A Complex CTO via the Radial Approach
The following case is the third in a series of transradial-focused reports directed by section editor Dr. Samir Pancholy. This case series is supported by an educational grant from Medtronic.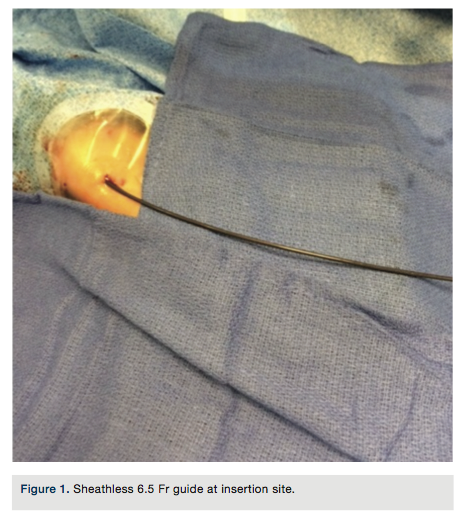
Case report
The patient is a frail 76-year-old with a prior history of a coronary stent in 2007. He is a diabetic, hypertensive smoker who recently developed crescendo angina. His physical examination was unremarkable except for a body mass index 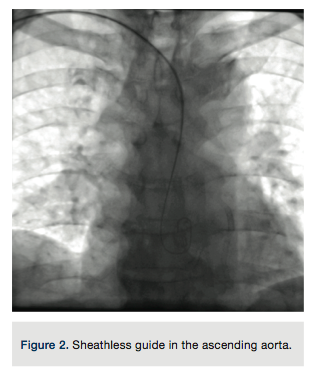 measurement of 22. A baseline electrocardiogram (EKG) had no q waves and only non-specific ST-T wave changes. A rest echocardiogram demonstrated normal wall motion. He was on beta-blockers, ACE inhibitors, a statin, and aspirin. A long-acting nitrate was added to his medical therapy after a diagnostic angiogram revealed a total obstruction of the left circumflex in the previously stented segment. The patient returned after several weeks, still having chest discomfort when engaging in mild physical activity.
measurement of 22. A baseline electrocardiogram (EKG) had no q waves and only non-specific ST-T wave changes. A rest echocardiogram demonstrated normal wall motion. He was on beta-blockers, ACE inhibitors, a statin, and aspirin. A long-acting nitrate was added to his medical therapy after a diagnostic angiogram revealed a total obstruction of the left circumflex in the previously stented segment. The patient returned after several weeks, still having chest discomfort when engaging in mild physical activity.
Based on his limiting symptoms, a plan to attempt treatment of the total left circumflex obstruction was discussed with the patient, who agreed to proceed to an attempted angioplasty. Due to his small body size and associated increased bleeding 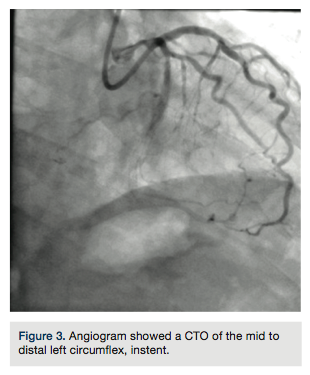 risk, a radial approach was chosen.
risk, a radial approach was chosen.
A 4 French (Fr) Glidesheath (Terumo Corporation) was inserted in the right radial artery and a vasodilator cocktail of 2.5 mg verapamil and 100 micrograms of nitroglycerin were given via the sheath. Since this was to be a planned chronic total occlusion (CTO) intervention, 5,000 units of heparin were given via an intravenous route. The 4 Fr introducer was exchanged out for a 6.5 PB4.0 Asahi sheathless guide (Asahi Intecc) (Figures 1-2). A control angiogram of the left coronary (Figure 3) reveals a total occlusion in the distal circumflex artery.
