


Complex Bypass Graft Anatomy: Deciphering the Puzzle
 Note: This article has accompanying videos referenced in the text.
Note: This article has accompanying videos referenced in the text.
Deciphering complex coronary anatomy can be challenging, particularly in post-CABG patients. CABG surgery using conduits with multiple distal anastomoses has the potential to lead to graft failure, largely related to bypass graft flow dynamics.1,2 Recognizing conventional, as well as anomalous, coronary artery patterns in specific angiographic views is paramount in understanding elaborate graft anatomies. We present herein an interesting case of complex bypass graft angiography with multiple anastamoses supplying the entire myocardium.
Case
 A 75-year-old male with history of coronary artery disease, prior 3-vessel coronary artery bypass graft surgery (CABG) in 2001, peripheral arterial disease, hypertension, and prior tobacco use was admitted for elective cardiac catheterization due to progressive symptoms of chest pain with an abnormal nuclear stress test. The details of his CABG surgery, performed at an outside institution, were unknown at the time of his coronary angiography.
A 75-year-old male with history of coronary artery disease, prior 3-vessel coronary artery bypass graft surgery (CABG) in 2001, peripheral arterial disease, hypertension, and prior tobacco use was admitted for elective cardiac catheterization due to progressive symptoms of chest pain with an abnormal nuclear stress test. The details of his CABG surgery, performed at an outside institution, were unknown at the time of his coronary angiography.
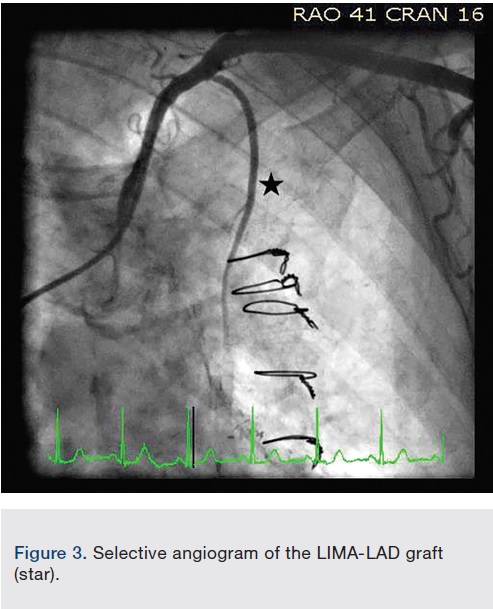
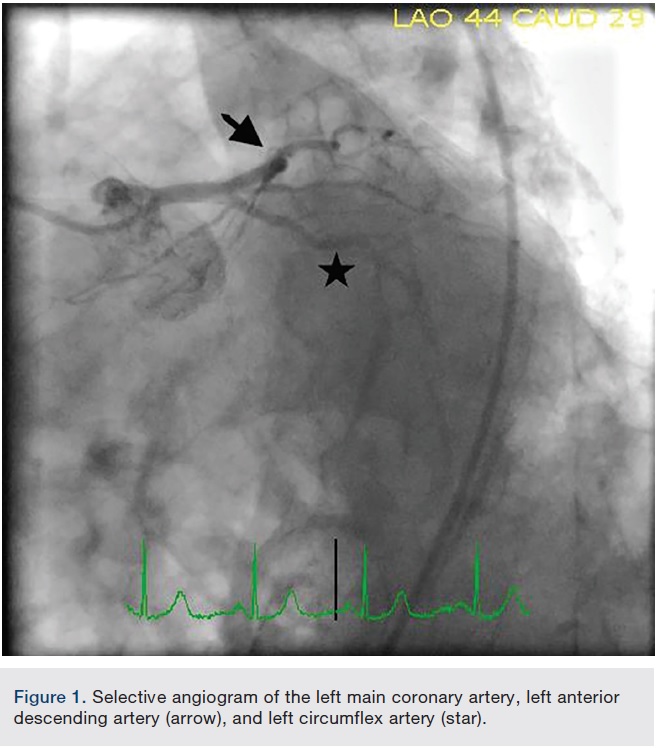
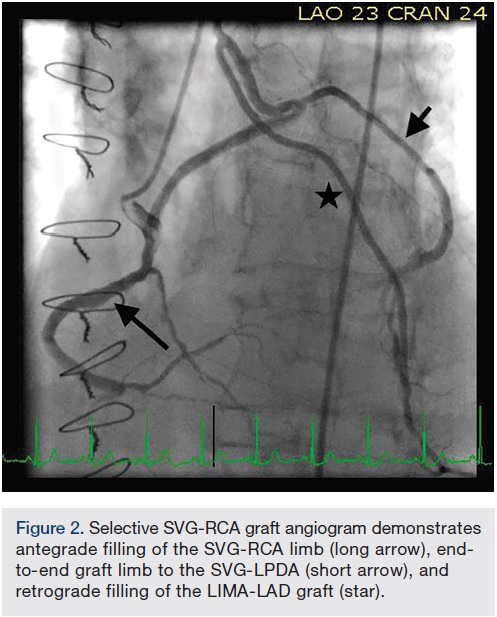 Right common femoral artery access was obtained, and selective coronary artery and bypass graft angiography performed. The right coronary artery (RCA) was proximally occluded (Video 1). The left main coronary artery demonstrated mild disease, with 100% occlusions of the mid left anterior descending (LAD) and left circumflex (LCX) coronary arteries (Figure 1, Video 2). Selective saphenous vein graft (SVG) to distal RCA angiography demonstrated a patent graft with a side-to-end anastomosis to