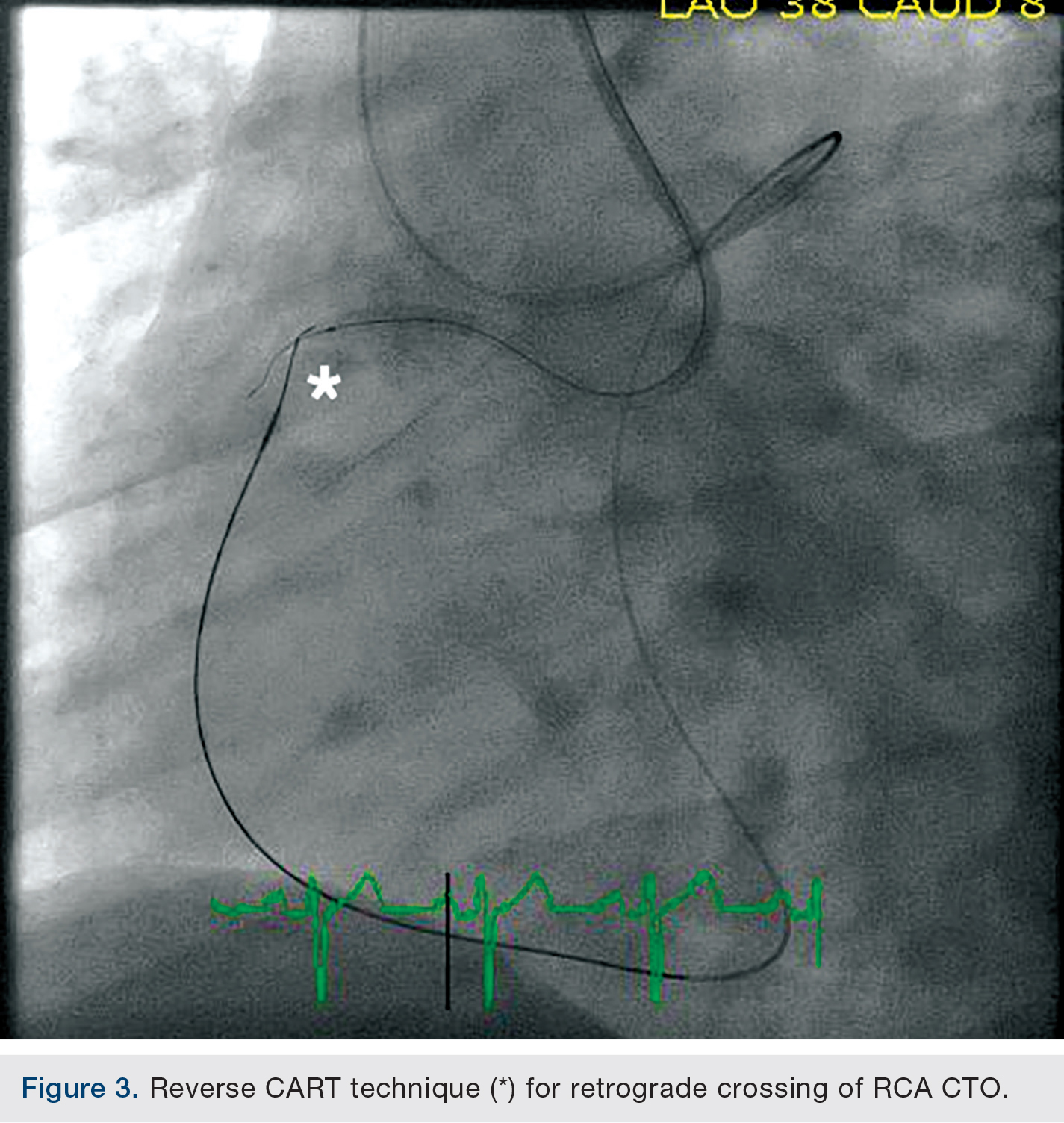
The patient underwent bilateral femoral artery access with 8 French sheath placement. An 8 French Extra Back Up Launcher 4.0 guide catheter (Medtronic) was positioned in the left coronary system and a 7 French Amplatz Left-1(AL-1) (Medtronic) positioned in the RCA ostium. The proximal RCA CTO cap was very ambiguous, with septal collaterals supplying the distal RCA (Figure 1). A retrograde approach via well-developed septal artery perforators was accessed with an Asahi Fielder XT wire (Abbott Vascular) and a 150cm Corsair micro-catheter (Asahi Intecc) (Figure 2). 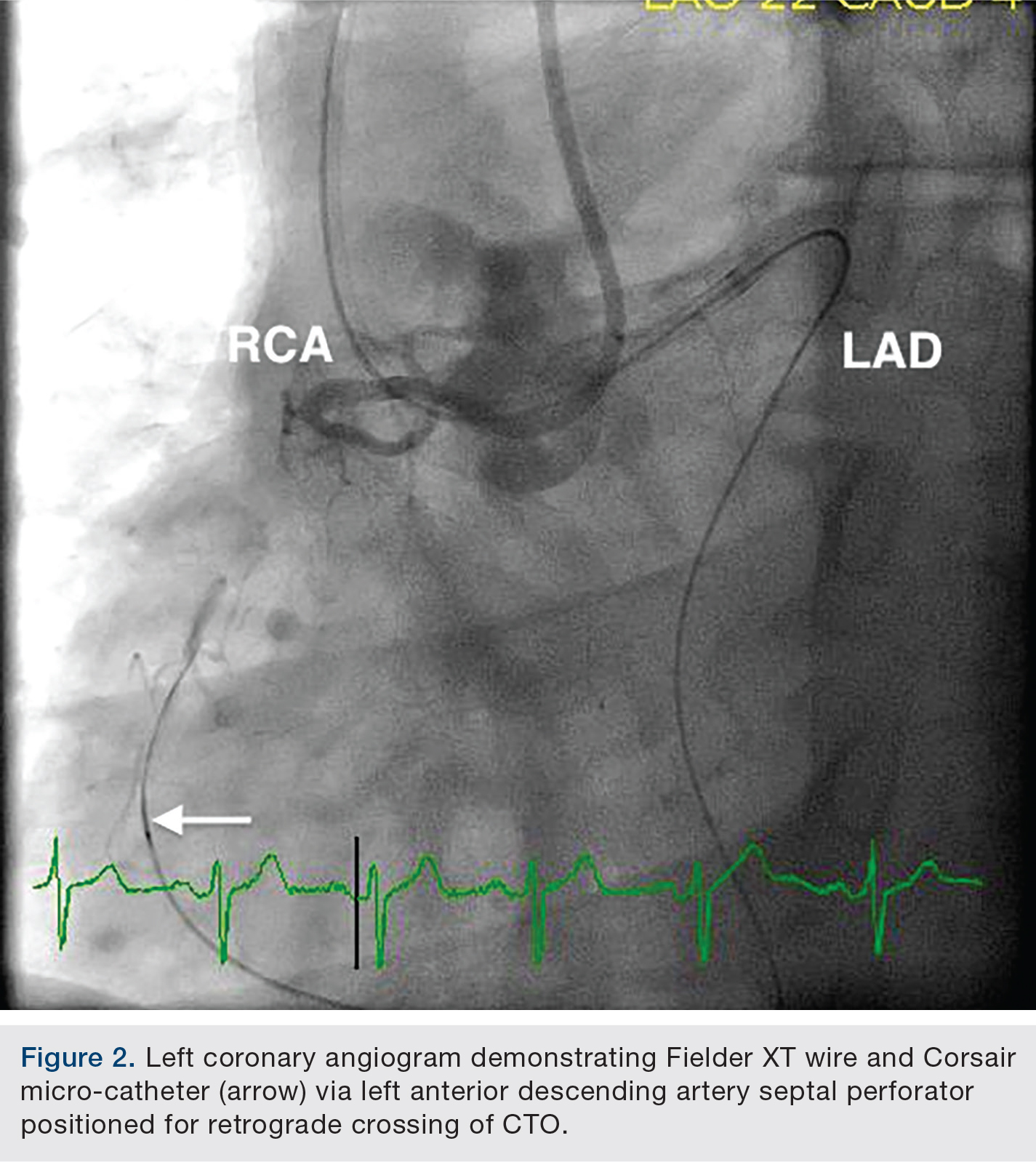 Once the wire was advanced all the way to the proximal CTO in the RCA, the proximal cap proved to be difficult to cross and a reverse controlled antegrade and retrograde subintimal tracking (CART) technique was utilized (Figure 3). This entailed creating a dissection plane channel proximally in the RCA using a small 1.25mm over-the-wire balloon and a Confianza Pro 12 wire (Abbott Vascular) that was advanced proximally from the RCA AL-1 guide in an antegrade maneuver. The septal Fielder XT wire was then exchanged over the Corsair for an Asahi Miracle Bros 4.5 wire (Abbott Vascular), advanced through the calcific proximal cap and into the RCA AL-1 guide, and externalized via the RCA guide.The RCA lesion was then pre-dilated and stented with a total of four drug-eluting stents in overlapping fashion, up to but short of the ostium.