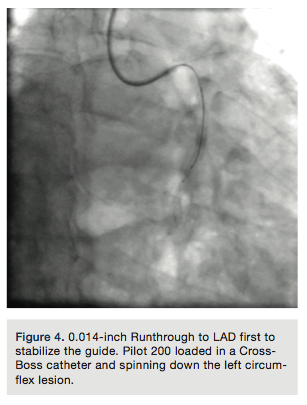
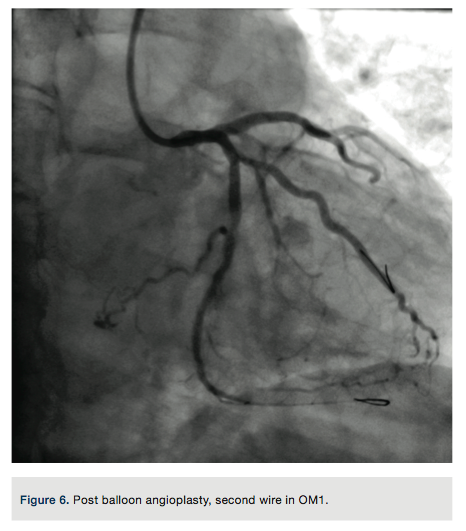
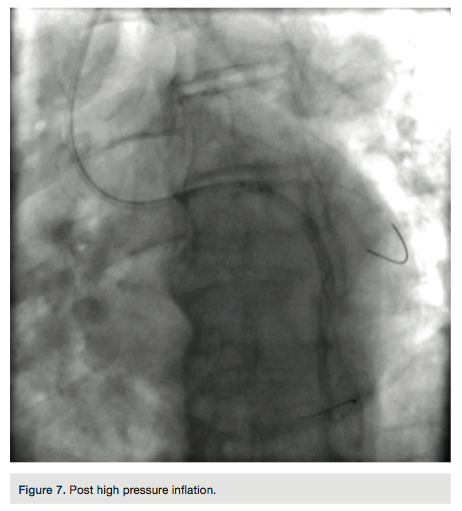
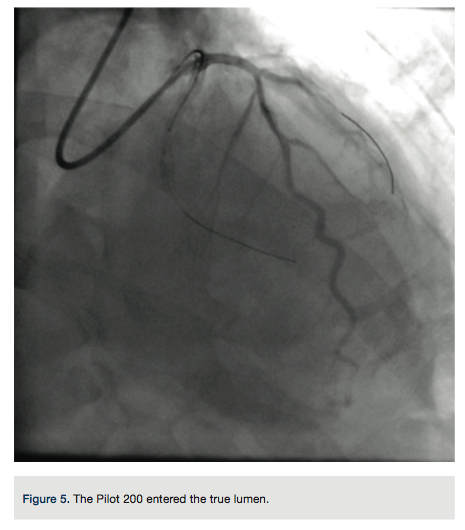
A Pilot 200 wire (Abbott Vascular) was loaded in a CrossBoss catheter (Boston Scientific) and advanced into the circumflex artery. The CrossBoss was slowly advanced, using the Pilot wire to redirect the device to remain as close to the lumen as possible. Once past the total obstruction, the Pilot 200 wire was used to re-enter the distal circumflex (Figures 3-4). A balloon dilation with a 1.5 mm x 20 mm long balloon was performed at 12 atmospheres (atm) followed by a 2.5 mm x 20mm balloon at 12 atm. A Runthrough wire (Terumo) was placed in the first marginal and stenting of the circumflex was performed using a 2.5 mm x 38 mm Promus Premier stent (Boston Scientific) overlapped with a 3.0 mm x 24 mm Promus Premier stent. High-pressure inflation in the entire stented segment was performed using a 3.0 mm balloon. The segment proximal to the first obtuse marginal was dilated to high pressure using a 3.25 mm balloon (Figures 5-7). A good angiographic result was seen (Figure 8).
When seen back in the office at 1 week, the patient reported relief of symptoms and the right radial pulse was present. At the last office visit 6 months post procedure, the patient remains free of angina.