the RV marginal artery, and distal anastomosis to the posterior lateral artery, which had mild disease (Figure 2, Video 3). Interestingly, there was also an end-to-end vein graft limb, originating mid graft, extending to an SVG to left posterior descending artery (LPDA). The SVG-LPDA graft was widely patent, and originated from the left internal mammary artery graft (LIMA) to LAD. The LIMA-LAD arose from the left subclavian artery, and had mild disease in the distal native LAD (Figure 3, Video 4).
Right common femoral artery access was obtained, and selective coronary artery and bypass graft angiography performed. The right coronary artery (RCA) was proximally occluded (Video 1). The left main coronary artery demonstrated mild disease, with 100% occlusions of the mid left anterior descending (LAD) and left circumflex (LCX) coronary arteries (Figure 1, Video 2). Selective saphenous vein graft (SVG) to distal RCA angiography demonstrated a patent graft with a side-to-end anastomosis to the RV marginal artery, and distal anastomosis to the posterior lateral artery, which had mild disease (Figure 2, Video 3). Interestingly, there was also an end-to-end vein graft limb, originating mid graft, extending to an SVG to left posterior descending artery (LPDA). The SVG-LPDA graft was widely patent, and originated from the left internal mammary artery graft (LIMA) to LAD. The LIMA-LAD arose from the left subclavian artery, and had mild disease in the distal native LAD (Figure 3, Video 4).
References
- Morakhia J, Ramachandran P, Sanjeeva NC, Thakkar A. Coronary steal or large collateral? Three cases of graft failure in sequential and composite grafts. BMJ Case Rep. 2014 Nov 12; 2014. pii: bcr2014206932. doi: 10.1136/bcr-2014-206932.
- Glineur D, Hanet C. Competitive flow in coronary bypass surgery: is it a problem? Curr Opin Cardiol. 2012 Nov; 27(6): 620-628.
*Dr. Jon C. George is now Cath Lab Director, Einstein Medical Center, Philadelphia, Pennsylvania.
Disclosure: Dr. Vincent Varghese reports no conflicts of interest regarding the content herein. Dr. George reports he is a consultant for Abbott, Atrium/Maquet, Boston Scientific, Edwards, and Medtronic.
The authors can be contacted via Dr. Jon George at jcgeorgemd@gmail.com.