Once the wire was advanced all the way to the proximal CTO in the RCA, the proximal cap proved to be difficult to cross and a reverse controlled antegrade and retrograde subintimal tracking (CART) technique was utilized (Figure 3). This entailed creating a dissection plane channel proximally in the RCA using a small 1.25mm over-the-wire balloon and a Confianza Pro 12 wire (Abbott Vascular) that was advanced proximally from the RCA AL-1 guide in an antegrade maneuver. The septal Fielder XT wire was then exchanged over the Corsair for an Asahi Miracle Bros 4.5 wire (Abbott Vascular), advanced through the calcific proximal cap and into the RCA AL-1 guide, and externalized via the RCA guide.The RCA lesion was then pre-dilated and stented with a total of four drug-eluting stents in overlapping fashion, up to but short of the ostium.
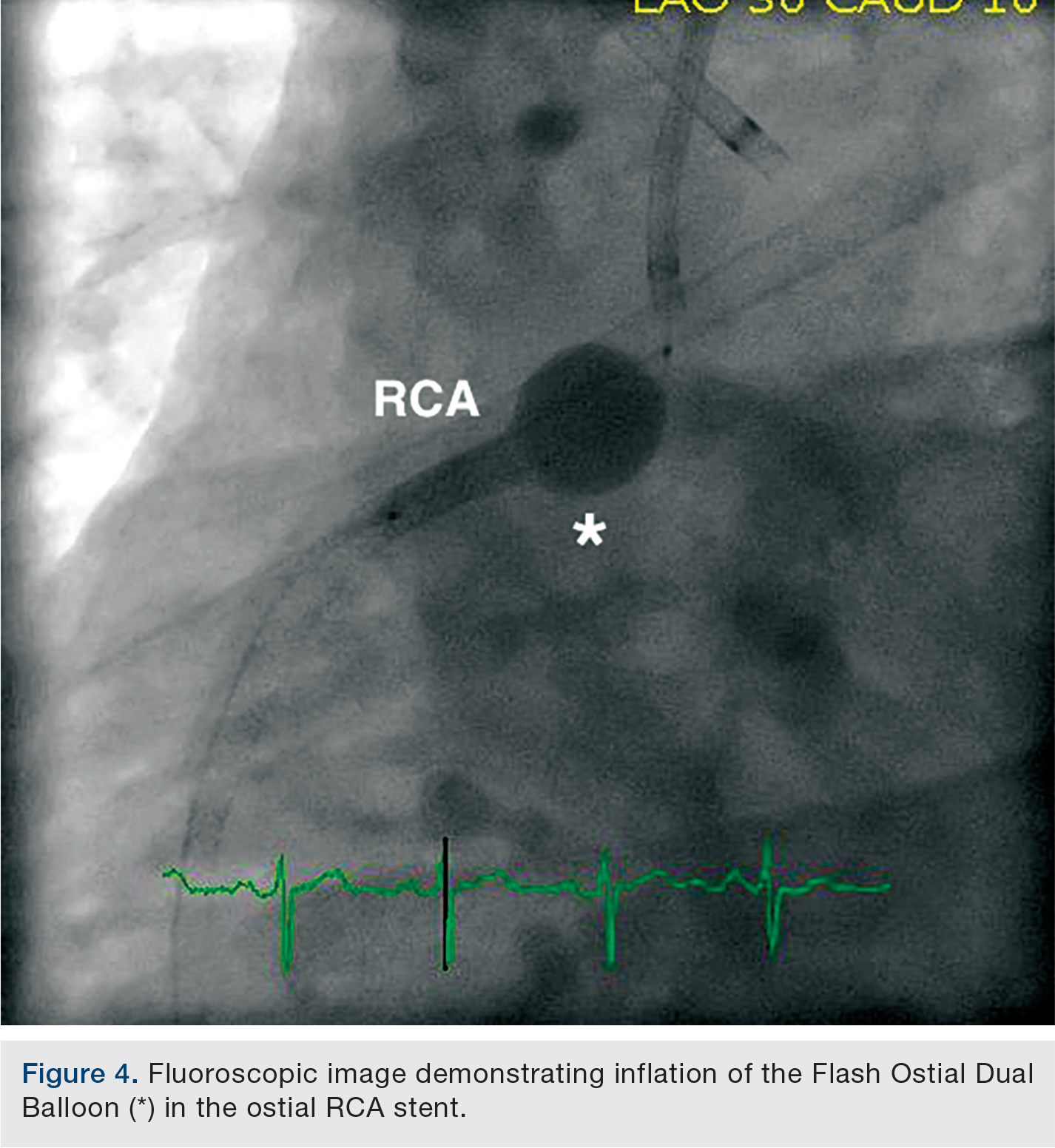
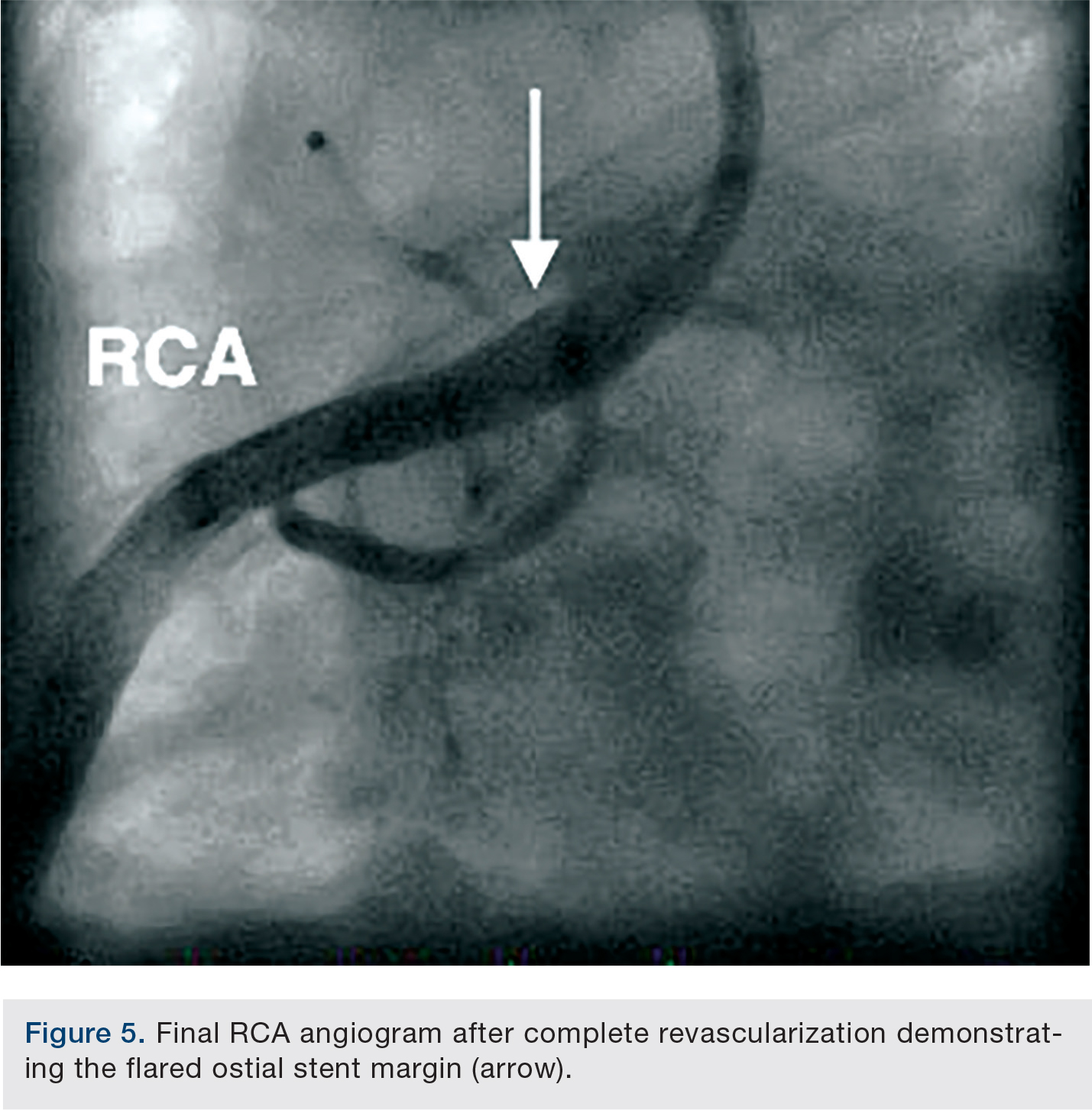
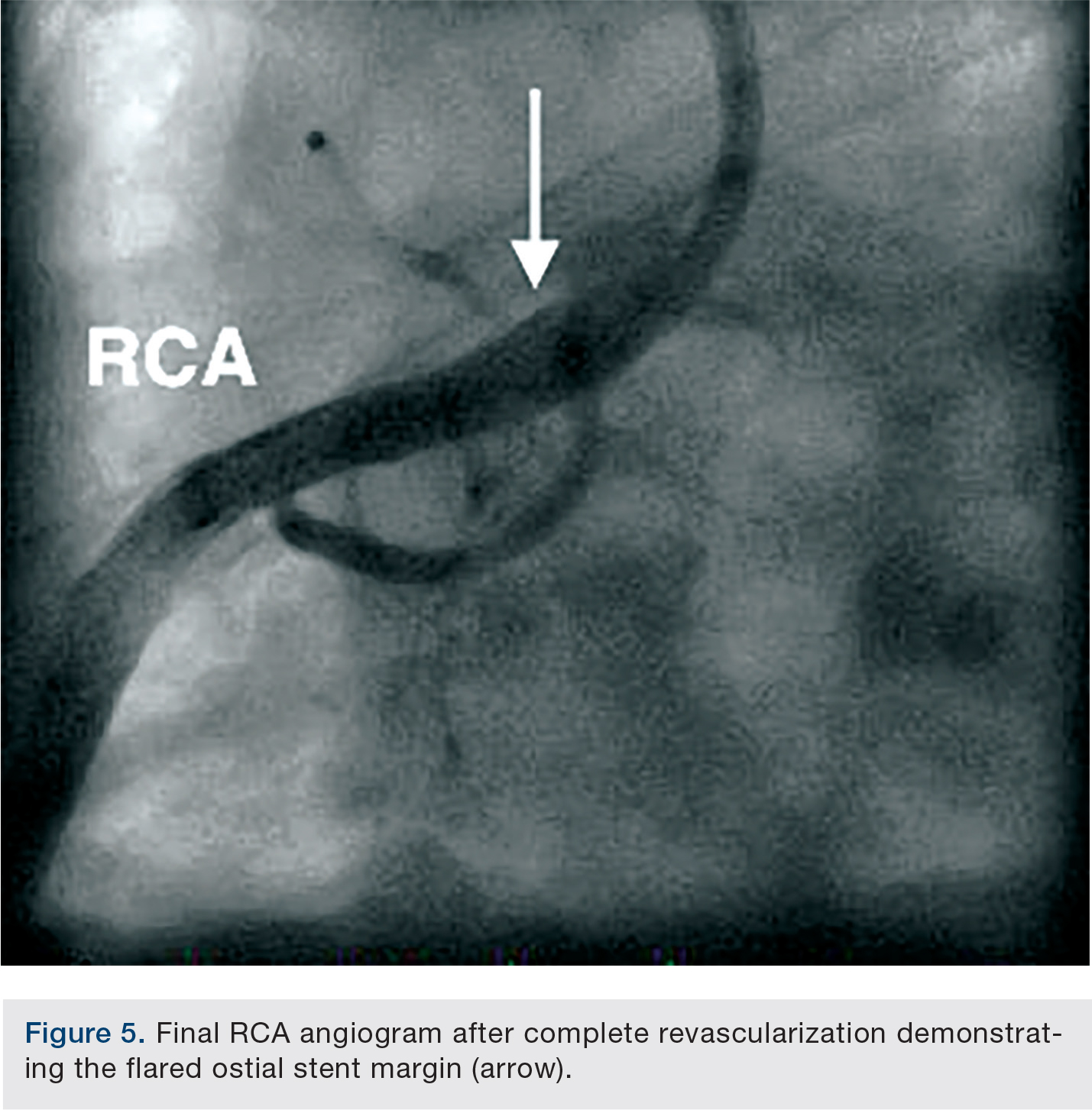
A short ostial 4.0 x 16mm Promus Premier stent (Boston Scientific) was deployed with 1-2mm extending into the aorta. A 4.0 x 14mm Flash Ostial Dual Balloon coronary angioplasty catheter (AccessClosure) was then inflated in two sequential maneuvers: first, the elongated body of the non-compliant balloon was inflated to 14 atmospheres, and second, the spherical flash ostial portion of the balloon was inflated with 0.9cc of contrast medium for a total of 3 seconds in order to flare the ostial stent margin to the aorta (Figure 4). The final RCA angiogram revealed brisk antegrade flow and an appropriately flared ostial stent margin well apposed to the aortic wall (Figure 5). The patient’s femoral arteries were sealed with 8 French Angio-Seal (St. Jude Medical) vascular closure devices and the patient was discharged the following day in stable condition after being loaded with dual antiplatelet therapy.
 Discussion
Discussion
There are greater than 300,000 aorto-ostial vessel percutaneous stenting procedures performed worldwide each year.1-2 Although aorto-ostial lesions represent a numerically small volume of procedures (only about 7-8% of all intra-coronary stenting interventions), they represent more than 90% of mesenteric and renal artery endovascular interventions.1,3
 Previous studies have reported low technical success rates of aorto-ostial interventions, presumed to be related to the geometric angle, stent misplacement, or even geographic miss, which has been reported to be greater than 50% even among experienced interventional cardiologists when using traditional angiographic guidance.2-8 This translates into longer procedure and fluoroscopy times, relatively high complication rates, increased target vessel restenosis rates, reduced event-free survival and increased major adverse cardiac event occurrences.4-8 Subsequently, poor stent coverage of the diseased vessel, suboptimal forward flow dynamics, and difficulty re-accessing the target vessel after malpositioned ostial stents lead to a continuous and cumulative problem for re-interventions during future procedures.5-8
Previous studies have reported low technical success rates of aorto-ostial interventions, presumed to be related to the geometric angle, stent misplacement, or even geographic miss, which has been reported to be greater than 50% even among experienced interventional cardiologists when using traditional angiographic guidance.2-8 This translates into longer procedure and fluoroscopy times, relatively high complication rates, increased target vessel restenosis rates, reduced event-free survival and increased major adverse cardiac event occurrences.4-8 Subsequently, poor stent coverage of the diseased vessel, suboptimal forward flow dynamics, and difficulty re-accessing the target vessel after malpositioned ostial stents lead to a continuous and cumulative problem for re-interventions during future procedures.5-8
 The anatomic challenges of percutaneous stenting of aorto-ostial stenosis create an arduous task for interventional cardiologists. The angle of ostial vessel anatomy in relation to the aorta is one of the main complexities of this specific type of stenosis. It is not a perpendicular 90-degree angle, but rather a multi-dimensional tapering of the vessel, constituting the geometric angle.4 The geometric angle has been delineated using computed tomography coronary angiography using 2-dimensional and 3-dimensional reconstructions, which have demonstrated ostial bifurcation of vessels as a tapering or funneling of the junction of the parent vessel (aorta) into the daughter vessels (right and left coronary arteries) as branching tributaries.4 This proposed geometric mismatch becomes the nidus for much of the subsequent difficulties in the percutaneous management of ostial vessel stenoses.4
The anatomic challenges of percutaneous stenting of aorto-ostial stenosis create an arduous task for interventional cardiologists. The angle of ostial vessel anatomy in relation to the aorta is one of the main complexities of this specific type of stenosis. It is not a perpendicular 90-degree angle, but rather a multi-dimensional tapering of the vessel, constituting the geometric angle.4 The geometric angle has been delineated using computed tomography coronary angiography using 2-dimensional and 3-dimensional reconstructions, which have demonstrated ostial bifurcation of vessels as a tapering or funneling of the junction of the parent vessel (aorta) into the daughter vessels (right and left coronary arteries) as branching tributaries.4 This proposed geometric mismatch becomes the nidus for much of the subsequent difficulties in the percutaneous management of ostial vessel stenoses.4
The Flash Ostial Balloon (Access Closure) is a novel ostial balloon designed for post-dilation balloon angioplasty. The design consists of a long cylindrical balloon (sizes of 3.5-5.0mm) with a second larger-diameter spherical balloon abutting the proximal shaft. The dual balloon design enables stent wall apposition after post-dilation, and stability during angioplasty by conforming to the target vessel ostium during stent post-dilatation and angioplasty. This allows the proximal stent struts to be flared against the aortic wall. The Flash Ostial Dual Balloon catheter is currently available for both coronary and peripheral aorto-ostial vascular interventions.
Herein, we describe a complex coronary CTO intervention involving the aorto-coronary ostium that was managed using the Flash Ostial Balloon for flaring the ostial stent.
References
- Rissanen V. Occurrence of coronary ostial stenosis in a necropsy series of myocardial infarction, sudden death, and violent death. Brit Heart J. 1975; 37: 182-191.
- Fischell TA, Saltiel FS, Foster MT, et al. Initial clinical experience using an ostial stent positioning system (Ostial Pro™) for the accurate placement of stents in the treatment of coronary aorto-ostial lesions. J Invasive Cardiol. 2009; 21: 53-59.
- Darabian S, Amirzadegan AR, Sadeghian H, et al. Ostial lesions of left main and right coronary arteries: Demographic and angiographic features. Angiology. 2008; 59: 682-687.
- Aviram G, Shmilovich H, Finkelstein A, et al. Coronary ostium — straight tube or funnel-shaped? A computerized tomographic coronary angiography study. Acute Cardiac Care. 2006; 8: 224-228.
- Cook S, Eshtehardi P, Kalesan B, et al. Impact of incomplete stent apposition on long-term clinical outcome after drug-eluting stent implantation. EHJ. 2012; 33: 1334-1343.
- Dishmon D, Elhaddi A, Packard K, et al. High incidence of inaccurate stent placement in the treatment of coronary aorto-ostial disease. J Invasive Cardiol. 2011; 23(8): 322-326.
- Ko E, Natsuaki M, Toyofuku M, et al. Sirolimus-eluting stent implantation for ostial right coronary artery lesions: five-year outcomes from the j-Cypher registry. Cardiovasc Interv Ther. 2014 Jul; 29(3): 200-208. doi: 10.1007/s12928-013-0236-2.
- Fujii K, Carlier S, Mintz G, et al. Stent under-expansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: an intravascular ultrasound study. J Am Coll Cardiol. 2005 Apr 5; 45(7): 995-998.
- Mathias DW, Mooney JF, Lange HW, et al. Frequency of success and complications of coronary angioplasty of a stenosis at the ostium of a branch vessel. Am J Cardiol. 1991; 67: 491-495.
- Horlitz M, Amin FR, Sigwart U, Clague JR. Coronary stenting of aorto-ostial saphenous vein graft lesions. J Invasive Cardiol. 2006; 68: 901-906.
Disclosure: Dr. Waggoner reports no conflicts of interest regarding the content herein. Dr. Kovach reports he is a consultant for Boston Scientific and Medtronic. Dr. George reports he is a consultant for Boston Scientific and Abbott.
The authors can be contacted via Dr. Jon George at georgej@deborah.org.
